

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Knee osteoarthritis (OA), the most common form of arthritis affecting older people, is a growing public health problem associated with population aging.1 Although knee pain due to OA is a key symptom influencing the decision to seek medical attention, radiographic OA changes are poorly correlated with pain and physical function.2 With the advent of sophisticated imaging, such as magnetic resonance imaging (MRI), noninvasive examination of pathologic changes in the joint and periarticular structures of the knee, which sometimes correlate with symptoms, is possible. Although MRI shows high sensitivity and specificity for the detection of abnormalities in the articular soft tissues,3 clinical significance of such lesions detected by MRI is in many cases unclear, and even consensus on when to perform MRI in knee OA subjects is not reached.
In previous studies of middle-aged and elderly men and women representative of the general population, incidental meniscal findings on MRI of the knee were common, and the majority of meniscal damage was found in persons without knee symptoms.4 In addition, meniscal damage was not significantly associated with the presence of knee pain or its severity among subjects with radiographic knee OA.5 These data suggest that compared to traumatic meniscal tears, where arthroscopic repairs show a high success rate in terms of functional outcome and cartilage protection, the therapeutic efficacy of arthroscopic surgery for degenerative meniscal tears may not be high. The number of knee arthroscopic surgery has grown rapidly along with the introduction of MRI, which reveals a high prevalence of meniscal tears in OA, and there is a possibility that surgery is performed to resect meniscal lesions that may not be the cause of symptoms.6 Although arthroscopic partial meniscectomy (APM) is one of the most common types of knee surgery7; evidence of its efficacy lags behind.
Rigorous outcome studies conducted after the 2000s began to shed light on the clinical value of arthroscopic surgery. Randomized controlled trials (RCTs) of arthroscopic management of degenerative meniscal tears showed that surgery was no better than physical therapy (PT) or even a sham surgery in improving pain or functional status.89 However, studies were heterogeneous in terms of study subjects, including those with and without radiographic knee OA and type of surgical treatment, including different modalities such as meniscectomy, debridement, synovectomy, or chondroplasty. This study aimed to determine the clinical effectiveness of APM compared with non-operative care in patients with knee OA. A systematic review (SR) of the literature was first performed to identify gaps in the existing evidence, and then quantitative synthesis of the extracted data was attempted.
METHODS
The literature search for existing SRs was conducted according to the method of the Cochrane Handbook10 and was reported following the Preferred Reporting Items for Systematic Review and Meta-Analyses.11 The protocol for this SR was registered in PROSPERO (CRD42020215965) on December 11, 2020.
Step 1. selection of existing SRs
We intended to use existing SRs for effectiveness in this review. In this step, existing SRs were searched and selected according to the eligibility criteria of the new SR. Their quality assessment was performed, and primary studies included in those SRs were selected if they conformed to the objective of the new SR accordingly.
Information sources and search strategy
A search through Ovid-Medline, Cochrane Library, and Epistemonikos was performed, without limitations of language and publication date. The search terms included knee OA, meniscal tear, and meniscectomy. Studies that met the following criteria were included: a) studies including knee OA patients with meniscal degeneration; b) those with an intervention arm including APM; c) RCTs and comparative observational studies; and d) those reporting patient outcomes including function, pain, and quality of life by using validated assessment tools such as the Western Ontario and McMaster Universities Arthritis Index (WOMAC), Knee Injury and OA Outcome Score (KOOS), Arthritis Impact Measurement Scales (AIMS), and visual analog scale (VAS) and total knee replacement (TKR) surgery. Studies on animal or pre-clinical studies, review articles, editorials, letters, and comments were excluded. Studies with duplicate subjects (studies using the same outcome indicators published in duplicate) were also excluded. The search was performed by two independent reviewers; the complete details of which are available in Supplementary Data 1.
Study selection, quality assessment and data extraction
Two reviewers independently screened the titles and abstracts of SRs. Then, full texts were retrieved and reviewed based on the inclusion criteria, and final studies were selected by consensus. The SRs were formally evaluated for risk of bias (RoB) using the “A MeaSurement Tool to Assess SR (AMSTAR).” Two authors assessed each of the SRs; any disagreements were resolved by consensus. The extracted data included authors details, year of publication, search period, number of studies, characteristics of the participants, the intervention and comparator delivered, and the final value of outcome data. As for the selection criteria of primary studies, we included studies of adults with a diagnosis of knee OA with meniscal tear that was defined by clinical assessment and radiologic findings. The intervention included arthroscopic partial or total meniscectomy, while the comparators were sham-surgery, physical exercise, medication, and other conservative treatments. RCTs and comparative observational studies were included, while studies with other surgical comparators (e.g., repair, allograft, implant transplantation) as well as gray literature were accordingly excluded. We cross-checked all primary studies included in the SRs, and any primary studies not included in the selected SRs were then retrieved and checked for eligibility of their inclusion in this review.
Step 2. latest studies update
In this step, new primary studies published after the selected existing SRs were searched, selected, and evaluated accordingly.
Information sources and search strategy
After selection of existing SRs, we searched Ovid-Medline, Ovid-EMBASE, Cochrane Library, and Korean literature databases such as KoreaMed and KMBASE for primary studies published after searched existing SRs. We limited the publication year to one year before the last SR search year to August 12, 2020. The search was performed by two independent researchers. The entire details of this search are available in Supplementary Data 1.
Study selection, quality assessment and data extraction
Two reviewers independently screened all the titles and abstracts identified by the searches. Full manuscripts of studies screened as potentially relevant by either reviewer were obtained and assessed by two independent reviewers. Discrepancies were resolved by consensus. Finally, we pooled the relevant studies from existing SRs and those published after the existing SRs.
Two reviewers independently assessed the methodological quality of the included studies using the Cochrane RoB tool12 for RCTs and Risk of Bias for Nonrandomized Studies (ROBANS) tool13 for cohort study. The results of the RoB and ROBANS evaluations are displayed in a diagram with graphs using Review Manager version 5.4 (The Nordic Cochrane Center, Copenhagen, Denmark).
For each study, the data extraction details included the trial name and authors details, study design, number of participants and population characteristics, tear pattern or the presence of locking, intervention, comparator, and major outcomes, respectively. One reviewer extracted the study data, and the second reviewer checked the extracted data for accuracy and completeness. Disagreements were resolved by consensus.
Search results
In the first step, an existing SR search strategy identified 134 articles for screening, and after removing duplicates, we screened 100 articles by their titles and abstracts. A total of 20 full-text articles were selected, of which six were eligible for primary study selection. The study selection process is illustrated in Fig. 1. Five of the six selected SRs, most of which were recently published, received more than eight ‘yes’ evaluations in a total of 11 items of the AMSTAR tool used for quality assessment. The methodological weaknesses were the lack of including reports of the SR prior plan (i.e., protocol), conflicts of interest, and lists of excluded studies (Supplementary Table 1). The subjects included in the six SRs were heterogeneous in terms of the presence of OA (Supplementary Table 2). Primary studies that did not include patients with OA or those that did not specify the Kellgren-Lawrence (KL) grade of the included patients were excluded from the analysis. A total of 22 studies (21 RCTs, one cohort study) selected from the six SRs were finally obtained and reviewed. We excluded 19 studies from this total due to target population or intervention ineligibility, and hence, only three were finally selected.81415 The studies excluded after reviewing the primary studies from the existing SRs are listed in Supplementary Table 3.
Fig. 1
Preferred Reporting Items for Systematic Review and Meta-Analyses flow diagram. (A) Step 1: selection of existing SR. (B) Step 2: selection of latest primary articles.
RCT = randomized controlled trial, SR = systematic review.
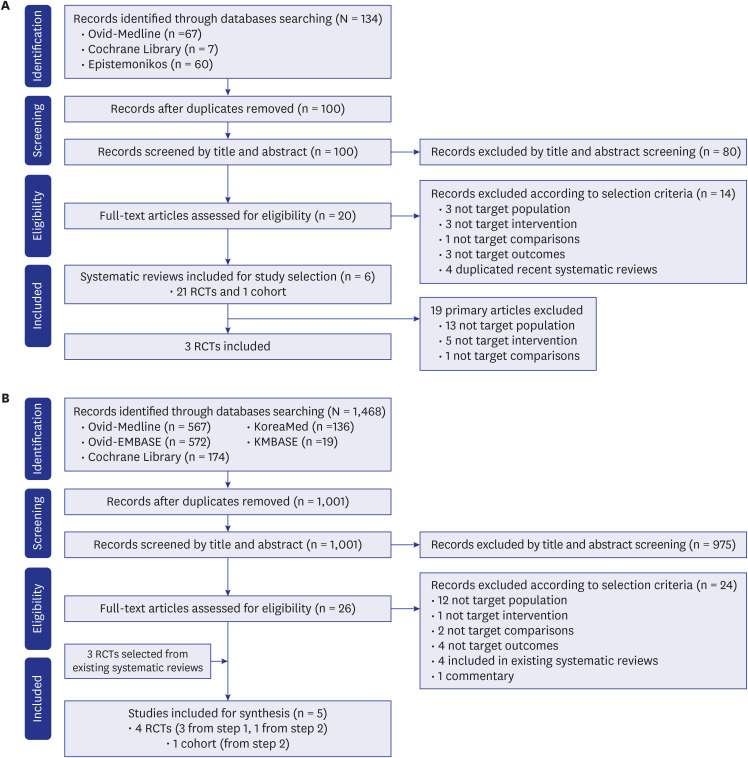
The latest primary studies were searched accordingly in the second step. For RCTs, studies published after 2018 were searched, whereas for observational studies, such limitation of publication year was not applied. A total of 1,468 studies were included, and after excluding deduplication, 1,001 articles were screened by titles and abstracts. Twenty-six studies were selected for full-text review, and two studies were finally chosen after assessment of their eligibility.1617 Three studies selected from the existing SRs were then included in the final analysis (Fig. 1). The studies excluded after reviewing the full text are listed in Supplementary Table 4.
Data analysis
Outcome variables to determine clinical effectiveness of APM were knee function, knee pain, and quality of life measured with validated assessment tools such as the WOMAC, KOOS, AIMS, and VAS. If the studies were considered clinically similar and the extracted data could be quantitatively synthesized, a meta-analysis was performed using Review Manager 5.4. When quantitative synthesis of the extracted data was not possible, we only described the results of the studies and summarized the final outcomes accordingly. Data were converted using the data conversion formula of the Cochrane Handbook, and in case of extracting data points from graphs we used Ungraph program (Biosoft, 2004). Data were analyzed to compare the effects of the APM intervention versus each of the comparators (e.g., PT, sham surgery). Continuous variables, such as mean change from baseline, median, range, and standard deviation (SD) were extracted from the studies.18 If SD was not available, it was calculated at a 95% confidence interval (CI). The standardized mean difference (SMD) was used to pool the results for continuous outcomes measured using different measures. When meta-analysis was possible, and when heterogeneity was judged to be high, a random effect model was accordingly applied. The Cochrane Collaboration's Review Manager version 5.4 was used for data analysis.
RESULTS
Finally, five studies were selected; three involved the same study population from the METEOR trial,81617 while two other studies were from different populations.1415 The characteristics of each study, such as participants, tear pattern/the presence of locking, intervention, comparison, and major outcomes are listed in Tables 1 and 2. The METEOR trial and Kirkley et al.'s trial14 compared the effects of APM plus PT with PT alone, while the ESCAPE trial compared APM alone and PT alone. The METEOR and ESCAPE trials included 21.1 and 12% of patients, respectively, with KL-grade 0, while all patients included in the Kirkley et al.'s trial14 had OA. Patients with knee locking were unanimously excluded. All studies were rated as having a high RoB in the domain of blinding of participants and personnel. Regarding ‘other bias’, the METEOR trial was rated as ‘high’ due to the high rate of cross-over after being assigned to a control group and the ESCAPE trial due to some significant differences in the baseline characteristics after randomization. In the study by MacFarlane et al.,17 which assessed the influence of baseline MRI features on the outcome of meniscectomy, the RoB was rated as low, except for the lack of blinding (Supplementary Fig. 1).
Table 1
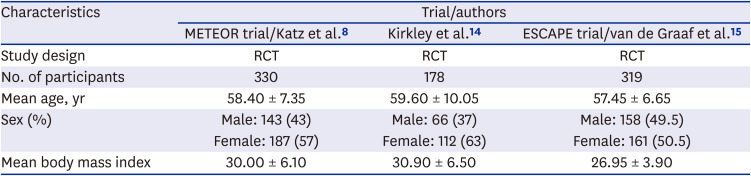
Brief demographic data
| Characteristics | Trial/authors | ||
|---|---|---|---|
| METEOR trial/Katz et al.8 | Kirkley et al.14 | ESCAPE trial/van de Graaf et al.15 | |
| Study design | RCT | RCT | RCT |
| No. of participants | 330 | 178 | 319 |
| Mean age, yr | 58.40 ± 7.35 | 59.60 ± 10.05 | 57.45 ± 6.65 |
| Sex (%) | Male: 143 (43) | Male: 66 (37) | Male: 158 (49.5) |
| Female: 187 (57) | Female: 112 (63) | Female: 161 (50.5) | |
| Mean body mass index | 30.00 ± 6.10 | 30.90 ± 6.50 | 26.95 ± 3.90 |
Table 2
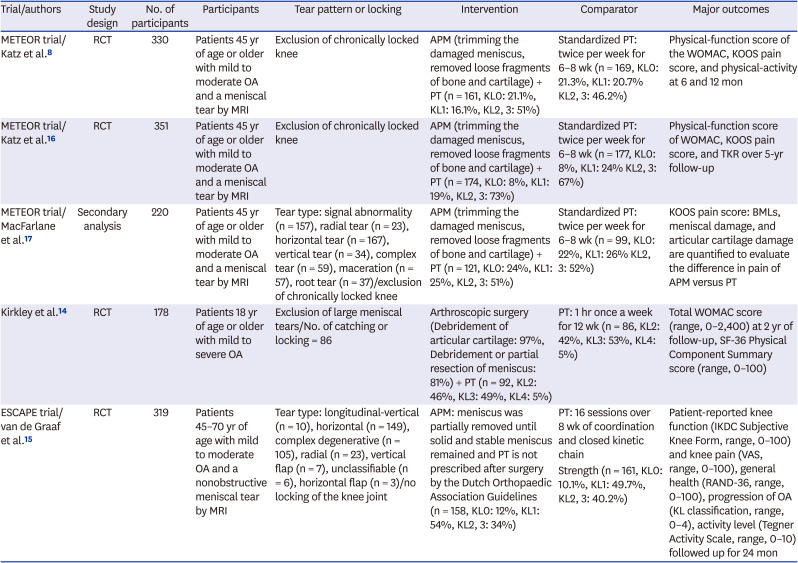
Summary of the characteristics of final studies included
| Trial/authors | Study design | No. of participants | Participants | Tear pattern or locking | Intervention | Comparator | Major outcomes |
|---|---|---|---|---|---|---|---|
| METEOR trial/Katz et al.8 | RCT | 330 | Patients 45 yr of age or older with mild to moderate OA and a meniscal tear by MRI | Exclusion of chronically locked knee | APM (trimming the damaged meniscus, removed loose fragments of bone and cartilage) + PT (n = 161, KL0: 21.1%, KL1: 16.1%, KL2, 3: 51%) | Standardized PT: twice per week for 6–8 wk (n = 169, KL0: 21.3%, KL1: 20.7% KL2, 3: 46.2%) | Physical-function score of the WOMAC, KOOS pain score, and physical-activity at 6 and 12 mon |
| METEOR trial/Katz et al.16 | RCT | 351 | Patients 45 yr of age or older with mild to moderate OA and a meniscal tear by MRI | Exclusion of chronically locked knee | APM (trimming the damaged meniscus, removed loose fragments of bone and cartilage) + PT (n = 174, KL0: 8%, KL1: 19%, KL2, 3: 73%) | Standardized PT: twice per week for 6–8 wk (n = 177, KL0: 8%, KL1: 24% KL2, 3: 67%) | Physical-function score of WOMAC, KOOS pain score, and TKR over 5-yr follow-up |
| METEOR trial/MacFarlane et al.17 | Secondary analysis | 220 | Patients 45 yr of age or older with mild to moderate OA and a meniscal tear by MRI | Tear type: signal abnormality (n = 157), radial tear (n = 23), horizontal tear (n = 167), vertical tear (n = 34), complex tear (n = 59), maceration (n = 57), root tear (n = 37)/exclusion of chronically locked knee | APM (trimming the damaged meniscus, removed loose fragments of bone and cartilage) + PT (n = 121, KL0: 24%, KL1: 25%, KL2, 3: 51%) | Standardized PT: twice per week for 6–8 wk (n = 99, KL0: 22%, KL1: 26% KL2, 3: 52%) | KOOS pain score: BMLs, meniscal damage, and articular cartilage damage are quantified to evaluate the difference in pain of APM versus PT |
| Kirkley et al.14 | RCT | 178 | Patients 18 yr of age or older with mild to severe OA | Exclusion of large meniscal tears/No. of catching or locking = 86 | Arthroscopic surgery (Debridement of articular cartilage: 97%, Debridement or partial resection of meniscus: 81%) + PT (n = 92, KL2: 46%, KL3: 49%, KL4: 5%) | PT: 1 hr once a week for 12 wk (n = 86, KL2: 42%, KL3: 53%, KL4: 5%) | Total WOMAC score (range, 0–2,400) at 2 yr of follow-up, SF-36 Physical Component Summary score (range, 0–100) |
| ESCAPE trial/van de Graaf et al.15 | RCT | 319 | Patients 45–70 yr of age with mild to moderate OA and a nonobstructive meniscal tear by MRI | Tear type: longitudinal-vertical (n = 10), horizontal (n = 149), complex degenerative (n = 105), radial (n = 23), vertical flap (n = 7), unclassifiable (n = 6), horizontal flap (n = 3)/no locking of the knee joint | APM: meniscus was partially removed until solid and stable meniscus remained and PT is not prescribed after surgery by the Dutch Orthopaedic Association Guidelines (n = 158, KL0: 12%, KL1: 54%, KL2, 3: 34%) | PT: 16 sessions over 8 wk of coordination and closed kinetic chain | Patient-reported knee function (IKDC Subjective Knee Form, range, 0–100) and knee pain (VAS, range, 0–100), general health (RAND-36, range, 0–100), progression of OA (KL classification, range, 0–4), activity level (Tegner Activity Scale, range, 0–10) followed up for 24 mon |
| Strength (n = 161, KL0: 10.1%, KL1: 49.7%, KL2, 3: 40.2%) |
RCT = randomized controlled trial, OA = osteoarthritis, MRI = magnetic resonance imaging, APM = arthroscopic partial meniscectomy, PT = physical therapy, KL = Kellgren-Lawrence, WOMAC = Western Ontario and McMaster University Osteoarthritis Index, KOOS = Knee injury and Osteoarthritis Outcome Score, TKR = total knee replacement, BML = bone marrow lesion, SF-36 = 36-Item Short Form Survey, IKDC = International Knee Documentation Committee.
APM plus PT versus PT
The METEOR trial81617 and Kirkley et al.'s trial14 compared the effects of APM plus PT and PT. The METEOR trial presented follow-up results from 6 months to 5 years after surgery, while Kirkley et al.14 presented the results up to 2 years of follow-up. Standardized APM surgery was performed in the intervention group, and PT was provided for rehabilitation after surgery.
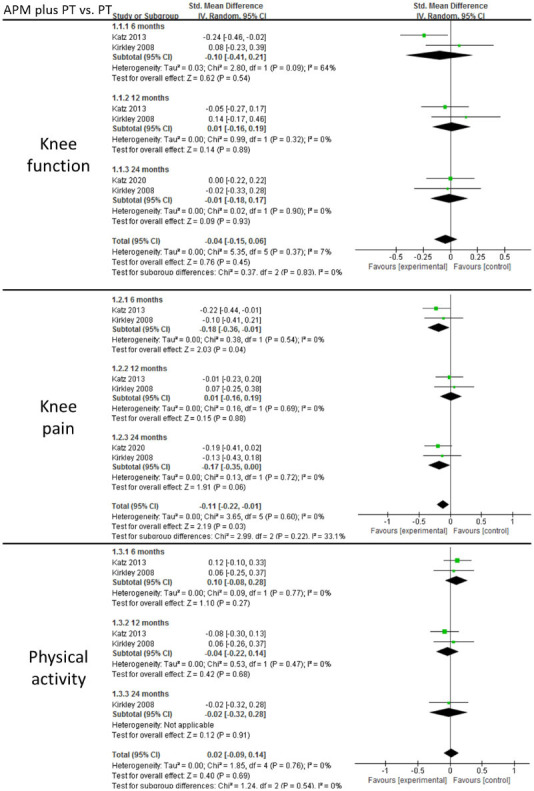
Knee function
Both trials presented the WOMAC physical function score, in which the higher the score, the more limited the function. METEOR trials used a scale of 0–100 points, while Kirkley et al.14 used a scale of 0–2,400 points. Because of such differences in scale, standardized mean scores were synthesized for the comparison period of 6-, 12-, and 24-month outcomes (Fig. 2). At 6 months, the scores in the intervention group were lower, mostly due to the METEOR result, but the difference did not reach statistical significance. At 12 and 24 months, no differences were found between the groups. The results of the follow-up from 2 to 5 years could only be confirmed in the Katz et al.'s study16; therefore, we did not perform a meta-analysis.

Knee pain
In the METEOR trial, the KOOS pain score was used, while in the study by Kirkley et al.,14 WOMAC pain score was used, in which the higher the score, the more severe the pain. Due to the differences in the measurement tools, the standardized mean scores were used for data synthesis to compare the 6-, 12-, and 24-month outcomes. At 6 months, the pain score of the APM group was significantly lower than that of the PT group (Fig. 3). There were no significant differences at 12 and 24 months.
Fig. 3
Knee pain following APM plus PT versus PT.
APM = arthroscopic partial meniscectomy, PT = physical therapy, SD = standard deviation, CI = confidence interval.
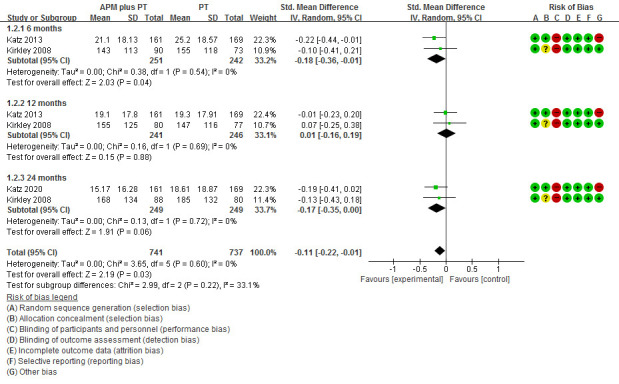
The results after 5 years could only be obtained in the Katz et al.'s study16; therefore, we did not perform a meta-analysis. The pain score continued to improve throughout the 24 months and then stabilized at 24–60 months in both groups.
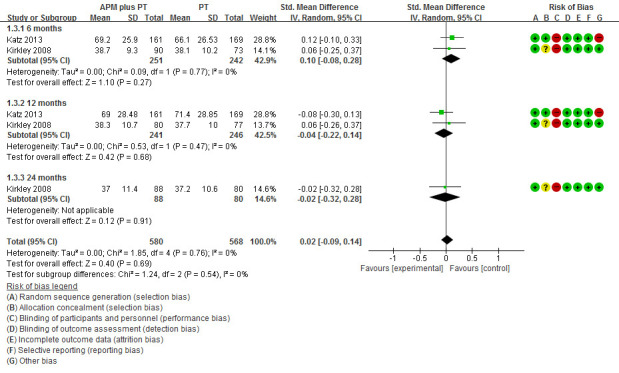
Physical activity
In both trials, the physical activity scale of 36-Item Short Form Survey (SF-36) was applied. Both reported results at 6 and 12 months, when there was no significant difference between the groups (Fig. 4).
TKR
Katz et al.16 showed that the intervention group had a greater frequency of TKR over 5 years. The hazard ratio for analysis as assigned (intention-to-treat) was 2.0 (95% CI, 0.8–4.9) and as a treated analysis, 4.9 (95% CI, 1.1–20.9). However, 30.2% of patients in the PT group crossed over to receive APM treatment during the 5-year observation period.
Other outcomes: effects of degree of intra-articular damage on pain improvement
MacFarlane et al.17 analyzed data from the METEOR trial post hoc and reported that those with the least and moderate damage (bone marrow lesions, cartilage, and meniscal damage) measured with MRI showed greater improvement in pain with APM than with PT, while those with the greatest damage had a similar improvement.
Adverse effects
There was no significant difference in the adverse effects between the groups, and serious adverse effects such as death occurred in three patients in the intervention group and two in the control group during the 12-month follow-up period. Mild and moderate adverse effects occurred in 15 and 13 patients in the intervention and control groups, respectively.
APM versus PT
Only ESCAPE trial15 compared the effects of APM surgery alone and PT alone in patients with meniscal tear without mechanical symptom. The change in patients-reported knee function measured using the International Knee Documentation Committee score (0–100 points, a score of 100 indicates no knee-related symptoms and no restrictions in daily life) was the primary outcome. At 24 months follow-up, knee function improved by 26.2 points in the intervention group and by 20.4 points in the control group, showing that PT was not inferior to APM. Knee pain measured using a VAS (0–100 points, a score of 0 indicating no pain and 100 indicating the most severe pain) was a secondary outcome. At 24 months follow-up, knee pain improved by 39.2 mm in the intervention group and by 32.5 mm in the control group, showing more favorable results for APM (between-group difference 5.9 mm (95% CI, 1.4–10.3; P = 0.01). The difference in other outcomes including activity level, general health and OA severity at 24 months was not statistically significant. Serious adverse events (e.g., cardiovascular, or repeat knee surgery) occurred in 9 participants in the intervention and 8 in the control group while non-serious adverse events including knee pain resulting in extra consultation occurred in 9 participants in the intervention and 4 in the control group.
DISCUSSION
In this study, using a modified update of an existing SR and a meta-analysis to assess the effectiveness of APM in patients with knee OA, we found that knee pain was significantly improved in the APM plus PT compared to the PT alone group or the APM alone compared to PT alone group at 6 months and over 24 months, respectively. There was no difference observed between the two groups in terms of knee function, physical activity, or knee pain at other time points.
RCTs comparing arthroscopic surgery with sham surgery or PT in patients with degenerative meniscal tears have been performed recently, raising concerns about the value of surgical treatment. Our study focused on patients with knee OA, which was in line with results from previous studies that showed largely weak evidence for arthroscopic surgery. Although pain at 6 months was significantly better in APM plus PT group compared to PT only group, the SMD was small (−0.19, 95% CI, −0.36–0.01), with questionable clinical significance. Comparison between APM alone and PT alone was only possible using a single RCT, which showed that pain improved more in the APM group. Again, the between-group difference of 5.9 mm using the 100 mm VAS scale was small and less than the minimum clinically important change for various pain conditions, including OA (range, −8–−40 mm; knee OA, −19.9 mm).1920 Favorable results on physical function measured with the WOMAC function scale at 6 months for APM plus PT in the METEOR trial was negated by Kirkley et al.'s trial,14 and the pooled difference was not statistically different between the two groups. Pain and function at 12 and 24 months were not different between the APM plus PT and PT groups, as well as physical activity measured with the SF-36. These results were also in the same direction in the RCT comparing APM only and PT only. MacFarlane et al.17 showed that patients with less structural damage had greater improvement in pain with APM than with PT, suggesting again that the efficacy of APM in advanced OA patients may be limited. Although APM is an invasive procedure, there was no significant difference in adverse effects between the study groups. A study using National Hospital Episode Statistics data in England reported a low risk associated with undergoing APM (serious complication rate of 0.317%) with increasing age and a high Charlson comorbidity index associated with an increased risk of serious complications.21 The risk-benefit of APM should be prudently determined, considering the rare but serious complications, including pulmonary embolism and infection associated with the procedure.
The rationale behind the lack of effect of APM in OA meniscal tears for symptom relief is manifold. Meniscal damage on MRI of the knee is common among middle-aged and elderly persons without knee symptoms and is not associated with pain severity in OA patients.45 A recent study collected data on the presence of patient-reported knee symptoms, including mechanical symptoms such as knee catching and locking in 565 consecutive patients and examined the association of specific pathological conditions of the knee observed during arthroscopic surgery with the presence of preoperative knee symptoms.22 Contrary to the belief that “meniscal” and “mechanical” symptoms arose from meniscal tears, the study revealed no significant association between the meniscal tear pattern and symptom score, nor any difference in grinding/clicking/popping, pain when pivoting, or catching/locking among those without, with a stable, or with an unstable meniscal tear.
The concern about the influence of meniscus resection or arthroscopy itself on cartilage damage is a lingering subject, with some supportive evidence. Previous studies suggested the protective function of the meniscus on cartilage, such that a statistically significant incidence of radiographic signs of OA is observed at 8 to 16 years of follow-up after knee APM compared with control non-operated knees.23 These results are especially worrisome for OA patients with meniscal tears whose cartilage is already compromised, and in whom the number of arthroscopic surgeries is substantial. Although the rate of knee arthroscopies in the aged population and in OA has been declining in Australia and the US, especially since the Medicare program stopped reimbursing physicians for arthroscopies performed for knee OA in 2004, whether such a decline occurs in OA patients with meniscus tears or elsewhere in the world is not known.624
This study had several limitations. Despite our efforts, we could obtain only three RCTs that met our eligibility criteria without overlapping patient populations. For these 3 trials, the proportion of definite OA patients was different, such that the METEOR and ESCAPE trials included 21.1 and 12% of patients, respectively, with KL-grade 0, while Kirkley et al.14 included none. The slight discrepancy in pain outcome between studies may stem from such a difference in the proportion of included OA patients, with the study including OA patients exclusively not showing improvement of pain by APM. Patients with knee locking were universally excluded; thus, the results does not apply to such patients. Although we observed a significant difference in pain at 6 months, which favored APM, it should be noted that the minimum clinically important change in pain scores for patients with meniscal tears is not defined. Our results are in line with the current trend of caution against the use of APM in patients with OA and a recent umbrella review of level 1 evidence for common elective orthopaedic procedures showing that small benefits of APM for degenerative meniscal tears is reported only for patients without OA.25 However, improvement at an earlier time point by APM may be interpreted differently depending on the patient preferences, which differs according to the health care system and culture. In some societies, lengthy recovery with PT may not be preferred by patients and pose problems with patient compliance.
In conclusion, our study showed that knee pain was significantly improved in the APM group compared to non-operative care group at 6 months and over 24 months. There was no difference observed between the two groups in terms of knee function, physical activity, or knee pain at other time points. Our result was based on only 3 RCTs revealing a significant knowledge gap, hence demanding more high-quality RCTs in OA patients.
 XML Download
XML Download