

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Despite considerable efforts, Plasmodium vivax malaria remains a major infectious disease worldwide, including in South Korea.12 Unexpected global uptrends of malaria have also been reported recently.3 The life cycle of P. vivax includes a dormant stage in the liver called the hypnozoite, which can be activated, causing relapse weeks, months, or years after the initial infection.4 Although the relapse rate of P. vivax malaria in temperate regions, including South Korea, is lower than that in tropical regions, it is a significant obstacle to eliminating P. vivax malaria.5
Therefore, presumptive anti-relapse therapy is required to prevent relapses by eradicating the dormant hypnozoite liver stage of P. vivax.6 Traditionally, primaquine has been used in combination with chloroquine to prevent the relapse of P. vivax malaria.7 However, because the medication needs to be taken continuously for two weeks to be effective, some patients may have problems with medication adherence, creating a major barrier to primaquine effectiveness.8910 To overcome this, clinical studies on alternative dosing schedules for primaquine such as 7-day regimens have been conducted.1112 However, low adherence in unsupervised patients remains a predominant cause of the limited effectiveness of this drug.
Tafenoquine, developed to overcome the shortcomings of primaquine and approved by the US Food and Drug Administration (FDA) in 2018, removes hepatic hypnozoites following a single dose and has proven effective in clinical trials and Cochrane Review.13141516 Tafenoquine could be used to surmount adherence problems because of its convenience of administration, and therefore, it can be utilized as chemoprophylaxis when traveling.171819 This treatment strategy could also prevent relapse and reduce the overall incidence of P. vivax malaria in the real world, where it is difficult to supervise primaquine administration.20 Meanwhile, in the case of glucose-6-phosphate dehydrogenase (G6PD) deficiency, hemolysis could occur when using tafenoquine, so a G6PD test is mandatory before the tafenoquine prescription.21
Modeling studies have investigated the effect of introducing tafenoquine into the treatment regimen of patients with P. vivax malaria. The impact of intervention strategies on controlling the burden of the P. vivax malaria relapse was explored in South Korea and Brazil.2223 Few studies have compared the cost-effectiveness of tafenoquine and primaquine for the prevention of P. vivax malaria relapse in Serbia and other countries using the Markov or decision tree models.2425 However, a comprehensive economic evaluation of the potential benefits of tafenoquine introduction based on a dynamic model for P. vivax malaria transmission is lacking.
In our previous study, we developed a dynamic compartmental model for P. vivax malaria transmission to estimate the impacts of introducing rapid diagnostic tests (RDTs) on disease burden and medical expenditure.20 In addition, we performed a cost-benefit analysis of RDT in South Korea.26 The model was elaborately calibrated to fit overall weekly malaria incidence, the sum of incidences after short and long latency periods and relapse. However, although it is less distinctive than the primary infection, relapse intervals are also divided into a short and long period.522 A recent study analyzed characteristics of recurred patients between 2005 and 2009 when the same treatment regimen was administered as now, and they had experienced either short or long latency periods.27
Therefore, in this study, we expanded our previous model by dividing relapse latency into short and long periods and assessed the effects of introducing tafenoquine as a treatment strategy for relapse and overall P. vivax malaria incidence. In addition, we analyzed the medical costs of tafenoquine treatment and performed a cost-benefit analysis from the payer’s perspective.
METHODS
Study design and data sources
Based on the study that analyzed characteristics of recurred patients,27 we calculated average short and long latency periods of relapse patients to expand our previous model.26 We split one relapse flow into two in the model and assigned the calculated average short and long latency periods. A relapse was defined as a case in which the period from the previous malaria diagnosis to the current diagnosis was less than two years, and there was no possibility of a new malaria infection since the last disease.28 Weekly civilian malaria incidence data in malaria-risk areas (Incheon, Gyeonggi, and Gangwon provinces) were used for model calibration. We only included Korean civilians and excluded military soldiers, who account for about one-third of P. vivax malaria incidence because military soldiers at malaria-risk areas take chloroquine chemoprophylaxis to prevent P. vivax malaria infections. We constructed scenarios for the use of primaquine and tafenoquine based on the relapse probability. The relapse probability of primaquine was obtained from an annual report of the Korea Centers for Disease Control and Prevention (KCDC),28 and we varied the relapse probability of tafenoquine.
In South Korea, a low dose of primaquine (0.25 mg/kg for 14 days) is effectively used,2829 so we calculated the cost of primaquine when 15 mg was used for 14 days. The increase in cost due to the introduction of tafenoquine into the treatment strategy includes the price of tafenoquine and the G6PD rapid diagnostic test in South Korea. The benefit of introducing tafenoquine was a reduction in medical expenditure associated with its prevention of relapse and secondary cases. Furthermore, the values were extracted from the Health Insurance Review & Assessment Service (HIRA) data, which is a mandatory nationwide insurance database for all Korean citizens enrolled. The reliability of the data from the HIRA has been demonstrated in previous studies.303132
We then predicted the 10-year relapse and overall malaria incidences in each scenario and compared the estimated number of prevented cases between primaquine and tafenoquine scenarios. We conducted the cost-benefit analysis using the net present value (NPV), benefit-cost ratio (BCR), and incremental benefit-cost ratio (IBCR) as indicators and examined the sensitivity of the IBCR to model parameters, costs, and benefits.
Modeling and interventions
We propose a modified P. vivax malaria model to account for relapse incidence by separating the relapse latency period into short and long, as shown in Supplementary Fig. 1. The human population was categorized into susceptible, exposed, infectious, and treated states, and the mosquito population was divided into the aquatic, susceptible, exposed, and infectious states. The malaria parasite is transmitted when an infectious mosquito bites a susceptible human or a susceptible mosquito bites an infectious human. In this study, the term “transmission” refers to introducing parasites in the human or mosquito body, and when the transmission occurs, the human and mosquito are said to be infected.
Following infection with the parasite, humans undergo a short or long latency stage and become infectious. We assumed that all infected individuals were treated and prescribed chloroquine and primaquine. Failure to complete the drug course leads to a chance for hypnozoites to persist in the liver. As a result, some patients do not recover fully and relapse. Full model equations are shown in Supplementary Data 1.
Three parameters were estimated by fitting the model to the weekly civilian malaria incidence between 2014 and 2018 using maximum likelihood estimation. Descriptions and estimated values of the three parameters are listed in Supplementary Table 1, including the other model parameters, and the result of the model calibration is shown in Supplementary Fig. 2.
RDT was included in all scenarios because it has been covered by insurance in South Korea since 2019. Both primaquine and tafenoquine for relapse prevention are used with treatment doses of chloroquine. In the primaquine scenario, the relapse probability was set to 0.04, reflecting the current level of relapse in South Korea.2833 In the tafenoquine scenarios, since the relapse prevention when taking tafenoquine is comparable to that when taking primaquine,1516 and potential benefits are expected from improvement in adherence, we assumed four different relapse probabilities decreasing from 0.04 to 0.03, 0.02, and 0.01 due to improved drug adherence. All scenarios were simulated over 10 years from 2019 to 2028.
Cost-benefit analysis
Tafenoquine is more expensive than primaquine, and a G6PD deficiency test must be performed before tafenoquine is prescribed. However, since the prevalence of G6PD deficiency is low in South Korea, this test is not routinely conducted.34 Therefore, the incremental cost of replacing primaquine with tafenoquine would be considerable. However, a decrease in the relapse probability would be accompanied by the prevention of new malaria infections, which would lead to savings on medical costs for treatment. Thus, in the cost-benefit analysis, we included only the treatment drug and G6PD test costs as cost factors, defined the medical cost per malaria episode as a benefit per prevented case, and obtained the value from the HIRA data.
We set two primaquine comparator scenarios. One included only the price of primaquine, reflecting the current situation in South Korea, and the other included the cost of both primaquine and G6PD for the hypothetical situation. As a measure for the cost-benefit analysis, we estimated the NPV and BCR for each scenario and estimated the IBCR of tafenoquine use compared to primaquine use. All monetary values are presented in US dollars based on the 2019 yearly average exchange rate of ₩1,165.65 per dollar and are discounted by 3% annually.
Sensitivity analysis
The probabilistic sensitivity analysis of the IBCR was performed to account for the effect of uncertainty in model parameters, costs, and benefits on the results, and 1,000 values were sampled for each parameter assuming a uniform distribution over a selected range of each parameter. We then simulated the model to obtain a projected IBCR in 2028 for each set of samples. First, a univariate sensitivity analysis of the relative sensitivity of all parameters was performed by perturbing ± 10% of each value.
Next, we selected 14 parameters based on the relative sensitivity and interest level and determined a feasible range or distribution for each selected parameter. We performed another univariate sensitivity analysis to examine the practical sensitivity of the result under the feasible range or distribution. In addition, the following pairs of parameters of interest were chosen for bivariate sensitivity analysis: relapse probabilities of primaquine and tafenoquine and cost and benefit of tafenoquine. Finally, all parameters were perturbed simultaneously to evaluate the model sensitivity to multiple parameters.
RESULTS
Malaria incidence
The relapse incidence of P. vivax malaria decreased over time with the introduction of the RDT even under the primaquine scenario, as shown in Fig. 1. In the tafenoquine scenario, noticeable reductions in the relapse incidence were observed only when its relapse probability was lower than that of primaquine. These reductions were proportional to the decrease in the relapse probability due to the tafenoquine use, which contributed to a drop in the total malaria incidence in two ways: directly by a reduction in the number of relapse cases and indirectly by a reduction in secondary cases owing to relapse patients, as shown in Table 1. The most effective tafenoquine scenario assuming a relapse probability of 0.01 showed that tafenoquine prevented 35 (77.78%) cases of relapse malaria and 129 (12.27%) total malaria cases for a decade whereas it had no preventative effect at the same relapse probability with primaquine.
Fig. 1
Annual relapse incidences based on relapse control scenario.
PQ = primaquine, TQ = tafenoquine, q = relapse probability.
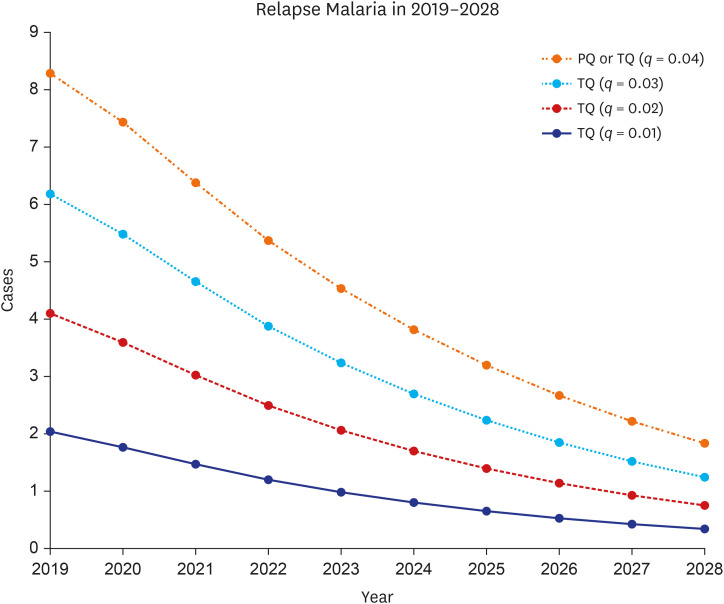
Table 1
Accumulated relapse and total malaria cases over 10 years

Cost-benefit analysis
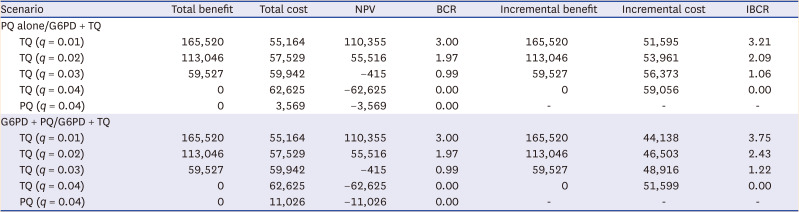
The prices of tafenoquine, G6PD rapid diagnostic testing, and 14-day primaquine treatment were calculated as $57.37, $7.76, and $3.71, respectively. The average medical expenditure per malaria patient was extracted to be $1,444.79. In the primaquine scenario with a relapse probability of 0.04, the total cost accumulated for all patients over the decade was $3,569 considering only the price of primaquine and $11,026 considering both primaquine and G6PD testing prices, as shown in Table 2. In contrast, in the tafenoquine scenario, the total cost was $62,625 and $55,164 as the relapse probability decreased from 0.04 to 0.01. When tafenoquine had the same relapse probability as primaquine, there was no benefit, and when the relapse probability decreased to 0.03, the total benefit was positive but slightly less than the total cost, resulting in a negative NPV and a BCR < 1. However, as the relapse probability decreased to 0.02 and 0.01, the total benefit was nearly 2- and 3-fold greater than the total cost. Therefore, the NPV of the tafenoquine scenario turned into a positive number, and BCR became > 1. The incremental benefits of tafenoquine treatment were greater than the incremental costs for all relapse probabilities of tafenoquine except for those with the same relapse probability as primaquine. Under a relapse probability of 0.01 of tafenoquine use and primaquine scenario accounting for the cost of primaquine alone, the IBCR was 3.21 after 10 consecutive years.
Table 2
Total costs and benefits and cost-benefit analysis over the next 10 years
Probabilistic sensitivity analysis
Univariate sensitivity
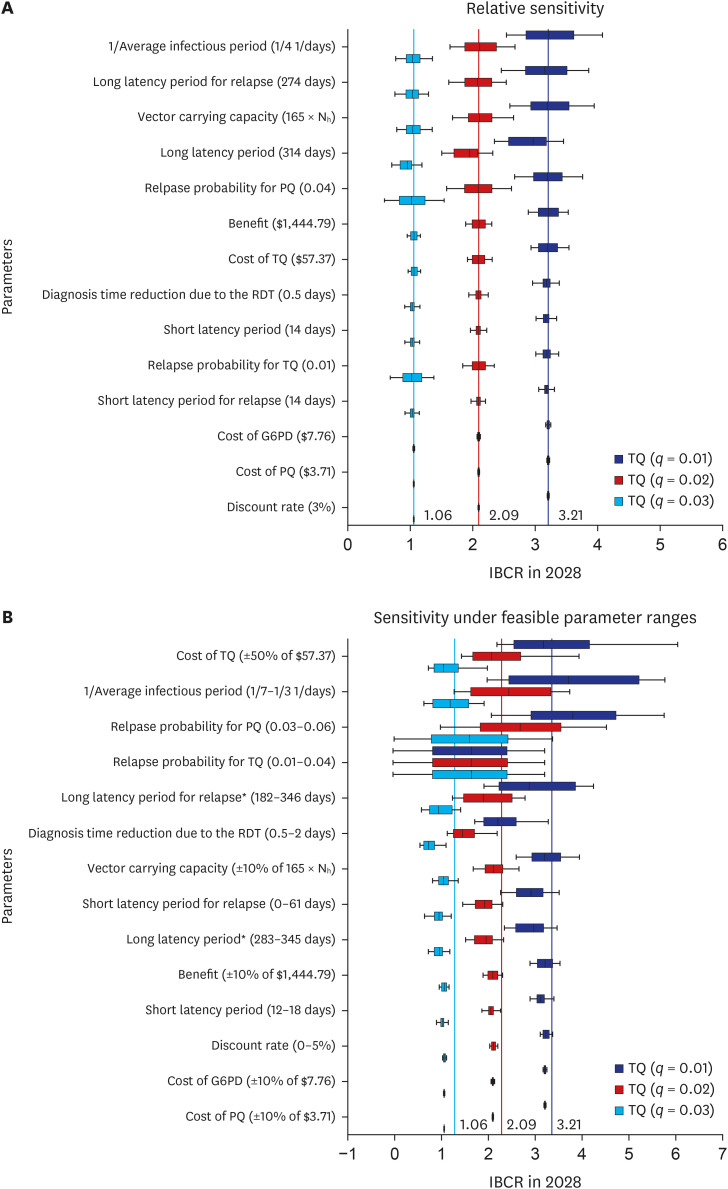
We performed the sensitivity analysis on the IBCR values obtained in each tafenoquine scenario. The average infectious period; long latency period for relapse; and vector carrying capacity, which means the size of the mosquito population, were the three most relatively sensitive parameters for the IBCR in 2028, as shown in Fig. 2A. Under feasible ranges of the parameter, as shown in Fig. 2B, the cost of tafenoquine became the most sensitive parameter as we set up a comprehensive test range. The average infectious period and long latency period for relapse remained sensitive parameters, but the relapse probability of primaquine and tafenoquine became more sensitive to the result.
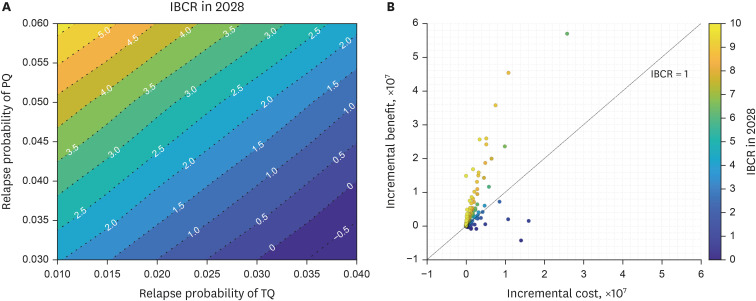
Fig. 2
Tornado box plots of univariate sensitivity. (A) Relative sensitivity of IBCR for each TQ scenario and (B) Sensitivity of IBCR under feasible parameters ranges for each TQ scenario.
G6PD = glucose-6-phosphate dehydrogenase, IBCR = incremental benefit-cost ratio, PQ = primaquine, RDT = rapid diagnostic tests, TQ = tafenoquine.
Additionally, for the cost- and benefit-related parameters, we further examined a threshold that made the IBCR in 2028 ≥ 1, indicating that the incremental benefit was greater than or equal to the incremental cost. We achieved an IBCR ≥ 1 when the cost of tafenoquine was ≤ $191.87, $124.26, and $60.80 or the benefit, which was the saved medical cost from preventing one malaria case, was ≥ $450.37, $689.65, and $1,368.25 at 0.01, 0.02, and 0.03 tafenoquine relapse probabilities, respectively.
Bivariate sensitivity
We explored the combined effect of primaquine and tafenoquine relapse probabilities on the IBCR and illustrated it with a contour graph in Fig. 3A. As demonstrated in the main results, the IBCR = 0 when both relapse probabilities are the same, and IBCR < 0 as tafenoquine relapse probability became higher than primaquine. Tafenoquine was beneficial as long as the difference in the relapse probability from that of primaquine was ≥ 0.01. Additionally, we examined sensitivity under changes in tafenoquine cost and benefit for each tafenoquine scenario, as shown in Supplementary Fig. 3. The IBCR increased when the benefit increased, and the cost of tafenoquine decreased.
Multivariate sensitivity
Finally, uncertainties of all parameters, including relapse probabilities of primaquine and tafenoquine, were simultaneously assessed and each result was scattered on a cost-benefit plane, as shown in Fig. 3B. Among the results of 1,000 combinations of the parameters, 69.1% were above an IBCR of 1.
DISCUSSION
In this study, we expanded a previously developed P. vivax malaria transmission model to consider relapse in detail. Model simulations were performed to investigate the effect of introducing tafenoquine into the treatment regimen for P. vivax malaria relapse and total incidence, as well as medical expenses over the next decade from 2019 to 2028. The results suggested the potential advantage of tafenoquine introduction for suppressing P. vivax malaria relapse and total incidence and reducing overall medical expenses.
According to the study that synthesized the results of the phase 3 trial on the efficacy of tafenoquine and primaquine, the risk of relapse at 6 months was non-significantly higher for tafenoquine compared with primaquine (33.0% vs. 27.2%), with an odds ratio of 1.81 (95% confidence interval, 0.82–3.96).1315 However, while the group taking primaquine in these trials was a highly adherent population, a real-world study showed that adherence to primaquine is only 23.8%.35 Therefore, the real-world effectiveness of tafenoquine is expected to be at least equal to or better than primaquine.16 The drug information for tafenoquine and primaquine is presented in Supplementary Table 2. In this study, we constructed the scenarios considering these factors.
The relapse probability in the primaquine scenario was set to 0.04 based on the relapse incidence data reported by the KCDC,2833 but no relapse probability data was available for the tafenoquine scenario; therefore, we assumed it to be 0.01 to 0.04. Low adherence to primaquine is presumed to be the leading cause of relapse in South Korea because it is impossible to supervise treatment adherence under real-world conditions. The introduction of tafenoquine is expected to improve adherence significantly, and therefore, we set the relapse probability with tafenoquine use at 0.01–0.04 to determine the contribution of tafenoquine use to controlling the actual relapse and total incidence of P. vivax malaria. The result showed that under the assumption of a relapse probability of 0.01 with tafenoquine use, 77.78% of relapses and 12.27% of all P. vivax malaria incidence could be prevented in 10 years. Thus, the introduction of tafenoquine could contribute to returning South Korea to malaria elimination status. Indeed, if South Korea returns to malaria elimination status, the real source of reinfection would presumably be North Korea. Accordingly, we have conducted a follow-up study to distribute RDT and tafenoquine to North Korea and simulate its effect on malaria incidence.
In addition to the adherence issues associated with primaquine, the cytochrome P450 (CYP) 2D6 enzyme may be crucial for its anti-malarial efficacy.3637 Therefore, low CYP2D6 metabolism may result in treatment failure in patients with P. vivax malaria.38 A report also confirms impaired CYP2D6 function in a patient with four relapses of P. vivax malaria despite primaquine treatment in Korea.39 In contrast, previous studies have shown that low CYP2D6 metabolism did not appear to be associated with relapse in patients with tafenoquine use.4041 Therefore, this is another advantage of tafenoquine over primaquine. In addition, primaquine interacts with quinacrine and myeloid suppressive drugs; this increases primaquine toxicity. Therefore, the manufacturer contraindicates their concomitant use.42 In this case, using tafenoquine could also overcome these issues.
Although the medical necessity of introducing tafenoquine treatment to prevent relapse by improving adherence is acknowledged, further investigations into the economic benefits of tafenoquine are required for its widespread use instead of primaquine. This is because the price of tafenoquine is much higher than that of primaquine. In particular, because the prevalence of G6PD deficiency is low in South Korea, primaquine may be prescribed without G6PD testing, which must precede tafenoquine use, inevitably contributing to an increase in cost.434445 Therefore, a cost-benefit analysis comparing the additional cost of tafenoquine use and the expected decrease in medical expenditure with the reduction of patients is essential to predict the burden of medical expenses resulting from long-term drug use. To this end, we calculated the cost of tafenoquine, primaquine, and G6PD testing and extracted the average incurred medical cost per patient with P. vivax malaria by analyzing HIRA data. Furthermore, the cost-benefit analysis results showed that the introduction of tafenoquine could be economically beneficial. If South Korea needs to use a high dose of primaquine (0.5 mg/kg for 14 days), such as Southeast Asia and Oceania,629 the benefit of using tafenoquine could be more significant than using primaquine since the cost of primaquine increases when high-dose primaquine is used. The cost-benefit analysis results when G6PD testing was conducted before prescribing primaquine, as recommended by the World Health Organization, also proved it was beneficial. If the G6PD test is not mandatory when using tafenoquine, the benefit of using tafenoquine could be more significant.
Moreover, the sensitivity analysis verified that introducing tafenoquine is beneficial over primaquine under a feasible range of parameters. As the price of tafenoquine may vary by country, we fluctuated the price considerably in the sensitivity analysis. As the relapse probability of tafenoquine decreased up to 0.01, its introduction was beneficial at tafenoquine cost ≤ $191.87. Regarding the relapse probabilities of the two regimens, we confirmed that tafenoquine was beneficial when its relapse probability was lower than that of primaquine by at least 0.01 in the bivariate sensitivity analysis. In addition, evaluating the simultaneous impact of uncertainty in multiple parameters showed that the tafenoquine was beneficial at 69.1%.
This study has several strengths; the first is that this newly updated model elaborately reflects the relapse latency periods by expanding the previously developed mathematical P. vivax malaria model. Second, the model was calibrated to the actual malaria incidence data, and the monetary values used in this study were based on actual data, including that of the HIRA database. Therefore, the model simulations allowed us to estimate the impact of tafenoquine use on the relapse and total incidences of P. vivax malaria, as well as national medical expenditures. Lastly, the sensitivity analysis demonstrated the robustness of the result under uncertainties of the model parameters, costs, and benefits.
Despite these strengths, this study has some limitations that are worth mentioning. First, the relapse probability of P. vivax malaria with tafenoquine use was assumed in the simulation. As tafenoquine has not been used in South Korea, we assumed the relapse probability of its use by considering the probability and the causes of relapse with primaquine use. To overcome this limitation, we evaluated the incidences and economic feasibility under several different scenarios by changing the relapse probability of tafenoquine. We also performed the bivariate sensitivity analysis of the various combinations of tafenoquine and primaquine relapse probabilities. Second, the cost of tafenoquine, G6PD testing, and primaquine and the medical expenditure per malaria patient used in the cost-benefit analysis may vary by country. Thus, we described how the economic feasibility could change according to price changes in the sensitivity analysis.
In conclusion, the introduction of tafenoquine could reduce P. vivax malaria relapse and total incidence. The cost-benefit analysis and the sensitivity analysis also suggested the potential advantage of using tafenoquine under uncertainties. These results support the need to adopt and use tafenoquine to eliminate P. vivax malaria in South Korea.
 XML Download
XML Download