

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The evolving trends in stroke care are critical for the strategic planning of health policies, effective resource allocation, and guiding future research. While international stroke organizations have periodically updated stroke statistics, the most comprehensive report available covers only up to 2020.12 These updates have not addressed changes following the latest stroke guidelines,345 nor have they considered the impact of the coronavirus disease 2019 (COVID-19) pandemic, which significantly disrupted stroke care systems during 2020–2021.6 This highlights the need for current, real-world data to evaluate the effects of such disruptions and to guide adjustments in patient care strategies.
This study aimed to provide updated statistics for 2022, using data from a nationwide, prospective stroke registry. It explored various aspects including demographics, risk factors, clinical symptoms, treatment approaches during the hyperacute and acute phases, and patient outcomes. By doing so, it seeks to provide valuable insights for stroke care professionals, researchers, and policy-makers, contributing to the enhancement of stroke care quality.
ABOUT THESE STATISTICS
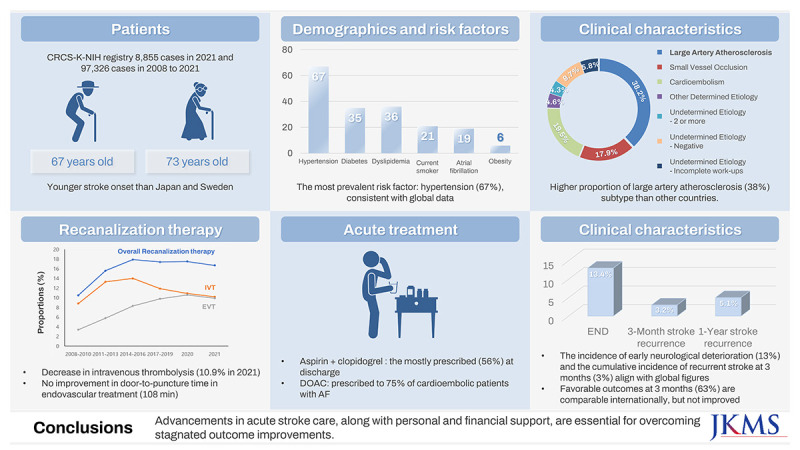
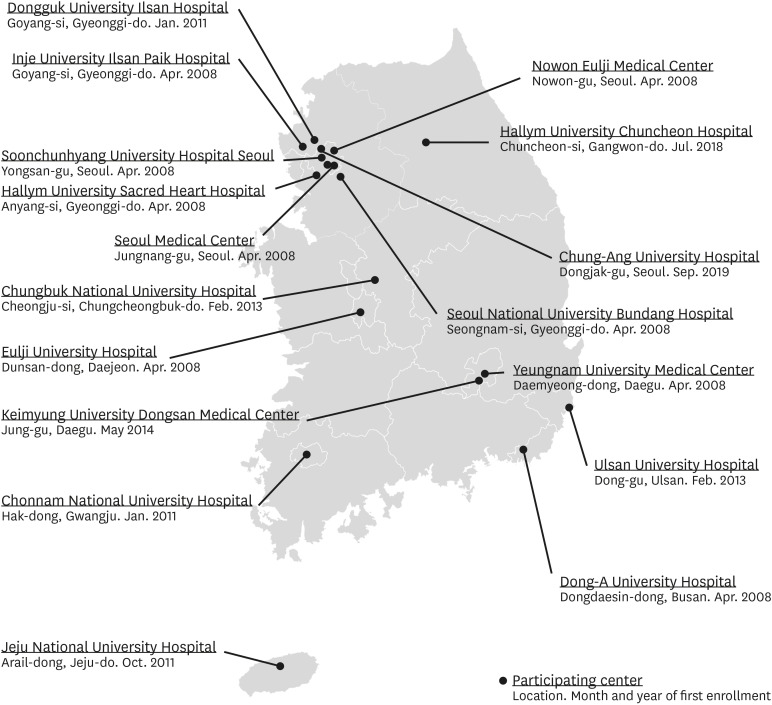
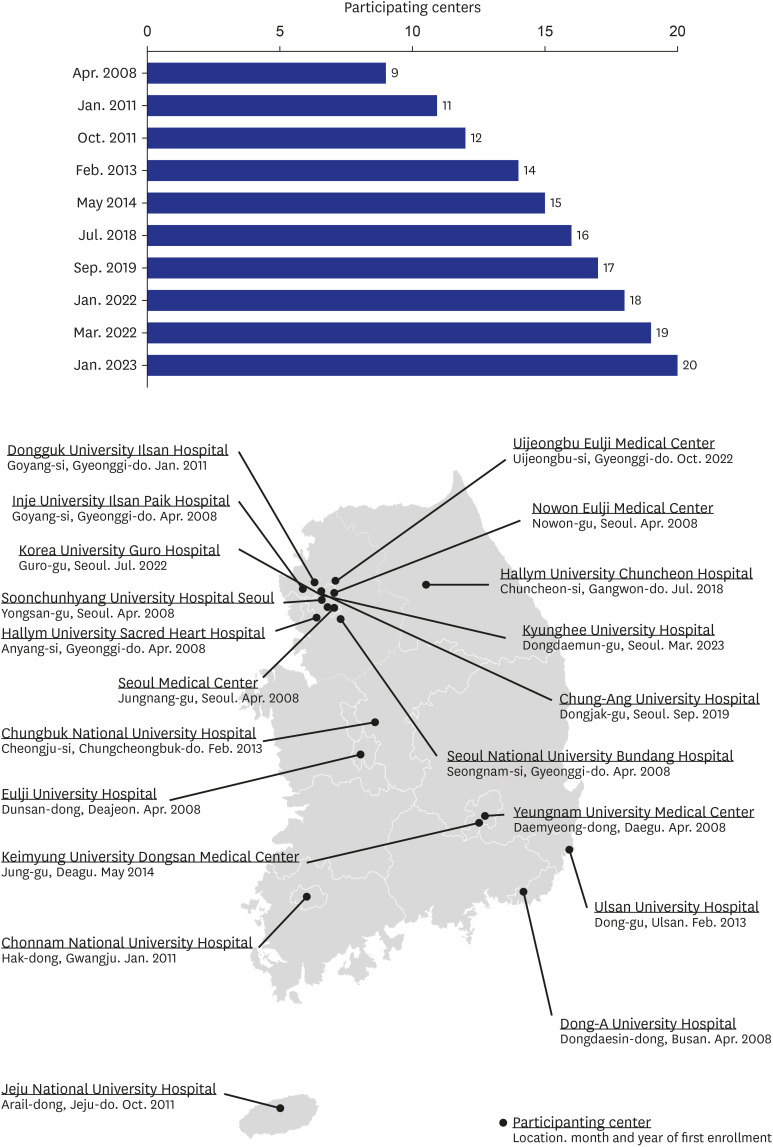
The Clinical Research Collaborations for Stroke in Korea-National Institute for Health (CRCS-K-NIH), established in 2008, is a nationwide, multicenter, prospective stroke registry. It aims to develop national guidelines, enhance the quality of stroke care, and reduce the stroke burden in Korea.78 Details on the registry’s history are provided in the Glossary under “History of the CRCS-K-NIH Registry” (Appendix 1). As of 2021, it encompasses 17 stroke centers across South Korea (Fig. 1) and compiles comprehensive clinical data on patients admitted with acute stroke or transient ischemic attack (TIA), as detailed in Supplementary Table 1. Generally, patients with hemorrhagic stroke are admitted to neurosurgical departments, therefore, the focus here is primarily on acute ischemic stroke (AIS) and TIA. A portion of patients with ischemic stroke are admitted to neurosurgical departments in Korea, especially in small or mid-sized hospitals. This subset of patients was not included in our study, which may limit the generalizability of our findings across all stroke care settings in the country. Future studies could aim to incorporate this data to provide a more comprehensive analysis of stroke care in South Korea.9
Data integrity is ensured through a protocol requiring initial registration within 24 hours of hospital admission, followed by de-identification of personal information and web-based ongoing data collection. Data is collected and registered by trained personnel, following standardized procedures and regular training, supported by a rigorous audit process for quality control, which has seen a query volume decrease from over 5,000 in 2018 to around 1,000 in 2021 (Supplementary Fig. 1). An independent outcome adjudication committee reviews outcome data monthly and conducts on-site investigations if needed.
The registry’s geographical spread across 10 of the 17 first-tier administrative divisions ensures its representativeness (Fig. 1). The demographics and baseline characteristics closely match the national stroke audit data compiled by the Health Insurance Review and Assessment Service of 2018 (Supplementary Table 2), affirming the generalizability of the findings.10
We compared stroke statistics from 2021 with those from 2008–2020 to provide insights into contemporary stroke care. For recanalization therapy, owing to the significant impact of the COVID-19 pandemic on the accessibility of intravenous thrombolysis (IVT) and endovascular treatment (EVT),1112131415 the results were presented for pre-pandemic (2017–2019), and pandemic periods (2020 and 2021).161718
Stroke cases in the CRCS-K-NIH registry for 2021
In 2021, the CRCS-K-NIH registry recorded 8,992 new cases of acute stroke or TIA. Of these, 8,855 (98.5%) were diagnosed as AIS or TIA, and 137 (1.5%) as hemorrhagic strokes. This addition brings the cumulative total to 97,326 cases from 2008 to 2021 (Supplementary Table 3, Supplementary Fig. 2).
Demographics and risk factors of acute ischemic stroke
In 2021, the CRCS-K-NIH registry reported a sex ratio of 1.5 for AIS or TIA cases (Supplementary Table 4), with men constituting 59.8% and women 40.2% (Supplementary Table 5). This ratio aligns with findings from other Asian countries such as Japan, Taiwan, and China,19202122 and is higher than those observed in the United States and Sweden.2324 The lower prevalence of hypertension, diabetes, smoking, and obesity among Korean women compared to their American counterparts may contribute to these differences, indicating regional variances in vascular risk factors.2526272829
Age-specific sex ratios show that men were more prevalent in the middle-aged group (55–64 years), while women were more common in the older age group (≥ 85 years), a finding consistent with prior research.30 The mean age was 72.9 ± 13.4 years for women and 66.6 ± 12.9 years for men in 2021, both younger than counterparts in Japan and Sweden20 but similar to those in the Greater Cincinnati/Northern Kentucky Stroke Study (Supplementary Fig. 3).31 Considering these facts alongside Korea’s life expectancy, which is comparable to Japan and Sweden and longer than the US,32 highlight a higher incidence among young adults (20–54 years) compared to other countries.33
A 2-year increase in the mean age of AIS or TIA patients since 2008 reflects trends observed in Japan2034 but contrasts with stable or decreasing trends in European countries3536 and the US,31 possibly indicating a rapidly aging population in Korea and Japan.
In 2021, hypertension was the most prevalent modifiable risk factor, affecting 67.4% of AIS cases, a figure consistent with international data (Table 1, Fig. 2A).192135 The prevalence of diabetes in AIS patients was 35%, which aligns with the United States (36%) but is higher than in Sweden, the UK, and Japan, where rates range from 23–28% (Fig. 2B). This disparity is notable considering that the prevalence of diabetes among the general Korean population over 20 years old is only 10% (13% in men, 8% in women), comparable to those countries (Supplementary Table 6). This underscores the importance of exploring the gap in diabetes management and associated vascular risk factors.
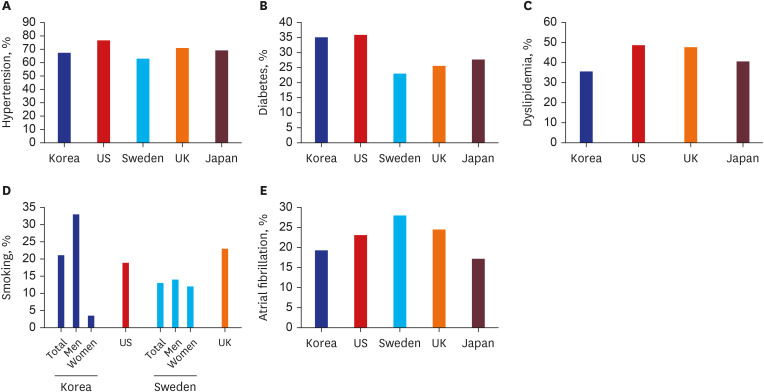
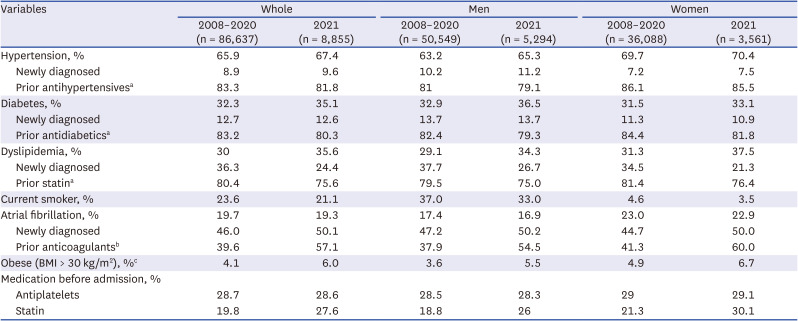
Fig. 2
Prevalences of vascular risk factors among acute ischemic stroke patients, categorized by country. Prevalence of hypertension (A), diabetes (B), dyslipidemia (C), current smoking (D) and atrial fibrillation (E).
![]()
Table 1
Major modifiable vascular risk factors and pre-stroke management
Based on 8,855 and 86,637 ischemic stroke cases registered in 2021 and 2008–2020, respectively.
BMI = body mass index.
aThe denominator of the prior medication or anticoagulants use proportion in each risk factor is the number of patients having history of the risk factor.
bAnticoagulants include warfarin, apixaban, dabigatran, edoxaban, and ribaroxaban.
cIn obese prevalence, due to missing values for height and weight, the number of patients in the population is following: 8,635 in 2021 and 84,732 in 2008–2020 of whole population; 5,166 in 2021 and 49,542 in 2008–2020 in men: 3,469 in 2021 and 35,190 in 2008–2020 in women.
![]()
Dyslipidemia was observed in 35.6% of AIS patients, slightly lower than observed in other countries (41–49%) (Fig. 2C). This parallels the lower prevalence of hypercholesterolemia in the general Korean population compared to that in the US (Supplementary Table 6).
In 2021, the prevalence of hypertension and dyslipidemia showed a slight increase compared to the levels observed during 2008–2010 (Supplementary Table 7), a trend also noted in the UK registry.35 In contrast, the prevalence of diabetes in 2021 remained largely unchanged from 2008–2010, mirroring findings from both the US37 and UK35 registries.
A notable decrease was observed in newly diagnosed cases of dyslipidemia, dropping from 36.3% in 2008–2020 to 24.4% in 2021. This shift could be attributed to improved dyslipidemia awareness and detection among the Korean general population.38 Comparatively, the proportion of patients receiving treatment prior to their index stroke for hypertension, diabetes, and dyslipidemia in Korea (Table 1) was on par with figures from the US and Japan.2037
In 2021, the proportion of stroke patients with atrial fibrillation (AF) in Korea was 19%, aligning closely with Japan (17%)22 and the UK (18%),35 but was lower compared to the US (23%),14 Germany (27%), and Sweden (28%).15 Despite the aging of the Korean stroke population, the AF prevalence has remained stable since the mid-2010s (Supplementary Table 7). This stability could be partially attributed to the widespread use of direct oral anticoagulants (DOACs) since the mid-2010s, alongside an increase in patients receiving anticoagulants prior to their index stroke observed from 2014 to 2016.3940
Nonetheless, it is noteworthy that half of the AF patients were still newly diagnosed post-stroke, a figure comparable to the global average of 43%.41 This similarity underscores the need for more proactive AF detection and primary prevention strategies in individuals at high risk of AF.
In 2021, the prevalence of current smoking among stroke patients in Korea was 21%, slightly above that in the US (19%) and significantly higher than that in Sweden (13%) (Supplementary Table 6). However, there was a clear difference in the smoking rate between Korean men and women. It was 33.3% in men, which was higher than those in US counterparts (19.2% for Black men, 11.3% for White men), while the rate of 3.5% in women was substantially lower than those observed in US women (15.4% for Black women, 13.2% for White women).42 These observations highlight the critical need for enhanced smoking cessation initiatives, particularly among Korean men, and vigilance to prevent an increase in smoking rates among Korean women.
The prevalence of obesity (body mass index > 30 kg/m2) in the Korean stroke population stood at 6.0% in 2021, lower than 15.3% reported in Germany in 2001.43 There was a 2% increase in obesity rates among both genders in 2021 compared to 2008–2020 (Table 1). Despite the lower prevalence of obesity in South Korea relative to western countries,44 the rising trend, likely attributed to changes in dietary patterns, calls for increased awareness and intervention.
Clinical characteristics of acute ischemic strokes
In 2021, large artery atherosclerosis (LAA) emerged as the predominant subtype of AIS within the CRCS-K-NIH cohort, surpassing cardioembolism (CE) and small vessel occlusion (SVO) (Table 2, Supplementary Fig. 4, Supplementary Table 8). The LAA subtype accounted for 38% of cases, significantly exceeding the proportions observed in Japan (21%),45 the UK (9%),35 Canada (25%),46 and the Czech Republic (28%).47 This higher proportion may be attributed to several factors:
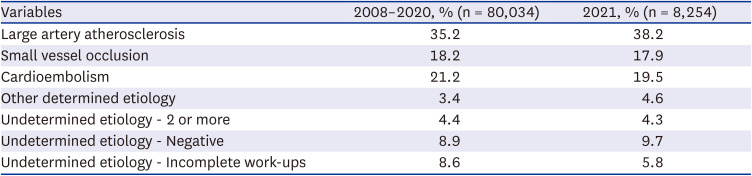
Table 2
Proportion of patients according to the TOAST classification in 2008–2020 vs. 2021
Based on 88,288 AIS cases registered between 2008 and 2021.
TOAST = Trial of ORG 10172 in Acute Stroke Treatment, AIS = acute ischemic stroke.
![]()
First, the greater prevalence of intracranial arterial disease among East Asians compared to Non-Hispanic Caucasians.48
Second, the adoption of less stringent criteria for defining the LAA subtype in Korea, including the use of an magnetic resonance imaging (MRI)-based algorithm for stroke subtype classification without a 50% stenosis threshold.49
Third, the increased utilization of advanced imaging techniques, such as high-resolution vessel wall MRI, facilitating more sensitive detection of arterial anomalies.48
In 2021, among patients with LAA stroke, 58% exhibited symptomatic intracranial arterial stenosis of over 50% or occlusion (Fig. 3, Supplementary Table 9). The prevalence of symptomatic intracranial steno-occlusion among AIS patients was 22%, which is consistent with findings from a sub-study of the Oxford Vascular Study.50
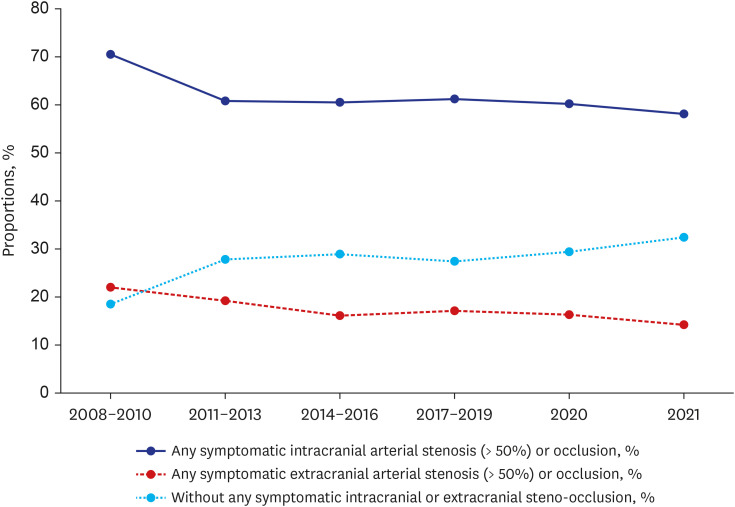
From 2008–2010 to 2021, there was a notable decline in the prevalence of symptomatic steno-occlusion of major cerebral arteries among patients with LAA stroke: from 70.5% to 58.1% for intracranial steno-occlusion and from 22.0% to 14.2% for extracranial steno-occlusion. This trend may be partially attributed to the increased use of lipid-lowering drugs in the general Korean population,38 supported by the rising proportion of patients receiving statins prior to index stroke, as indicated in our data (Table 1).
Between 2008 and 2021, 18.0% of AIS patients in the CRCS-K-NIH registry were identified to have a high-risk cardio-embolic source, predominantly due to AF (Supplementary Table 10). Additionally, medium-risk cardioembolic sources were present in 6.0% of patients, such as patent foramen ovale and lone AF.
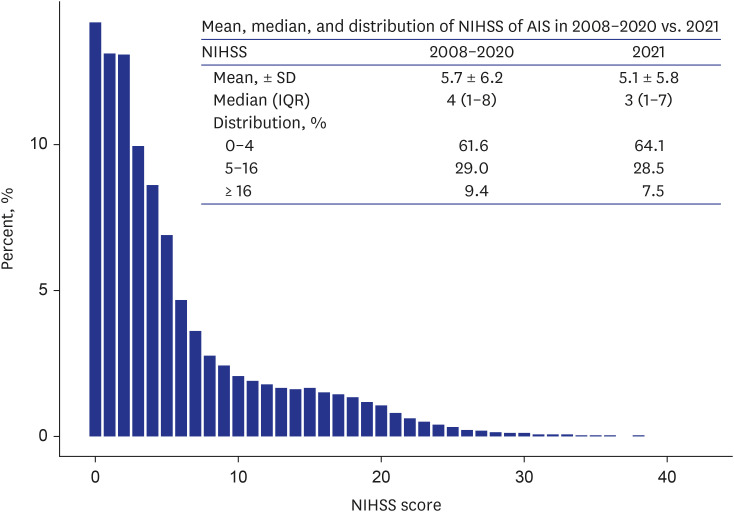
In 2021, the median National Institute for Health Stroke Scale (NIHSS) score among patients registered in the CRCS-K-NIH was 3, with an interquartile range (IQR) of 1–7 (Fig. 4), aligning with data from other countries.2437 Approximately 64% of patients experienced minor strokes (NIHSS scores of 0–4), a figure comparable to rates observed in the US24 and the UK.35 The proportion of minor strokes has increased over time, consistent with trends reported internationally.192035
The majority (81.2%) of patients had a pre-stroke modified Rankin Scale (mRS) score of 0 (Supplementary Tables 11). The prevalence of patients with a history of stroke or TIA was 23% (Supplementary Table 12), closely mirroring Japan’s 24%20 but lower than the 31% documented in the US.23 Among those with a history of stroke, 50% had a pre-stroke disability (pre-stroke mRS ≥ 1), compared to 15% among those without a stroke history (Supplementary Table 13).
Recanalization therapy
Accessibility of recanalization therapies was notably hindered during the COVID-19 pandemic.1112131415 Accordingly, pre-pandemic data (2017–2019) and pandemic data (2020 and 2021) were analyzed separately to underscore these effects.
In the pre-pandemic period (2017–2019), the IVT rate of 11.9% was comparable to the US data (11%) in 2019,23 yet lower than those in Germany (16%)51 and Sweden (14%)24 in the same year, but it was slightly higher than the rate in Japan (9%)22 (Fig. 5, Supplementary Table 14). In contrast, the EVT rate in 2017–2019 was 9.8%, surpassing the rates in the US,23 Germany,51 and Sweden,24 all at 7%.
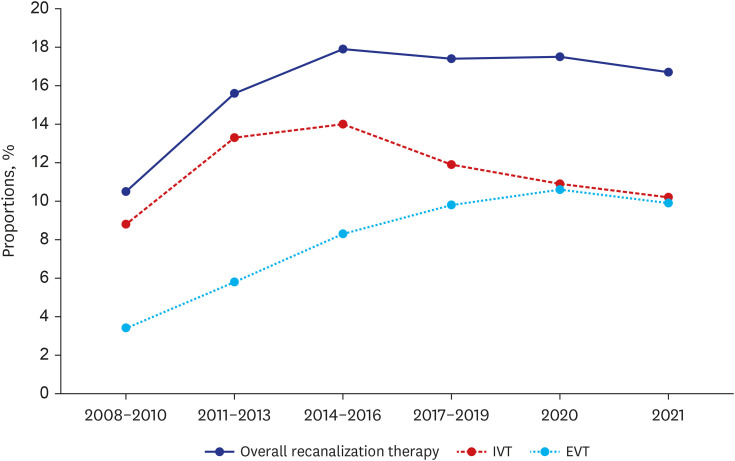
The overall rate of recanalization therapy has plateaued since 2015, characterized by a declining IVT rate alongside an ascending EVT rate (Fig. 5, Supplementary Table 14). This pattern contrasts with other countries, where an increase in treatment rates has been observed.525354 The declining of IVT rate in Korea might be attributed to an inadequate number of primary stroke centers and a lack of human resources, even in hospitals where have stroke centers.
During the COVID-19 pandemic, a decline in the overall IVT rate was noted, falling to 10.9% in 2020 and further to 10.2% in 2021 (Fig. 5, Supplementary Table 14), aligning with trends observed in Japan,2255 Germany,12 and China.14 The proportion of patients receiving IVT within 4.5 hours of symptom onset also decreased, from 41% during 2014–2016 to 34% in 2021. Similarly, the EVT rate experienced a slight decline from 10.6% in 2020 to 9.9% in 2021, reflecting a global decrease in EVT procedures during the pandemic.11
There was no significant improvement in door-to-needle (DTN) or door-to-puncture (DTP) times since 2013 (Fig. 6, Supplementary Table 15). In 2021, the proportion of patients with a DTN time under 60 minutes was 77%, comparable to US data from 2019 and 2020,13 yet falling short of the American Heart Association (AHA)’s target of 85%.56 The median DTN time remained around 37.0 minutes since 2014, in contrast to the ongoing improvements seen in the US, Canada, and Italy.525354
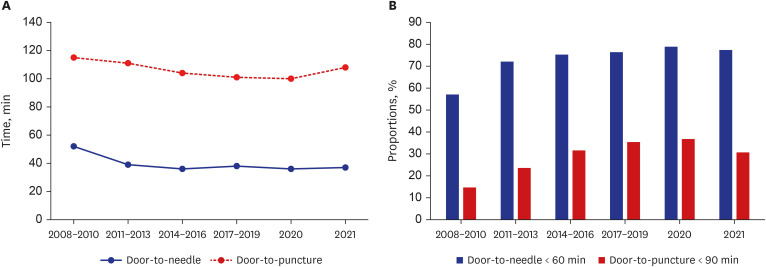
In 2021, the median DTP time recorded was 108 minutes, with only 31% of cases achieving a DTP time under 90 minutes (Fig. 6, Supplementary Table 15), falling short of the AHA’s target of 50%.56 This median DTP time not only exceeds the AHA goal but is also longer compared to the US (97 minutes)13 and Germany (74 minutes) data.57 Our recent data indicate an increasing trend in median DTP time, underscoring a lack of progress in reducing treatment delays. The lack of improvement in the IVT rate and DTP time could be attributable to several key factors within the Korean healthcare system. One major issue is the shortage of stroke specialists, which hampers the ability to provide continuous care. Additionally, many hospitals, particularly outside of major urban centers, lack the necessary infrastructure to support a full-time (7-day, 24-hour) stroke response team. This limitation is critical for timely recanalization therapy, which is essential for optimal stroke outcomes. Further compounding these challenges are the financial and logistical constraints that prevent the expansion of dedicated stroke care facilities and the adoption of advanced stroke care protocols uniformly across the country.
Recanalization therapy-related quality indicators exhibited significant disparities across participating centers, as illustrated in Supplementary Fig. 5 and Supplementary Table 16. Only 18% and 12% of hospitals met the AHA goal of a DTN time of less than 60 minutes in 85% of cases, and a DTP time of less than 90 minutes in 50% of cases, respectively.56 These disparities across centers underscore the critical need for concerted efforts to enhance treatment timeliness.
The median time from the last known-well time or the first abnormal time to hospital arrival decreased steadily until 2019. However, there was an increase in these timeframes thereafter (Supplementary Table 17), likely due to the impact of the COVID-19 pandemic.
Acute management
In 2021, 66.7% of AIS patients received stroke unit (SU) care, a significant rise from the period of 2014-2016 (Supplementary Table 18). Although this rate surpasses Canada’s 54%,52 it falls short of Sweden’s 93%.24 Since 2017, the increase in SU care has plateaued, mirroring trends observed internationally and indicating a potential need for enhanced efforts to boost SU admissions.2452 This stagnation might be explained by the decreasing financial attractiveness of providing SU care in general hospitals, due to overall inflation and fixed reimbursement rates for such care. With the national stroke audit designating SU care as a key quality indicator in 2020, further enhancements in accessibility to SU care are anticipated.
Our data exhibit a high utilization rate of MRI-based imaging for AIS patients. During hospitalization, diffusion-weighted imaging (DWI), MRI, and MR angiography were performed in 95%, 87%, and 88% of AIS cases, respectively, significantly surpassing the MRI scan rates in the US (33%) and Sweden (35%) (Supplementary Table 19).2458 Additionally, perfusion MRI and computed tomography imaging were conducted in 31% and 6% of AIS patients, showcasing the comprehensive imaging approach adopted in Korea.
In 2021, AIS patients showed a decrease in average total cholesterol and low-density lipoprotein (LDL) levels at admission (Supplementary Table 20), aligning with a gradual rise in the use of lipid-lowering drugs among Korean individuals at risk of cardiovascular disease.38 Initial glucose levels and hemoglobin A1c remained unchanged. However, average systolic and diastolic blood pressures at presentation have slightly increased, mirroring the rise in hypertension prevalence in Korea.59
In 2021, the use of transthoracic echocardiography (TTE) in our data reached 73%, surpassing Germany’s 66%.60 However, the use of transesophageal echocardiography (TEE) was notably lower at 4%, compared to Germany’s 21% (Supplementary Table 21). The adoption of 24-hour Holter monitoring was 57%, exceeding Canada’s 31%.61 TEE and Holter monitoring were frequently used in evaluating patients with embolic stroke of undetermined source, being utilized in 85% and 71% of cases, respectively.
Antithrombotic drugs were administered to 94% of AIS patients within 48 hours of hospitalization in 2021 (Supplementary Table 22), aligning closely with the US rate of 97%.23 Aspirin monotherapy was the most common treatment until 2016, but the combination of aspirin plus clopidogrel became the preferred regimen after 2017, used in 65% of cases by 2021 (Fig. 7A).
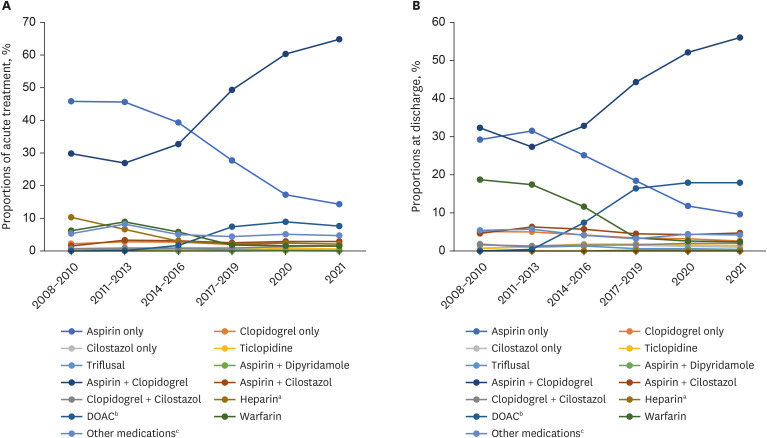
Fig. 7
Antithrombotic medications (multiple choices permitted) administered between 2008 and 2021. (A) Acute (within 48 hours of hospitalization) and (B) at-discharge antithrombotic medications.
aBoth conventional and low-molecular weighted heparin.
bApixaban, dabigatran, rivaroxaban, edoxaban.
cOther antiplatelets + other anticoagulants.
![]()
Upon discharge in 2021, aspirin plus clopidogrel was prescribed to 56% of all AIS patients (Supplementary Table 23), 64% of minor (NIHSS ≤ 3 points) stroke cares, and 47% of non-minor stroke cases (Fig. 7B, Supplementary Table 24). These rates are higher than those in the US; 47.0% and 42.6% for minor and non-minor stroke, respectively.62
In 2021, DOACs were prescribed at discharge for 75% of patients with CE stroke associated with AF (Table 3), a rate comparable to Sweden’s 78%.24 Additionally, DOACs were used acutely (within 48 hours of hospitalization) in 33% of these cases. It should be noted that previous evidence regarding the use of DOAC has been focused on stroke prevention in patients with AF or cryptogenic stroke. However, the role of DOACs is expanding, with emerging evidence supporting the benefits of their early initiation in patients with CE stroke and AF.63 Notably, the use of DOACs for CE stroke without AF increased to 26% in 2021, while warfarin usage significantly dropped from 39% in 2008–2010 to 12% in 2021, indicating a significant shift in anticoagulation practices that merits further investigation.

Table 3
Use of DOACs in cardioembolic stroke patients with and without atrial fibrillation
DOAC = direct oral anticoagulant.
aBased on 14,621 cardioembolic stroke patients with atrial fibrillation.
bBased on 3,971 cardioembolic stroke patients without atrial fibrillation.
![]()
In 2021, 91% of AIS patients were prescribed statins at discharge, a rate on par with the US (81%)23 and Sweden (84%),24 but significantly higher than Japan (47.1%).22 This represents an increase from 72% in 2008–2010, mirroring the upward trend seen in Sweden,24 where statin prescriptions rose from 64% in 2011 to 84% in 2022. Conversely, the US observed a stagnation in statin prescription rates, moving from 84.8% in 2007 to 81.2% in 2021.2364
The increase in statin prescriptions in South Korea spanned all stroke subtypes, including LAA, CE, and SVO (Supplementary Fig. 6, Supplementary Table 25). Landmark studies demonstrating the benefits of early statin use, including “Effects of Very Early Use of Rosuvastatin in Preventing Recurrence of Ischemic Stroke (EUREKA)”65 and “Target Stroke to Target (TST)”66 could lead to a lack of hesitation among clinicians in prescribing statins during the acute phase. Furthermore, comparative effectiveness research from CRCS-K-NIH revealed that CE patients who were treated with statins had better long-term outcomes, further supporting the widespread use of statins in CE as well.67 Increasing statin prescription rate across subtypes of AIS might be explained, partly by positive results from above-mentioned studies that included Korean stroke patients.
In the 2021 CRCS-K-NIH data, decompressive surgery for AIS patients was performed at rates of 0.6% (Supplementary Table 26), notably lower than the 1.2% reported by comprehensive stroke centers in the US (2013–2018)68 and 1.9% in Germany (2017).69 This discrepancy may stem from differences in patient and family perceptions, cultural attitudes, and medical resource availability, highlighting areas for deeper exploration. In 2021, other surgical interventions like bypass surgery, endarterectomy, and angioplasty/stenting were carried out in 0.2%, 0.1%, and 1.6% of AIS patients, respectively.
Clinical outcomes after ischemic stroke
Since 2011, clinical outcomes for AIS patients have been systematically collected. The 2021 outcomes were analyzed in comparison to previous periods (2011–2019 and 2020). Specifically, a contemporary 1-year outcome was defined in 2020 for comparative analysis. In 2021, 13.4% of AIS patients (out of 8,254 cases) experienced early neurological deterioration (END) (Table 4), a rate that aligns closely with pooled meta-analysis data (13.8%)70 and reports from China (14.1%).71 The primary cause of END was stroke progression. Symptomatic hemorrhagic transformation (SHT) was observed in 0.8% of patients, with those undergoing IVT showing a SHT rate of 2.8%—comparatively on the lower spectrum against other studies (2.1–8.8%) and IVT trial findings (1.9–8.8%).7273 Among patients receiving EVT, the SHT rate was 4.5%, slightly below the rates reported in EVT trials (4.9–9.0%),74757677 and a cohort study from the Netherlands (6%).78 Furthermore, the proportion of patients achieving a favorable outcome (a mRS score of 0–2) at discharge stood at 61%, echoing results from the Japanese Stroke Data Bank (51%).20
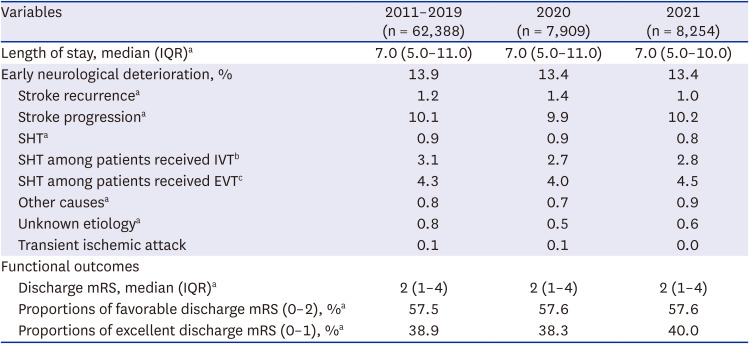
Table 4
Events and outcomes during the hospitalization between 2008 and 2021
IQR = interquartile range, SHT = symptomatic hemorrhagic transformation, IVT = intravenous thrombolysis, EVT = endovascular treatment, mRS = modified Rankin Scale.
aBased on 88,288 ischemic stroke cases registered between 2011 and 2021.
bBased on 9,665 ischemic stroke cases received IVT between 2011 and 2021.
cBased on 6,664 ischemic stroke cases received EVT between 2011 and 2021.
![]()
In 2021, the CRCS-K-NIH registry reported a 3-month cumulative incidence of recurrent stroke at 3.2%, aligning closely with Germany’s rate of 3.1% between 1998 and 2015 (Table 5).79 Our 1-year cumulative incidence was 5.1%, comparable to Denmark’s 4%80 but lower than Germany’s 7.5% (1998–2015)79 and the US Medicare Fee-for-Service population’s 7.6% (2016–2017).81 These variations could be attributed to enhanced prevention strategies and differences in outcome collection methods. The 1-year mortality rate in Korea was 9.6% in 2020, significantly lower than Germany (21.0%),79 Denmark (17%),80 and Sweden (26% in 2013),82 which might be explained by high accessibility to hospitalization for acute stroke even for patients with mild stroke and potential advances in stroke managements in Korea.
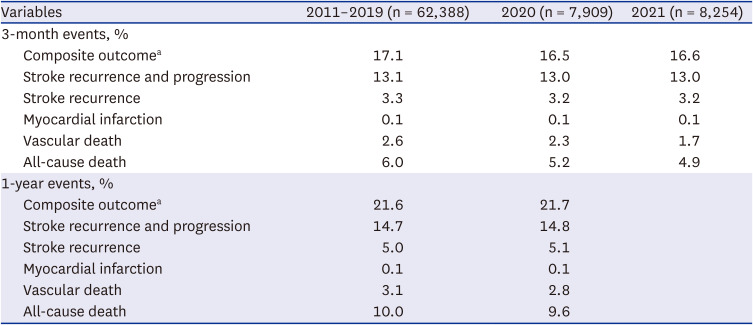
Table 5
Cumulative incidences (%) of outcome events after stroke
Based on 88,288 ischemic stroke cases registered between 2008 and 2021.
aComposite outcome: All-cause stroke + myocardial infarction + all-cause death.
![]()
The subgroup analysis revealed that the 1-year cumulative incidence of recurrent stroke hospitalized in 2020 was highest among AIS patients with undetermined etiologies-two or more) at 10.1%, followed by LAA at 5.7%, CE at 5.1%, undetermined-negative at 4.7%, undetermined-incomplete at 4.1%, and SVO at 2.8% (Supplementary Table 27). This pattern is somewhat mirrored in the German data, where stroke recurrence was notably common among patients with undetermined etiologies, succeeded by CE, LAA, and SVO.79 The pronounced recurrence in patients with undetermined etiologies-two or more underscores the need for further research. The comparatively lower recurrence rates in Korean patients with LAA and CE might reflect the recent adoption of dual antiplatelet therapy for non-CE strokes and DOACs for CE strokes, as opposed to the higher recurrence rates observed in Germany (7.7% in LAA and 8.0% in CE).79
In our cohort, 3-month and 1-year mRS scores were collected for 97% and 93% of patients, respectively. In 2021, 63% of all AIS patients achieved favorable outcomes (mRS 0–2) at 3 months, with 55% of those receiving IVT and 41% undergoing EVT achieving similar outcomes (Tables 6 and 7, Supplementary Fig. 7). These rates align with those from other cohort studies838485 and clinical trials.6986 Excellent 3-month outcomes (mRS 0–1) were seen in 48% of all AIS patients and 39% of those receiving IVT, surpassing the 31% reported in a meta-analysis of IVT trials.72 For 2021, favorable one-year outcomes were observed in 64% of AIS patients, with excellent one-year outcomes reported at 49% for 2020 (Supplementary Fig. 8).
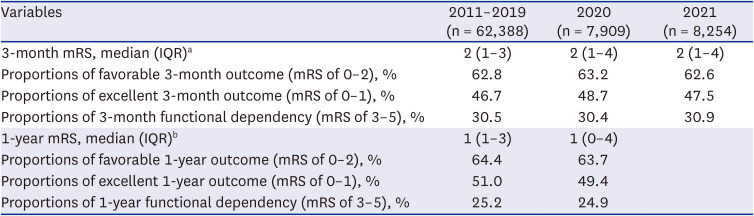
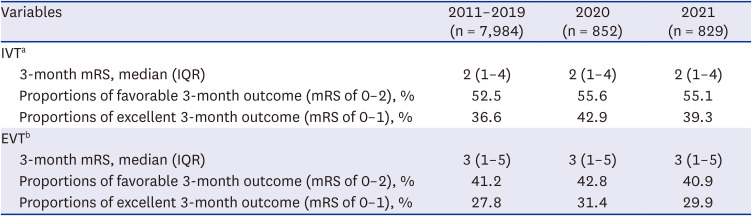
Table 6
Functional outcomes at 3 months and 1 year after stroke
IQR = interquartile range, mRS = modified Rankin Scale.
aBased on 76,222 ischemic stroke patients reported 3-month outcome between 2011 and 2021.
bBased on 65,048 ischemic stroke patients reported 1-year outcome between 2011 and 2020.
![]()
Table 7
Functional outcomes at 3 months and 1 year after stroke in patients received IVT and EVT
IVT = intravenous thrombolysis, EVT = endovascular treatment, IQR = interquartile range, mRS = modified Rankin Scale.
aBased on 9,419 ischemic stroke patients received IVT and reported 3-month outcome between 2011 and 2021.
bBased on 6,484 ischemic stroke patients received EVT and reported 3-month outcome between 2011 and 2020.
![]()
In 2021, functional dependency at 3 months post-stroke, defined by a mRS score of 3–5, remained at 31%, unchanged from the period 2011–2019. This stability contrasts with improvements seen in England, where functional dependency decreased from 35% (2000–2003) to 27% (2012–2015) as defined by a Barthel index < 15, and in Sweden,35 where it improved from 19% in 2011 to 15% in 2022, as measured by Activities of Daily Living scales.2487
SUMMARY
• The sex ratio of 1.5 favoring men over women in Korea aligns with other Asian countries and is notably higher than that in the US and Sweden. The difference between Korea and the US could be attributed to the lower prevalence of hypertension, diabetes, smoking, and obesity among Korean women.
• The average age for patients with AIS and TIA in this cohort was 73 years for women and 67 years for men. These ages are lower than those reported in Japan but are comparable to the United States. Considering these facts alongside Korea’s life expectancy being similar to Japan’s and higher than that of the US highlights the earlier onset of stroke in Korea. Since 2008, there has been a rising trend in the average age of the stroke population, a trend that mirrors data from Japan.
• Hypertension, present in 67%, was the most common risk factor. comparable to the prevalence in other countries. The diabetes prevalence in our cohort (35%) was higher than that in Sweden, the UK, and Japan, despite the prevalence in general population being lower than these countries. Dyslipidemia prevalence (35.6%) was marginally lower than in other countries and newly diagnosed dyslipidemia decreased from 2008–2020 to 2021.
• The prevalence of AF in AIS patients was 19%, lower than that in western countries, which could reflect the effective stroke prevention strategies for AF. Nonetheless, a significant number of AF cases are diagnosed only after a stroke has occurred.
• The smoking rate among AIS patients in Korea stands at 21%, significantly higher than in the US and Sweden, especially among Korean men, underscoring the urgent need for more aggressive smoking cessation initiatives.
• The proportion of LAA at 38% exceeds those observed in the UK, Japan, and Canada. This discrepancy may be due to higher prevalence of intracranial arterial disease among East Asians, less stringent definition of LAA, and the widespread use of advanced imaging techniques. The prevalence of symptomatic intracranial or extracranial steno-occlusions (> 50%) has declined from 2008–2010 to 2021, a trend that cloud be partly attributed to the increased use of lipid-lowering drugs.
• About two-thirds of patients were presented with minor stroke (NIHSS score of 0–4) that the proportion has increased from 2008–2010 to 2021, similar to other countries. The median NIHSS score was 3 in 2021, also similar to other countries.
• In the pre-pandemic (2017–2019), the IVT rate was 11.9% which was lower than that in Germany and Sweden, and it decreased from 14.0% during 2014–2016. The EVT rate (9.8%) was higher than other countries and saw a significant rise from 3.4% in 2008–2010. During the pandemic, a decreasing trend in IVT and EVT was noted, reflecting pandemic influences similar to global trends.
• Since 2014, the median DTN time has stayed constant at approximately 37 minutes, unlike the continuous improvements observed in other countries. In 2021, the median DTP time was recorded at 108 minutes, showing an upward trend and highlighting a stagnation in efforts to minimize treatment delays.
• Until 2016, aspirin monotherapy was the predominant acute treatment, but since 2017, aspirin plus clopidogrel has become the preferred regimen, being utilized in 65% of cases by 2021. Upon discharge, this dual therapy became the most common, prescribed to 64% of minor stroke patients and 47% of those with more severe strokes in 2021.
• Among CE stroke patients with AF, 75% were prescribed DOACs, with 33% receiving within 48 hours. Notably, warfarin usage significantly declined from 39% in 2008–2010 to 12% in 2021 and DOACs were used in 26% in 2021 among CE stroke patients without AF. Additionally, statins were prescribed at discharge to 91% of patients, indicating an upward trend in their use across all AIS subtypes.
• END occurred in 13%, a rate comparable to that found in meta-analysis data. SHT rates among patients who received IVT and EVT were 2.8% and 4.5%, respectively, both of which are relatively lower than the rates reported in other studies.
• In 2021, the crude 3-month cumulative incidence of recurrent stroke was 3.2%, aligning with historical figures from Germany. However, the 1-year recurrence rate of 5.1% was somewhat lower than those reported in Germany and the US until the mid-2010s, potentially reflecting advancements in stroke prevention strategies. The pronounced one-year recurrence in patients with undetermined etiologies-two or more (10.1%) draws our attention.
• The proportion of 3-month mRS 0–2 was 63%, comparable to other cohort studies and IVT trials. The proportion of patients with 3-month dependency (mRS 3–5) has remained at 31% in 2021, while a decrease was observed in other countries. Lower IVT rate and delays in DTP time for EVT could be attributable to this finding, at least partly.
CONCLUSION
These findings from the CRCS-K-NIH registry underscore unique epidemiological and clinical features of stroke in Korea, including a relatively younger stroke onset considering Korea’s life expectancy, higher diabetes and smoking prevalence, but lower AF prevalence. Notably, the lower rate of IVT and prolonged DTP times for EVT are pressing concerns requiring immediate intervention. Although dual antiplatelet therapy for non-CE stroke and DOACs for AF-related stroke have been effectively adopted, the declining use of warfarin and increasing use of DOACs for non-AF CE stroke warrants draw our attention. Prompt action to address these challenges is crucial.
 XML Download
XML Download