

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hepatocellular carcinoma (HCC) is the second-leading cause of cancer-related mortality in Korea.1 Additionally, mortality related to primary liver cancer is continuously increasing in the United States, although the data include intrahepatic biliary tract cancer.2
HCC occurs in patients with chronic hepatitis and/or liver cirrhosis.34 The active application of curative aimed treatment for patients with HCC is on the rise, particularly in populations at high risk of HCC development. This increase can be attributed to the active implementation of screening programs that prioritize early detection.56 However, frequent intrahepatic recurrence (IHR) remains an unresolved problem, even after curative treatment, including surgical resection and local ablation therapies (LAT), in early HCC.78
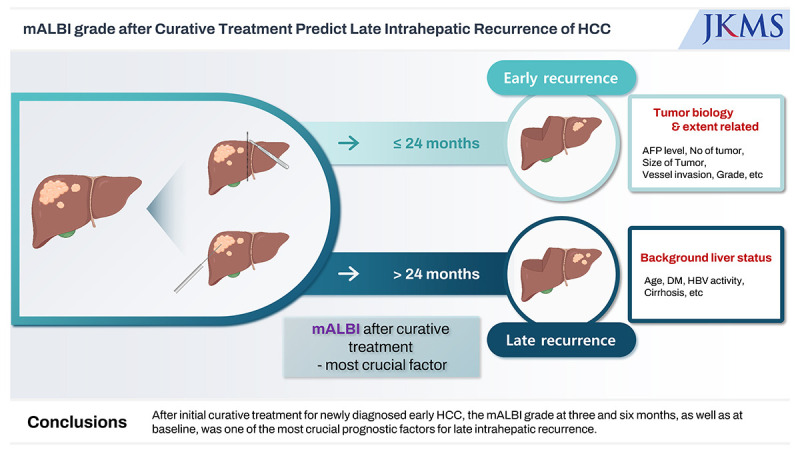
IHR develops in approximately 70% of the patient within five years after curative treatment of early stage HCC. It is divided into early IHR associated with previously treated tumors, and late IHR, in which de novo development of tumors is based on underlying chronic liver disease.9 Among these, the prognostic factors for early IHR are known relatively clearly, but the factors for late IHR are mainly associated with recurrence after two years of curative treatment. Identifying these prognostic factors for late IHR can provide important clues for strategies of surveillance and/or early detection for the application of curative salvage treatment depending on the risk grouping. In addition, it is possible to provide information that can reduce the risk of late IHR through appropriate additional interventions according to the causes of the prognostic factors.
Based on this background, we conducted the present study to identify prognostic factors for late IHR, and recurrence was defined as two years after curative treatment for HCC, based on prospectively collected data from a relatively large cohort at a single tertiary institution.
METHODS
Patients
Since January 2005, the Samsung Medical Center (SMC) has prospectively collected data on newly diagnosed, previously untreated patients with HCC and has managed them on an HCC registry.
The present study was conducted on patients who were registered in the SMC HCC registry by December 2017 and who met the following criteria; 1) diagnosed with HCC histologically or clinically according to the guidelines of the Korean Liver Cancer Association-National Cancer Center Korea (KLAC-NCC), 2) Barcelona Clinic Liver Cancer (BCLC) stage 0 or A at diagnosis, 3) received curative aim treatment as initial treatment including hepatic resection, LAT such as radiofrequency ablation (RFA), intraoperative RFA, RFA with hepatic resection, percutaneous ethanol injection, microwave ablation, cryoablation, stereotactic body radiotherapy, proton beam therapy and transarterial chemoembolization (TACE) plus RFA; and except liver transplantation, 4) did not show early IHR defined as recurrence within two years, 5) followed-up for more than two years at SMC, 6) did not show extrahepatic spread at the first recurrence, and 7) underwent laboratory tests included in this study at baseline, three months (± 4 weeks), and six months (± 4 weeks) after the initial treatment.
Data collection
The details of the SMC HCC registry data used in the present study have been previously reported.101112 Briefly, baseline characteristics, including age at diagnosis, sex, date of diagnosis, etiology, diabetes, hypertension, Eastern Cooperative Oncology Group performance status, Child-Pugh score and class, number of tumors, maximum tumor size, the BCLC stage, modified Union for International Cancer Control (mUICC) stage, α-fetoprotein (AFP), the protein induced by vitamin K absence or antagonist-II (PIVKA-II), the Model for End-Stage Liver Disease (MELD) score, and modified albumin-bilirubin (mALBI) score and grade were collected at the time of registration within four weeks of HCC diagnosis at SMC, and initial treatment modality, and treatment and/or pathologic reports were added after the treatment. Although not included in the prospective collected variables in the HCC registry, complete blood cell count and differential counts at the time of diagnosis and laboratory tests including complete blood cell count and differential counts, aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, albumin, bilirubin, AFP and PIVKA-II at three months (± 4 weeks), six months (± 4 weeks), and 24-months (± 8 weeks) after the initial treatment were obtained through medical records. Based on the collected data, the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), systemic immune inflammation index (SII), aspartate aminotransferase (AST)-to-platelet ratio (APRI), and AST-to-lymphocyte ratio (ALRI) were calculated at each time point. Lastly, we determined the presence of liver cirrhosis by assessing the morphological changes observed on imaging modalities at the time of registration or on histopathology if patients underwent surgical resection. In addition, recurrence and survival status during follow-up were evaluated in May 2022.
Follow-up
Patients were followed up one month after the initial curative treatment and every two–three months thereafter. Physical examinations, chest radiography, and laboratory tests, including complete blood cell count, differential counts, serum AFP, PIVKA-II, and liver function, were performed at each follow-up. Dynamic liver computed tomography (CT), including the pelvic area and/or liver magnetic resonance imaging (MRI), was also performed during the routine follow-up period, or more often if recurrence was suspected.
The primary endpoints of the present study were late IHR and late IHR-free survival (IHRFS), defined as the time interval from initial curative treatment to the first IHR two years after the application of initial curative treatment, death without IHR, or last follow-up, whichever came first. The secondary purpose was to evaluate whether prognostic factors that were significant in late IHR and late IHRFS also affected overall survival (OS), defined as the time interval from the initial curative treatment to death or the last follow-up.
Statistical analysis
To compare the characteristics between the groups showing late IHR or not, the χ2 test or Fisher’s exact test was used for categorical variables, and the t-test or Wilcoxon rank-sum test was used for continuous variables. Candidate prognostic factors included the variables assessed by laboratory tests at each of the different time points (baseline, three months, and six months), and also included the increments in those variables from baseline to three months and six months. Cox proportional hazards regression models were used to identify the prognostic factors affecting late IHR in univariable and multivariable analyses. And, multivariable model was built using variables with a P value ≤ 0.1 in the univariable analysis. The proportional hazard assumption was verified using Schoenfeld residuals. Collinearity was examined using variance inflation factor in the multivariable analysis. To explore changes in the rates of late IHR at baseline, three months, and six months, nested pie charts were constructed using the JMP (version 17.0; SAS Institute, Cary, NC, USA) program in all patients, surgery, and LAT groups. The curves of late IHRFS and OS were estimated using the Kaplan-Meier method and compared using the log-rank test with Tukey’s test for post-hoc comparison. A two-sided P value < 0.05 was considered to be statistically significant, and statistical analyses were performed using the SAS version 9.4 (SAS Institute) and R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org/).
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board (IRB) of the Samsung Medical Center (IRB No. 2022-04-100). The requirement for informed consent was waived owing to the retrospective nature of this study. The study was performed in accordance with the Declaration of Helsinki.
RESULTS
Patients and late IHR
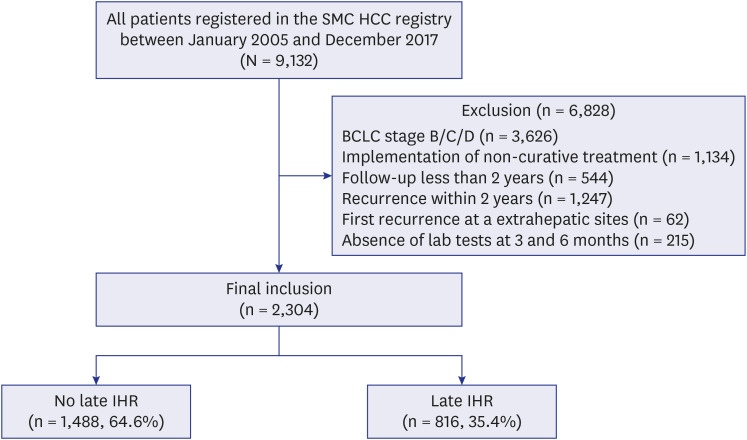
Among the 9,132 patients registered in the SMC HCC registry between January 2005 and December 2017, 5,506 had stage 0 or A BCLC disease at the time of registration. Among them, 6,828 patients who did not meet the inclusion criteria, including 1,247 patients with early IHR, were excluded, and a total of 2,304 patients included in the present study, finally (Fig. 1). Curative intent hepatectomy was conducted in 1,427 (61.9%) patients and the remaining 877 (38.1%) patients underwent LAT. RFA was performed in a total of 761 (86.8%) patients, the majority of the LAT patient group. The number of patients using specific treatment methods other than RFA in the LAT group is shown in Supplementary Table 1.
During the follow-up period (median, 82.6 months; range, 24.1 to 195.7), late IHR was developed in 816 (35.4%) patients. The late IHRFS and OS of all enrolled patients were 72.1% and 95.8% at 5-years, and 55.2% and 83.6% at 10-years, respectively (Supplementary Fig. 1).
Baseline prognostic factors related with late IHR and late IHRFS
Table 1 shows the comparison of the baseline characteristics of the patients according to the presence of late IHR. Older age, male sex, diabetes at HCC diagnosis, and hepatitis C virus infection were common in the late IHR group, although the differences were not clearly marked. In addition, the factors showing the greatest differences were the liver cirrhosis, Child-Pugh class and mALBI grade, which represent the baseline normal liver status and the initial treatment method.
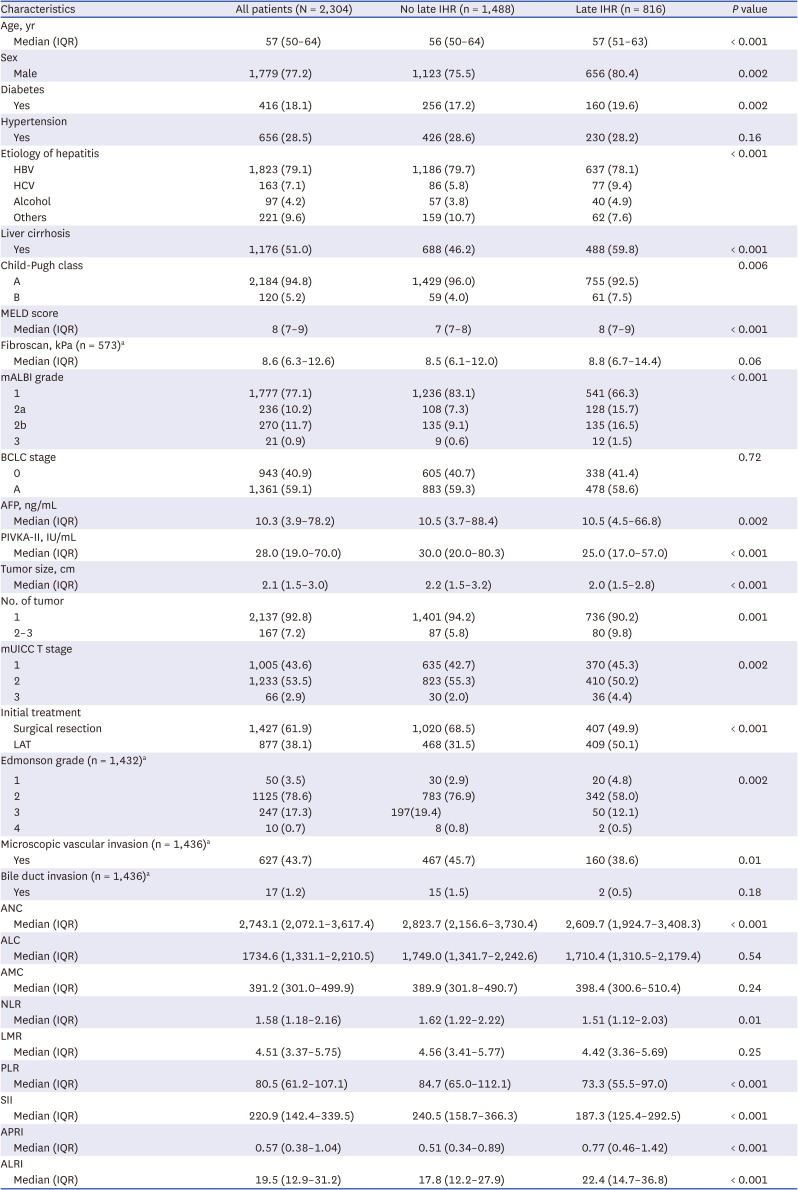
Table 1
Baseline characteristics
Data shown are number (%) not otherwise specified.
IHR = intrahepatic recurrence, IQR = interquartile range, HBV = hepatitis B virus, HCV = hepatitis C virus, MELD = Model for End-Stage Liver Disease, mALBI = modified albumin-bilirubin, BCLC = Barcelona Clinic Liver Cancer, AFP = α-fetoprotein, PIVKA-II = protein induced by vitamin K antagonist-II, mUICC = modified Union for International Cancer Control, LAT = local ablative treatment, ANC = absolute neutrophil count, ALC = absolute lymphocyte count, AMC = absolute monocyte count, NLR = neutrophil-to-lymphocyte ratio, LMR = lymphocyte-to-monocyte ratio, PLR = platelet-to-lymphocyte ratio, SII = systemic immune-inflammation index, APRI = aspartate aminotransferase-to-platelet ratio, ALRI = aspartate aminotransferase-to-lymphocyte ratio.
aThe analysis was performed only in patients who underwent baseline test or pathologically confirmed through surgical resection with or without LAT.
![]()
Age and laboratory test values (absolute neutrophil count and systemic immune and inflammatory markers [NLR, PLR, LMR, SII, APRI, and ALRI]) were significant prognostic factors for late IHRFS as continuous variables, while AFP and PIVKA-II were not significant prognostic factors in the univariable analysis. In the multivariable analysis, age (P < 0.001; hazard ratio [HR], 1.02; 95% confidence interval [CI], 1.01–1.03), and PLR (P = 0.03; HR, 1.00; 95% CI, 0.99–1.00) were the continuous variables, and male sex (P = 0.001; HR, 1.37; 95% CI, 1.14–1.64), liver cirrhosis (P < 0.001; HR, 1.30; 95% CI, 1.11–1.52), initial treatment method (P < 0.001; HR, 1.52; 95% CI, 1.30–1.77), and mALBI grade (2a vs. 1, P < 0.001; HR, 1.50; 95% CI, 1.19–1.89; 2b/3 vs. 1, P = 0.01; HR, 1.35; 95% CI, 1.05–1.74) were the categorical variables showing statistically significant differences in terms of late IHRFS as a baseline factors (Table 2).
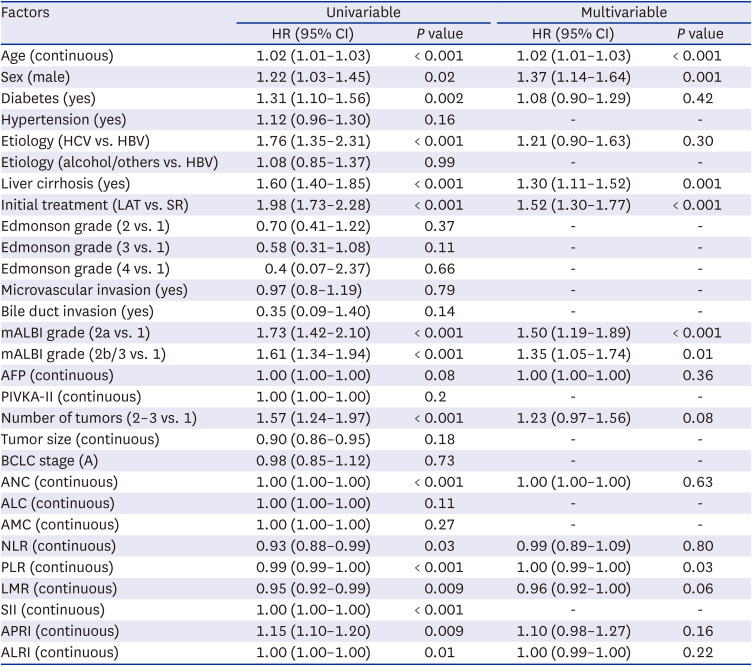
Table 2
Univariable and multivariable analysis of late intrahepatic recurrence-free survival and baseline characteristics
HR = hazard ratio, CI = confidence interval, HCV = hepatitis C virus, HBV = hepatitis B virus, LAT = local ablation therapy, SR = surgical resection, mALBI = modified albumin-bilirubin, AFP = α-fetoprotein, PIVKA-II = protein induced by vitamin K antagonist-II, BCLC = Barcelona Clinic Liver Cancer, ANC = absolute neutrophil count, ALC = absolute lymphocyte count, AMC = absolute monocyte count, NLR = neutrophil-to-lymphocyte ratio, PLR = platelet-to-lymphocyte ratio, LMR = lymphocyte-to-monocyte ratio, SII = systemic immune-inflammation index, APRI = aspartate aminotransferase-to-platelet ratio, ALRI = aspartate aminotransferase-to-lymphocyte ratio.
![]()
Prognostic factors for late IHRFS at three and six months after the initial treatment and change from baseline
Table 3 shows the probable prognostic factors for late IHRFS at three and six months after the initial treatment and the change from baseline. In the multivariable analysis including baseline significant factors that did not change after initial treatment, mALBI grade (2a vs. 1, P = 0.02; HR, 1.33; 95% CI, 1.04–1.70; 2b/3 vs. 1, P = 0.03; HR, 1.42; 95% CI, 1.03–1.94) and increment of PLR than baseline (P = 0.001; HR, 1.01; 95% CI, 1.00–1.01) at three months showed statistically significant correlations with prognosis of late IHRFS with older age, male sex, liver cirrhosis and type of initial treatment.
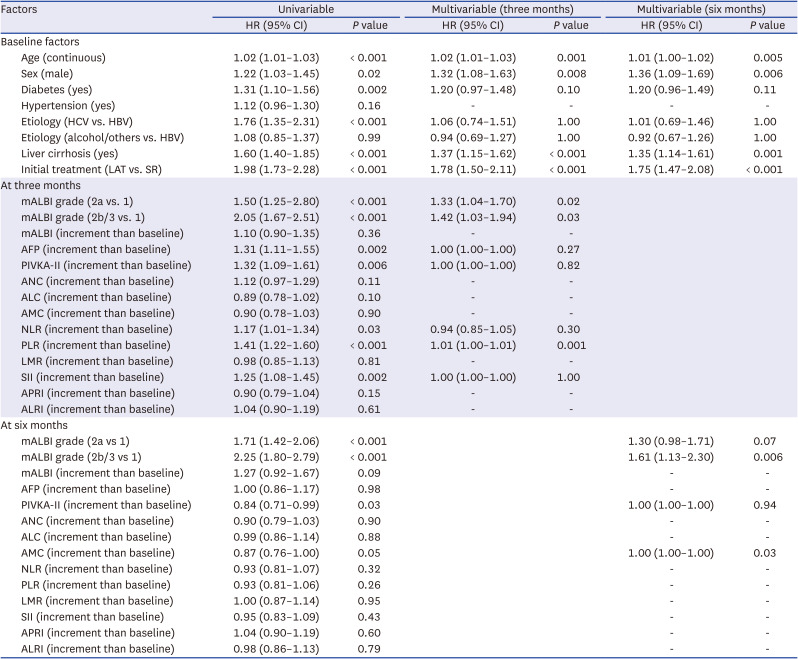
Table 3
Univariable and multivariable analysis of late intrahepatic recurrence-free survival and factors of baseline and at three and six months after initial curative treatment
HR = hazard ratio, CI = confidence interval, HCV = hepatitis C virus, HBV = hepatitis B virus, LAT = local ablation therapy, SR = surgical resection, mALBI = modified albumin-bilirubin, AFP = α-fetoprotein, PIVKA-II = protein induced by vitamin K antagonist-II, ANC = absolute neutrophil count, ALC = absolute lymphocyte count, AMC = absolute monocyte count, NLR = neutrophil-to-lymphocyte ratio, LMR = lymphocyte-to-monocyte ratio, PLR = platelet-to-lymphocyte ratio, SII = systemic immune-inflammation index, APRI = aspartate aminotransferase-to-platelet ratio, ALRI = aspartate aminotransferase-to-lymphocyte ratio.
![]()
In the multivariable analysis at six months including baseline significant factors that did not change after the initial treatment, mALBI grade (2b/3 vs. 1, P = 0.006; HR, 1.61; 95% CI, 1.13–2.30) at six months and increment of AMC than baseline (P = 0.03; HR, 1.00; 95% CI, 1.00–1.00) at six months showed statistically significant correlations with older age, male sex, liver cirrhosis and type of initial treatment.
The probable prognostic factors for OS at three and six months after the initial treatment and changes from baseline are shown in Supplementary Table 2. In the multivariable analysis, age, etiology related with alcohol or others, liver cirrhosis, and type of initial treatment were significant prognostic factors of OS with mALBI grade 2b/3 at baseline before initial treatment.
The outcomes of comparing the mALBI grades at three and six months with those at 24 months (total of 2,152 patients whose laboratory results were assessable within a window period of 8 weeks) after the initial curative treatment are presented in Supplementary Table 3. Approximately 70% of patients at three months and 60% at six months with mALBI grade 2a, and 25% to 30% of patients with grade 2b/3, showed improvement in mALBI grade to grade 1 at 24-months after curative treatment.
mALBI grade as a valid prognostic factor for late IHRFS after curative treatment
In all patients, the mALBI grade at baseline, three months, and six months after the initial curative treatment was a statistically significant prognostic factor for late IHRFS (Fig. 2). At all time points, late IHRFS was higher in patients with mALBI grade 1, but there was no difference between mALBI grades 2a and 2b/3 at baseline; however, there was a difference between the two groups at three and six months after initial treatment. In the subgroup analysis according to the initial treatment method, late IHRFS was reversed between baseline mALBI grade 2a and 2b/3 in the surgery subgroup, and there was no definite difference between mALBI grade 2a and 2b/3 at six months after initial treatment of the LAT subgroup (Supplementary Fig. 2). The prognostic significance of the mALBI grade at three months, and six months after the initial curative treatment as well as at baseline was also confirmed in univariable and multivariable OS analyses (Supplementary Table 4).
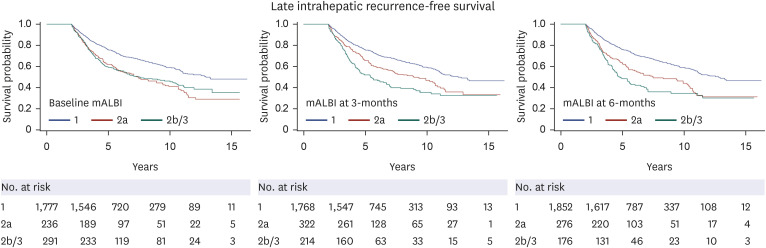
Fig. 2
Late IHRFS according to mALBI grade at baseline, 3- and 6-months after initial curative treatment. At all-time points, mALBI grade was significant prognostic factors of late IHRFS. There was, however, no difference between mALBI grade 2a and 2b/3 at baseline.
IHRFS = intrahepatic recurrence-free survival, mALBI = modified albumin-bilirubin.
![]()
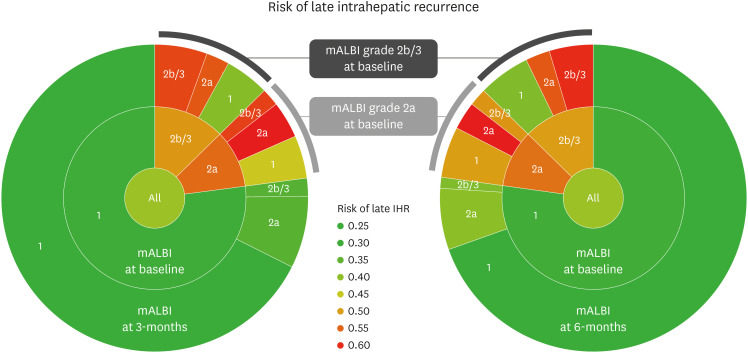
The risk of late IHR is shown as a nested pie plot in Fig. 3. There was a large difference in the risk of late IHR according to baseline mALBI grade and at three and six months after the initial treatment. In particular, late IHR occurred in more than 50% of cases where mALBI grade 2a or 2b/3 remained unchanged or worsened at three to six months after baseline. In the subgroup analysis according to the initial treatment method, the surgery subgroup tended to have fewer late IHR than the LAT subgroup; however, the pattern of higher risk in patients with mALBI grade 2a or 2b/3 either at baseline and three or six months after the initial treatment was similar (Supplementary Fig. 3).
DISCUSSION
In the current study, which assessed prognostic factors for late IHR following curative treatment in newly diagnosed very early or early-stage HCC patients who did not show early IHR, the mALBI grade demonstrated a significant correlation with the risk of late IHR, not only at baseline but also at three and six months after the application of initial curative treatment.
Through the application of active screening programs in high-risk patients with HCC, including those with chronic hepatitis and/or liver cirrhosis, the detection and diagnosis of early stage HCC are increasing.5 Long-term survival can be expected by applying curative treatment methods such as surgery, LAT, and transplantation in the case of early HCC, such as BCLC stage 0, defined as a 2 cm or less solitary lesion, or BCLC stage A, defined as up to three lesions not larger than 3 cm.34 Although curative treatment methods exhibit high local tumor control, the deterioration of liver function associated with early and late IHR and the subsequent implementation of salvage treatment continue to pose significant challenges in improving treatment outcomes for HCC.9
Numerous studies have identified the tumor burden and biological aggressiveness of primary tumors as prognostic factors for early IHR.131415 Studies evaluating the efficacy of adjuvant treatment in high-risk HCC after curative treatment have failed, but a recent phase III randomized trial, the IMbrave 050 trial, evaluating the efficacy of atezolizumab and bevacizumab in the adjuvant setting for HCC after curative treatment in liver cancer accompanied by high-risk features, showed superiority in terms of recurrence-free survival compared with active surveillance.16
Late IHR, reported to account for more than 90% of recurrences that occur two years after curative treatment of HCC, is thought to be related to de novo development, independent of previously treated tumors.17 Liver cirrhosis, which creates a vulnerable environment for HCC carcinogenesis along with the accumulation of genetic aberrations due to the rapid turnover of hepatocytes in a setting of chronic inflammation, represents the primary underlying cause of late IHR.9 In this respect, liver stiffness, esophageal varices, and splenic volume, which indicate the severity of cirrhosis, have also been identified as prognostic factors for late IHR.1819 In addition, old age and male sex were risk factors for late IHR as baseline characteristics.1720 The viral load of hepatitis B virus (HBV) and/or the level of HBV surface antigen are also associated with late IHR, and it has also been confirmed that effective control of the virus reduces HCC recurrence, including late IHR, in these risk groups.1721 Additionally, associations between late IHR and primary tumor size, number of tumors, tumor marker levels, and surgical resection have been suggested.9
In the current study, late IHR was observed in 35.4% of early-stage HCC patients, which intriguingly aligns with a previous Korean report indicating a rate of 33.2%.7 Similar to previous studies, old age, male sex, and surgical resection were significant prognostic factors of late IHR. Interestingly, other prognostic factors suggested by previous studies, including tumor marker level, primary tumor size, number of tumors, and BCLC stage, were not associated with late IHR. In addition, baseline values and changes in PLR and LMR after treatment, which can be associated with baseline liver conditions, systemic immunity, and/or inflammation, were associated with late IHR. The mALBI grade at baseline and at three and six months after curative treatment was identified as one of the most important prognostic factors for late IHR in the present study.
Compared to the MELD score and Child-Pugh grade, which are well-recognized and validated prognostic factors of liver cirrhosis and portal hypertension undergoing surgery for variceal bleeding, the ALBI grade can provide an objective, simple, and straightforward assessment of liver function without the subjectivity of clinical symptoms by classifying risk groups using only a combination of the albumin and bilirubin levels. In addition, MELD has been mainly studied for its prognostic relationship with the postoperative course rather than the prognosis of HCC. And, Child-Pugh classification has been confirmed to be useful in HCC, but it is limited only in patients with poor liver function except A grade good liver function with a score of 5 or 6. On the contrary, ALBI grade showed superior ability to distinguish prognosis even in subgroup of Child-Pugh grade A in HCC.22
Consequently, the mALBI grade was reclassified into four through the subdivision of mALBI grade 2 to 2a and 2b, and its clinical effectiveness has been confirmed and validated.2324 In a previous study, the authors suggested an association between the ALBI grade and NLR, PLR, and LMR, which are known to be associated with immunity and inflammation, and their clinical significance.11 In a situation where immunotherapy is becoming a critical part of HCC management, the mALBI grade is not only an important measurement factor of liver function itself, but also has the potential to reflect systemic nutritional and immune status. Further research is needed to explore the potential of the mALBI grade in this aspect.
In the present study, the number of patients with grade 3 mALBI was limited; therefore, grade 3 was combined with grade 2b mALBI for statistical analysis. Compared with the late IHR rate of 35.4% among patients, the IHR rate was even higher than 50% in the case of baseline mALBI grade of 2a or 2b/3; however, it was confirmed that the risk decreased to about 40% in the case of mALBI improvement to grade 1. Additionally, it was confirmed that the late IHRFS of the grade 2 or higher group was significantly worse than that of the mALBI grade 1 group at three months and six months after curative treatment. Considering the risk of late IHR as well as the liver function itself, it may be necessary to modify the management plan for these patients, such as more active follow-up and/or considering planned, earlier liver transplantation, or designing more efficient drugs.
The present study has several unavoidable limitations as a retrospective study of a single tertiary institution in an HBV-endemic country. The possibility of selection bias and the lack of external validation are major obstacles to generalizing the results of this study. In particular, approximately 80% of the patients enrolled in the present study have a history of underlying HBV, therefore, external validation studies targeting HCC patients related to HCV, alcoholic, steatohepatitis, and other causes are required. Despite these limitations, the results of this study could be highlighted through the prospectively well-designed collected data of various laboratory tests conducted under strict quality control of national regulations and a long-term follow-up of more than five years of a relatively large number of patients.
 XML Download
XML Download