

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Stroke is a leading cause of mortality and major disability.12 Secondary prevention strategy for ischemic stroke includes strict control of vascular risk factors, an appropriate use of antiplatelet agents or anticoagulants according to the stroke mechanism.34567 Stroke guidelines support a short-term use of dual antiplatelet therapy (DAPT) up to 21–30 days after non-cardioembolic minor stroke to prevent recurrent ischemic events at 90 days.57 Long-term treatment of DAPT or triple antiplatelet therapy (TAPT) for secondary prevention were not recommended due to a lack of data demonstrating in a reduction in recurrent stroke events, while it did increase the risk of major bleeding.678910111213 In reality, 6–10% of stroke patients may experience recurrence of stroke within a year following the stroke in spite of best medical management.1415 Indeed, there is no clear guideline on the optimal antiplatelet strategy for secondary stroke prevention in ischemic stroke patients while on single antiplatelet therapy (SAPT) in real practice.3456716171819 Therefore, we aimed to evaluate the effect of different antiplatelet strategies including SAPT, DAPT or TAPT on stroke recurrence, composite vascular outcomes, and major bleeding after 1 year in patients with non-cardioembolic ischemic stroke who were already treated with SAPT.
METHODS
Study population
We performed this retrospective study using a large linked dataset (n = 52,213 ischemic stroke cases) from the Health Insurance Review and Assessment Service (HIRA) administrative claims database and the Clinical Research Center for Stroke (CRCS) registry in patients with acute stroke or transient ischemic attack (TIA) within 7 days of onset between January 2007 and December 2014, as described previously.20 The CRCS registry included clinical information during acute stroke managements after stroke. The HIRA contained information on the diagnoses, treatments, and prescribed medications in the claims data which were managed as the process of reimbursement under National Health Insurance program.20 In addition, there were long-term follow-up data (until December 2018) of included patients after ischemic stroke in the claims data of the linked dataset. The inclusion criteria were as follows: 1) acute ischemic stroke within 7 days from onset between January 2008 and December 2014; 2) non-cardioembolic origin according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification21; 3) no history of atrial fibrillation (AF); and 4) SAPT before index stroke because of primary or secondary prevention, and any other causes. We excluded patients who were admitted before January 2008 (n = 3,955), died during hospitalization after stroke (n = 774), cardioembolic stroke (n = 9,511), or met any of the following criteria: a history of AF in patients with non-cardioembolic ischemic stroke (n = 2,327), no antiplatelet therapy before ischemic stroke (n = 18,518), inaccurate claims data to evaluate the history of medications (n = 5,403), a history of myocardial infarction (MI), intracerebral hemorrhage (ICH), or gastrointestinal (GI) bleeding (n = 537), or were treated with multiple antiplatelet therapy before index stroke (n = 1,904) for an accurate analysis of new events following the index stroke using operational definition of claims data (Fig. 1). Finally, 9,284 patients were included in this study (Fig. 1).

Baseline characteristics and clinical information
Demographic information, such as age, sex, and clinical information, including vascular risk factors, was obtained from the linked data. Clinical data related to acute stroke managements, including pre-stroke functional status, reperfusion therapy, stroke mechanisms, and stroke severity at the initial examination and discharge, assessed using the National Institute of Health Stroke Scale (NIHSS), were collected from the CRCS registry data of the linked data. Ischemic stroke mechanisms were classified into four categories based on the TOAST classification: 1) large artery atherosclerosis (LAA); 2) small vessel occlusion (SVO); 3) other determined etiology; and 4) undetermined etiology.21 Additionally, we collected medication information, including GI protectants (proton pump inhibitors, histamine-2 receptor antagonists, bismuth, and sucralfate) and anticoagulants (low molecular weight heparin, warfarin, and direct oral anticoagulants), which were prescribed after discharge of stroke from the linked claims dataset in the HIRA. Moreover, we analyzed data of the patients with percutaneous coronary intervention (PCI) or with a newly diagnosed AF after discharge using claims data. Patients were divided into the following three groups according to antiplatelet therapy at discharge after acute ischemic stroke (antiplatelet agents: aspirin, clopidogrel, cilostazol, triflusal, dipyridamole, and ticlopidine): 1) SAPT group; 2) DAPT group; and 3) TAPT group. SAPT group continued the same antiplatelet agent or switched to a different antiplatelet agent, DAPT group were treated with dual antiplatelet agents, and TAPT were treated with triple antiplatelet agents at discharge after ischemic stroke. The medication and combination of antiplatelet agents were decided at the discretion of physicians.
Outcomes
The primary outcomes were composite outcomes including vascular events (ischemic stroke, ICH, and MI), all-cause mortality, and ischemic stroke during the 1-year follow-up period after stroke.222324 Secondary outcomes were the occurrence of MI or death. Safety outcomes were major bleeding events such as ICH or GI bleeding during the 1-year period following the stroke.222324 Composite outcome was identified the first outcome event among total outcomes including ischemic stroke, ICH, acute myocardial infarction and all-cause mortality. In addition, other outcomes were identified as an independent outcome event for 1 year. The detailed outcome definitions are described in Supplementary Table 1. Predefined subgroup analyses were planned to assess the differential primary and safety outcomes according to stroke severity (minor stroke, NIHSS score 0–3; moderate-to-severe stroke, NIHSS score ≥ 4)2526 and stroke subtypes (LAA and SVO).
Statistical analysis
Baseline characteristics and clinical information are presented using frequency (%) for categorical variables, and continuous variables are presented as mean ± standard deviation or median (interquartile range) according to whether normal distributions or not. In categorical variables, they were analyzed based on Pearson’s χ2 test or Fisher’s exact test, as appropriate. Continuous variables were appropriately analyzed using the Kruskal-Wallis test or one-way analysis of variance. Moreover, the effect of variables including antiplatelet therapy on hazard ratios (HRs) with 95% confidence intervals (CIs) on outcomes were analyzed using the Cox proportional regression model based on the multivariable analysis. Additionally, Cox regression was conducted based on the Firth’s penalized maximum likelihood bias reduction method to estimate outcome events and to solve problem in case of monotone likelihood such as non-convergence of likelihood function.2728 Outcome analyses were performed based on time-to-discharge medications after ischemic stroke. A P value < 0.05 in univariate analysis was considered significant differences and those statistically significant variables and clinically important factors were adjusted for multivariable analysis. The cumulative incidence of outcomes over time was estimated and plotted using Kaplan-Meier analysis. Incidence rates per 1,000 person-years of outcomes were calculated for the three groups based on the log-transformed normal approximation. Statistical analyses were performed using SAS statistical software by professional medical statisticians Lee JS and Yoon JS (Release 9.4; SAS Institute Inc., Cary, NC, USA).
RESULTS
Baseline characteristics of the study patients
From January 2008 to December 2014, a total of 9,284 patients were included in the analysis (Fig. 1). Demographic and clinical baseline characteristics are shown in Table 1. The antiplatelet therapy strategies were 1) SAPT (n = 5,565, 59.9%); 2) DAPT (n = 3,638, 39.2%); and 3) TAPT (n = 81, 0.9%). The mean age of the patients was 68.2 years, and 58.2% were male. The SAPT group was younger, had less male preponderance, and had a lower proportion of vascular risk factors, including hypertension, diabetes mellitus (DM), and a previous history of stroke or TIA. In SAPT group, 64.9% (n = 3,554) patients changed to different antiplatelet agents. Clinical characteristics of the SAPT group based on the information of changing or maintaining the antiplatelet agent were presented in Supplementary Table 2. Changing group was significantly older and more likely to have hypertension, DM, and LAA mechanism than maintaining group. In addition, the proportion of patients with a baseline modified Rankin Scale (mRS) of 0 was significantly lower in the TAPT group than in the SAPT and DAPT groups (58.0% vs. 71.6% and 72.9%, respectively; P = 0.008). Regarding stroke mechanisms, LAA was more prevalent in the DAPT and TAPT groups than in the SAPT group (55.8% and 54.3% vs. 39.7%, respectively, P < 0.001) in Table 1. The patterns of acute reperfusion therapy did not differ among the three groups. However, the median initial and discharge NIHSS scores were significantly higher in the TAPT group than in the SAPT and DAPT groups (P < 0.001) (Table 1). TAPT was more likely to be treated with GI protectants after stroke. The proportion of newly diagnosed of AF and undergoing PCI after stroke was not significantly different in three groups (Table 1).
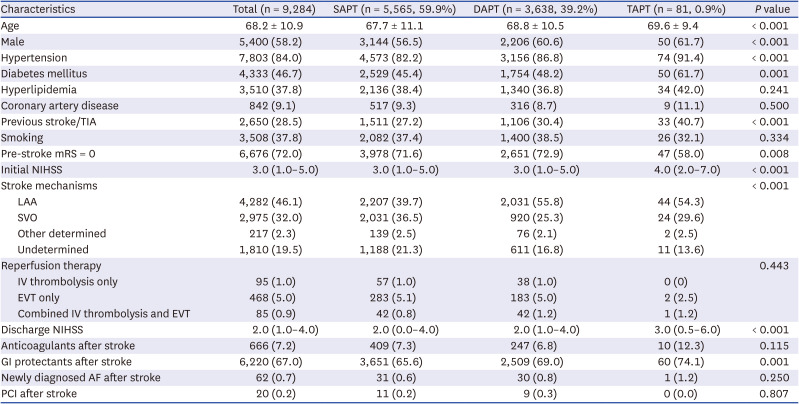
Table 1
Baseline characteristics of the included patients
Values are presented as mean ± standard deviation, number (%), or median (interquartile range).
SAPT = single antiplatelet therapy, DAPT = dual antiplatelet therapy, TAPT = triple antiplatelet therapy, TIA = transient ischemic attack, mRS = modified Rankin Scale, NIHSS = National Institute of Health Stroke Scale, LAA = large artery atherosclerosis, SVO = small vessel occlusion, IV = intravenous, EVT = endovascular therapy, GI = gastrointestinal, AF = atrial fibrillation, PCI = percutaneous coronary intervention.
![]()
Impact of antiplatelet therapy on the outcomes
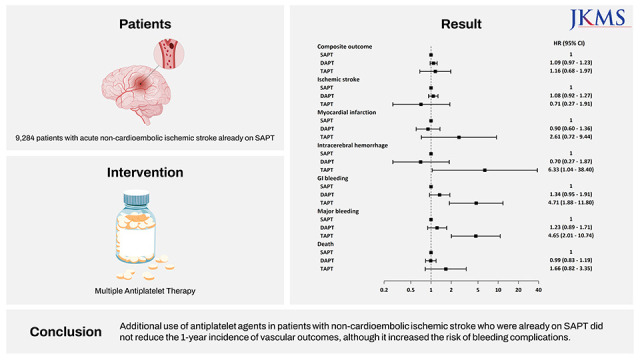
The composite outcome as the primary outcome occurred in 1,152 (12.4%). In Kaplan-Meier curves, more composite outcome events occurred in the DAPT and TAPT groups than in the SAPT group (13.47, 17.28 vs. 11.64 rates per 1,000 person-years, respectively, P = 0.014) (Fig. 2A, Table 2). In the adjusted analysis, DAPT and TAPT did not reduce the risk of composite outcomes (DAPT, HR, 1.09, 95% CI, 0.97–1.23, P = 0.152; TAPT, HR, 1.16, 95% CI, 0.68–1.97, P = 0.592). Ischemic stroke recurrence tended to be more common in the DAPT group than in the SAPT group, but the difference was not statistically significant (log-rank test, P = 0.08) (Fig. 2B). The multivariable analysis also showed that ischemic stroke recurrence at 1 year did not differ in three groups (Table 2, Fig. 2). Moreover, MI rate did not differ among the three subgroups (Fig. 2C, Table 2, P = 0.421). Multiple antiplatelet therapies (DAPT and TAPT) were associated with an increased risk of GI bleeding (P < 0.001 by log-rank test) and major bleeding events (P < 0.001 by log-rank test) (Table 2. Fig. 2). In particular, TAPT was associated with a 5-fold increased risk of bleeding events (GI bleeding and major bleeding) and a 6-fold increased risk of ICH in the adjusted analysis (Table 2, Fig. 3). Regarding the types and combinations of antiplatelet agents, there was no significant relationship between the types of antiplatelet agents and outcomes in SAPT group (Supplementary Table 3), and impact on outcomes according to combinations of antiplatelet agents in DAPT and TAPT groups (Supplementary Tables 4 and 5).
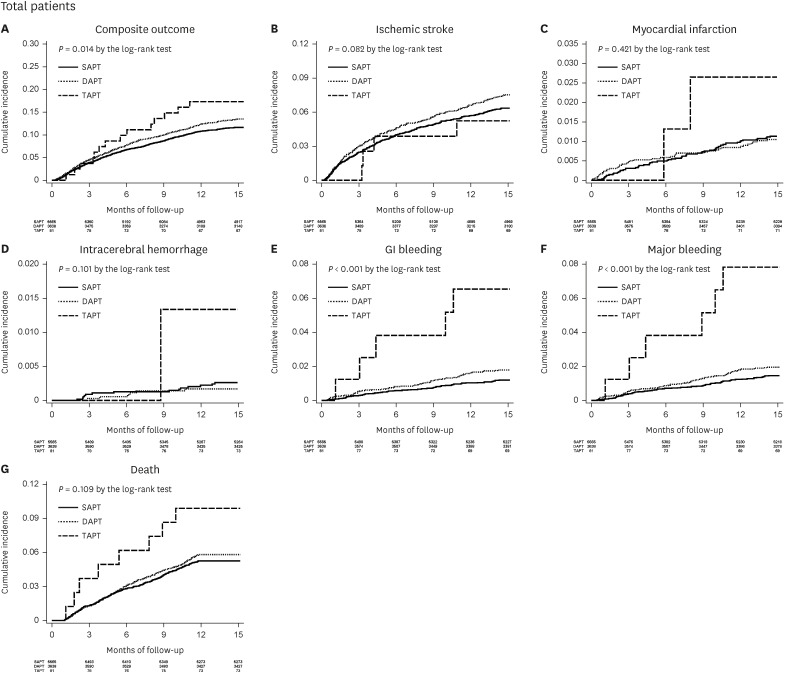
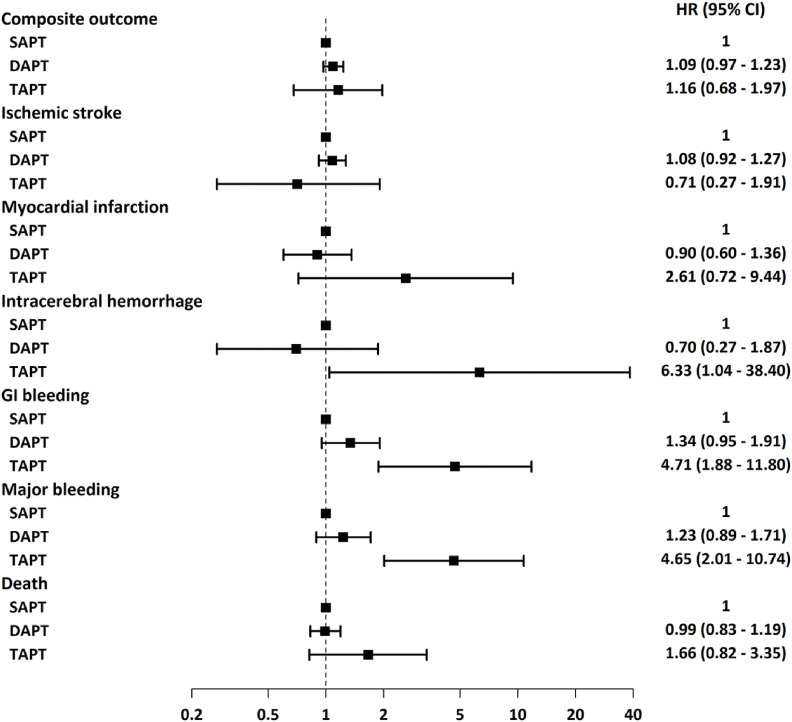

Fig. 2
Kaplan-Meier analysis of primary outcome and secondary outcome in the total patients. (A) Cumulative incidence of the composite outcome. (B) Cumulative incidence of the ischemic stroke. (C) Cumulative incidence of the myocardial infarction. (D) Cumulative incidence of the intracerebral hemorrhage. (E) Cumulative incidence of GI bleeding. (F) Cumulative incidence of major bleeding. (G) Cumulative incidence of all-cause death.
GI = gastrointestinal, SAPT = single antiplatelet therapy, DAPT = dual antiplatelet therapy, TAPT = triple antiplatelet therapy.
![]()
Fig. 3
HR for primary outcome and secondary outcome in the total patients. DAPT and TAPT did not reduce the 1-year incidence of composite outcome, recurrent stroke, myocardial infarction, and all-cause death. Instead, DAPT and TAPT were associated with a higher rate of bleeding events than maintaining SAPT in patients with acute non-cardioembolic ischemic stroke who were already on SAPT.
SAPT = single antiplatelet therapy, DAPT = dual antiplatelet therapy, TAPT = triple antiplatelet therapy, GI = gastrointestinal, HR = hazard ratio, CI = confidence interval.
![]()
Table 2
Primary and secondary outcomes according to antiplatelet therapy in total included patients
Composite outcome: adjusted for age, sex, hypertension, DM, previous stroke/TIA, pre-stroke mRS, initial NIHSS, stroke mechanism, thrombolytic therapy, anticoagulants, antiplatelet agents. Ischemic stroke, myocardial infarction, all-cause of death: adjusted for age, sex, hypertension, DM, previous stroke/TIA, pre-stroke mRS, initial NIHSS, stroke mechanism, thrombolytic therapy, antiplatelet agents. ICH: adjusted for age, sex, hypertension, DM, previous stroke/TIA, pre-stroke mRS, initial NIHSS, stroke mechanism, thrombolytic therapy, anticoagulants, antiplatelet agents. GI bleeding: adjusted for age, sex, hypertension, DM, previous stroke/TIA, pre-stroke mRS, initial NIHSS, stroke mechanism, thrombolytic therapy, anticoagulants, GI protectants, antiplatelet agents. Major bleeding: adjusted for age, sex, hypertension, DM, previous stroke/TIA, pre-stroke mRS, initial NIHSS, stroke mechanism, thrombolytic therapy, anticoagulants, GI protectants, antiplatelet agents.
HR = hazard ratio, CI = confidence interval, SAPT = single antiplatelet therapy, DAPT = dual antiplatelet therapy, TAPT = triple antiplatelet therapy, ICH = intracerebral hemorrhage, GI = gastrointestinal, DM = diabetes mellitus, TIA = transient ischemic attack, mRS = modified Rankin Scale, NIHSS = National Institute of Health Stroke Scale.
![]()
Subgroup analyses
Stroke severity (NIHSS 0–3 and NIHSS ≥ 4)
The baseline characteristics of the patients were stratified according to stroke severity (minor stroke [NIHSS score 0–3] and moderate-to-severe stroke [NIHSS score ≥ 4]) (Supplementary Tables 6 and 7). Among the minor stroke, 61.9% were treated with SAPT. The SAPT group was younger, was less likely to have stroke risk factors, and predominantly had SVO mechanism. The initial NIHSS score was significantly higher in the TAPT group, and the proportion of patients receiving GI protectants was also higher in the TAPT group (Supplementary Table 6). Patients with moderate-to-severe stroke were mostly treated with SAPT (57.1%), followed by DAPT (41.8%), which was higher than the minor stroke group (37.3%) (Supplementary Tables 6 and 7). As observed in patients with minor stroke, the TAPT group was more likely to have vascular risk factors with concomitant administration of anticoagulants (14.6%) than the other groups (SAPT, 8.9% and DAPT, 6.9%, respectively). Additionally, LAA was the most common stroke mechanism in the DAPT and TAPT groups (Supplementary Table 7). In outcomes analysis of patients with minor stroke, multiple antiplatelet strategies did not reduce the risk of composite outcomes or ischemic stroke. However, major bleeding events tended to be higher in the DAPT (HR, 1.21, 95% CI, 0.75–1.98) and TAPT groups (HR, 2.84, 95% CI, 0.53–15.21) than in the SAPT group (Supplementary Table 8, Supplementary Fig. 1). In the moderate or severe stroke group, DAPT and TAPT did not reduce vascular outcomes, and TAPT caused a 6.7-fold increase in the risk of major bleeding (HR, 6.69, 95% CI, 2.59–17.25, P < 0.001 in Supplementary Table 8, Supplementary Fig. 2).
Stroke mechanisms (LAA and SVO)
In the LAA group (n = 4,282), the proportion of patients with hypertension and coronary artery disease was significantly greater in the TAPT group than that in the other groups. A lower percentage of TAPT patients (56.8%) were independent before the index stroke (pre-stroke mRS = 0). Additionally, TAPT patients were more likely to be treated with concomitant anticoagulants and GI protectants during the 1-year follow-up period (Supplementary Table 9). Regarding outcomes, DAPT and TAPT did not reduce the incidence of recurrent ischemic stroke or composite outcomes. However, TAPT significantly increased the risk of major bleeding (HR, 3.94, 95% CI, 1.19–12.94, P = 0.024) than SAPT (Supplementary Table 10, Supplementary Figs. 3 and 4). In SVO group, the DAPT and TAPT groups were older and more likely to have hypertension, DM, history of stroke/TIA, and higher initial NIHSS scores than the SAPT group. Moreover, prescriptions of anticoagulants and GI protectants were also most common in the TAPT group (Supplementary Table 11). In multivariable analyses, the risk of composite outcomes was significantly higher in TAPT group, but the risk of ischemic stroke or major bleeding were not different among three treatment groups (Supplementary Table 10, Supplementary Figs. 3 and 4).
DISCUSSION
This study demonstrated that the use of multiple antiplatelet agents in patients with ischemic stroke while on SAPT did not reduce the composite vascular outcomes, recurrent stroke, MI, or all-cause mortality over 1-year of follow-up in non-cardioembolic ischemic stroke. Moreover, DAPT and TAPT increased the risk of bleeding complications compared with SAPT. If stratified by stroke severity and stroke mechanisms, no benefit was noted in the prevention of stroke recurrence and composite outcomes. In addition, TAPT increased the risk of major bleeding complications in ischemic stroke patients over 1-year.
A combination of different antiplatelet therapy mechanisms may provide synergistic effects on reducing the recurrence of ischemic events by rapid inhibition of platelet activity in thrombus propagation.4 In line with this, several clinical trials have demonstrated that a short-term (21–90 days) combination of aspirin and clopidogrel or ticagrelor (DAPT) significantly reduced the recurrence of stroke and cardiovascular events, despite an increase in bleeding events.25262930 However, intensive TAPT did not reduce the incidence of recurrent stroke, but did increase the risk of major bleeding at 90 days.78 Therefore, current guidelines recommend the administration of short-term DAPT in the acute phase of minor ischemic stroke.4531 In clinical practice, a significant portion of patients with acute ischemic stroke present with moderate or severe stroke (NIHSS > 4), and those DAPT trials have limited generalizability.252629303132 However, there is a lack of knowledge regarding the optimal antiplatelet regimen for patients after ischemic stroke who have been taking aspirin or other single antiplatelet agents based on the severity and mechanism of stroke.456781213 In Platelet-Oriented Inhibition in New TIA and Minor Ischemic Stroke (POINT) trial, about 60% of the participants already used SAPT (aspirin in 58% and clopidogrel in 2%) at presentation. However, there was no analysis of the data comparing treatment outcomes based on the medication use at presentation. Moreover, no results were presented regarding the effects of DAPT or SAPT regimen on outcome according to previous antiplatelet agent therapy.25
In this study, neither DAPT nor TAPT reduced the recurrence of ischemic stroke and composite outcomes at 1 year compared with continuing SAPT in patients already on SAPT before stroke. Multiple antiplatelet treatments were associated with an increase in bleeding events compared to continuing SAPT. In particular, TAPT significantly increased the risk of major bleeding, consistent with the results of previous studies.678910111213 Patients with DAPT or TAPT were more likely to have vascular risk factors and were more likely to have concomitant anticoagulants during the follow-up period. These factors could have affected bleeding outcomes. However, we adjusted for these confounding factors, and the results remained statistically significant.
A long-term follow-up study of the Clopidogrel in High-Risk Patients with Acute Nondisabling Cerebrovascular Events (CHANCE) trial showed that a beneficial effect of DAPT persisted up to 1 year in patients with minor stroke and TIA.3334 In our study, we compared the effect of DAPT or TAPT with that of SAPT on 1-year outcomes stratified by the stroke severity. In patients with minor stroke (NIHSS score 0–3), no difference was observed in efficacy or safety, including the bleeding risk between the groups, which is not in line with previous results.131931323334353637 Furthermore, multiple antiplatelet agents significantly increased the risk of major bleeding without any benefit for secondary prevention in patients with moderate-to-severe stroke (NIHSS score ≥ 4). Therefore, DAPT and TAPT did not reduce the 1-year risk of stroke recurrence regardless of stroke severity and increased the risk of major bleeding in patients with moderate-to-severe stroke, especially with TAPT.
Antiplatelet therapy strategies can be modified based on stroke mechanisms. Recurrent ischemic stroke occurs more frequently during the early stages of acute ischemic stroke in patients with LAA subtype. In a subgroup analysis from the CHANCE trial, DAPT tended to be more effective in patients with intracranial artery stenosis (ICAS).38 In addition, a subgroup from the Acute Stroke or Transient Ischemic Attack Treated with Ticagrelor and ASA for Prevention of Stroke and Death (THALES) patients with ICAS ≥ 30% stenosis had less recurrence with DAPT compared to that with aspirin alone.39 There was no clinical data on the association between multiple antiplatelet agents and 1-year outcomes in LAA stroke patients treated with SAPT before stroke. In our study, DAPT and TAPT did not reduce the risk of composite outcomes and recurrent ischemic stroke but did increase the incidence of major bleeding in the multiple antiplatelet therapy groups in the LAA group. In the SVO group, TAPT significantly increased the 1-year incidence of composite outcomes compared to SAPT and no benefit was noted in the multiple antiplatelet therapy in preventing recurrent ischemic stroke, which is consistent with a previous study.11 Overall, DAPT and TAPT were not more effective than continuing SAPT in reducing vascular events. Furthermore, this study found an increased risk for major bleeding events, especially in TAPT group, suggesting that TAPT should not be used or recommended.
This study had several limitations. First, the claims data of linked dataset did not contain laboratory and clinical information related to the outcomes during the follow-up period. We were unable to rule out the potential effect of unmeasured confounding variables on the results despite the adjustment for several variables related to outcomes. Second, we analyzed the results using a discharge antiplatelet regimen. Patients might have discontinued the initial agents or switched to other medications based on clinical events, physicians’ personal experience, and concerns regarding risk factors during the 1-year follow-up period. However, we could not evaluate this because the linked dataset did not have the information on that. Therefore, these could be limitations in a study using linked data set. Therefore, these factors could be unmeasured based on linked data. Third, there was no clinical information on the reason for changes in the antiplatelet regimen using the linked dataset. Therefore, those factors could have affected the results. Fourth, underwent PCI or developed new AF after discharge. These might have an effect on the treatment strategy and the vascular outcome. Fifth, the effect of different antiplatelet agents and combinations were not significantly different in our study. However, the analysis of the differential effect of multiple antiplatelet agent combinations could be limited because the numbers of patients in each combination were varied. This may have limited the interpretation of the results. Sixth, this study was conducted using data from Korean stroke patients; therefore, the results need to be interpreted in caution in different ethnic groups. Seventh, we did not randomly assign the patients to different antiplatelet therapy groups because this was a retrospective study based on linked data set using registry and insurance claims data. Despite we used multivariable analysis to control confounding factors such as age, stroke severity, stroke mechanisms and vascular risk factors, there was still a possibility of unmeasured bias.
In conclusion, this study demonstrated that a risk of 1-year recurrent stroke, vascular events, and death were not significantly different among patients with ischemic stroke receiving DAPT or TAPT compared with those receiving continued SAPT, regardless of stroke severity or stroke mechanisms using linked stroke data. Moreover, multiple antiplatelet agents, especially TAPT, were associated with a risk of major bleeding at 1-year after non-cardioembolic stroke while already on SAPT. Further large-scale prospective randomized controlled studies should be conducted to confirm the true relationship between long-term antiplatelet therapy and the 1-year outcomes after acute ischemic stroke.
 XML Download
XML Download