

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the outbreak of the coronavirus disease 2019 (COVID-19) pandemic, several variants of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have emerged. Among these variants, omicron (B.1.1.529) was first identified in November 2021 and had been subsequently declared as a variant of concern (VOC) by the World Health Organization (WHO).1 In South Korea, the first patient carrying the omicron variant was identified on December 1st, 2021,2 initiating a wide spread of the omicron variant (January 30, 2022 to April 24, 2022),3 which followed the preceding delta epidemic (July 7, 2021 to January 29, 2021).
Early national and international reports suggested that the clinical course of patients infected with the omicron variant was better than that of patients infected with the delta variant or variants of the other epidemics4; however, there were also reports suggesting the contrary.567 The SARS-CoV-2 omicron epidemic in South Korea was massive compared to that in other countries possibly owing to immune evasion8 or the previous epidemics,9 and there were reports of many severe patients.
Patients with severe COVID-19 infections require respiratory support, such as a high-flow nasal cannula (HFNC) or mechanical ventilation (MV),10 and the case fatality rate (CFR) in those patients varies depending on the size and speed of the outbreak. In a previous study, age > 65 years and underlying diseases were found to be risk factors for severe COVID-19 infection and death.10111213 Studies on young patients, although relatively limited,141516 reported that not only underlying diseases but also obesity15 and non-vaccination171819 had emerged as risk factors of complications in this particular population. A study conducted in South Korea during the fourth epidemic after the delta variant20 showed that for critical COVID-19 patients aged ≤ 50 years,21 age, elevated creatinine (Cr), decreased platelet, MV, continuous renal replacement therapy (CRRT), central line-associated bloodstream infection (CLABSI), obesity, and lack of vaccination were risk factors for mortality.
It was suggested that in South Korea, there might be specific differences between the omicron variant epidemic (fifth epidemic) and the previous epidemics with respect to the characteristics and severity of the variant driving the epidemic, epidemic magnitude and spread, and vaccination completion rate at that period. Therefore, this study aimed to analyze the clinical characteristics and risk factors of death in young critical COVID-19 patients in South Korea during the omicron epidemic in comparison to those of patients older than 50 years and to also comparing this period to the delta variant period based on previous data.
METHODS
Study population and data sources
This study enrolled all critical patients hospitalized for COVID-19 in nine hospitals in South Korea between February 1, 2022 and April 30, 2022. The inclusion criterion was age ≥ 19 years, and the exclusion criteria were pediatric cases, re-confirmed cases, and cases confirmed after death. Each patient aged ≤ 50 years was matched to two patients aged > 50 years based on the diagnosis date. Matching in the control group consisted of the nearest date of diagnosis. If there were multiple control groups on the same diagnosis date, one oldest and one lowest age was selected for the correction of age variables. These patients were then evaluated and compared with respect to their clinical characteristics and prognosis.
All patients were diagnosed with COVID-19 using SARS-CoV-2 real-time reverse transcription polymerase chain reaction performed using nasopharyngeal swabs or sputum specimens or by expert rapid antigen testing according to national guidelines. Electronic medical records were reviewed to collect demographic characteristics, including BMI; underlying diseases; clinical features and laboratory findings on the day of admission; clinical course; treatment received; and outcomes. The Health Insurance Review and Assessment system was used to identify information about the status of vaccination, route of infection, living environment before hospitalization, and variant contracted. The patients were followed until death or discharge, whichever occurred first.
Study outcomes and definitions
Critically ill patients were defined as those who received HFNC or higher respiratory support during hospitalization, as defined by the Korea Disease Control and Prevention Agency (KDCA).22 The completion of vaccination was defined as completion of the second dose of Janssen or the third dose of Moderna/Pfizer/AstraZeneca taking into consideration the timing of the investigation. Breakthrough infection was defined as infection 2 weeks after completion of vaccination or 14–90 days after the second dose of the vaccine. The outcome measures were all-cause hospital mortality and MV or extracorporeal membrane oxygenation (ECMO). The severity of the clinical course was assessed based on the highest respiratory support required during the hospitalization period. These were classified as HFNC, MV, and ECMO. Since the study population comprised critically ill patients, patients maintained on nasal cannula or on room air were not included. Non-invasive positive pressure ventilation was not performed for the patients in this study. The outbreak was defined as the simultaneous occurrence of multiple confirmed cases in a nursing home/long-term care hospital, workplace, or religious or group facility. Hospital-acquired infection (HAI) was defined as confirmed cases during admission to acute care hospitals or long-term care facilities for other unrelated illnesses, except for outbreaks.
Statistical analysis
Continuous variables were expressed as the mean ± standard deviation (SD), while categorical variables were expressed as the frequency and percentage. Continuous variables were compared using the Student’s t-test or Mann-Whitney U test, as appropriate, while categorical variables were compared using the χ2 test or Fisher’s exact test. The all-cause mortality rate was compared between the two groups using Kaplan-Meier curves. Significant variables (P < 0.050) were analyzed using multivariate analysis (logistic regression model), and significant results were presented as the odds ratio (OR) and 95% confidence interval (CI). A logistic regression model was used to control for confounding variables. Statistically significant variables in the univariate analyses were then used in the multivariate analysis in addition to the variables of clinical significance. We performed a collinearity analysis on the results that were significant in the univariate analysis. A multivariate analysis was performed on the test results that emerged as independent variables in the collinearity analysis. A collinearity test was also performed to exclude the possibility of cross-influences. Risks factors for mortality were reported with their ORs and 95% CIs. When the median and interquartile ranges (IQRs) were reported, the median was assumed to reflect the mean and the IQR was assumed to be 1.35 SD. All P-values were reported to three decimal places. P values of < 0.050 were considered statistically significant. All statistical analyses were performed using IBM SPSS for Windows version 24.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Gil Medical Center (approval No. GCIRB2021-462). This study adhered to the principles embodied in the Declaration of Helsinki. The requirement for written informed consent was waived because de-identified data were collected retrospectively.
RESULTS
Comparison of clinical characteristics between age groups
A total of 213 patients were evaluated. Among them, 71 patients were aged ≤ 50 years, while 142 patients were aged > 50 years (110 of 142 were aged 65 years or older) (Table 1). The mean patient age was 62.44 ± 19.10 years. The patients aged ≤ 50 years had a mean ± SD age of 39.51 ± 8.92 years, while patients aged > 50 years had a mean ± SD age of 73.91 ± 10.56 years. Women accounted for 49.3% in the group of patients aged ≤ 50 years and for 42.3% of patients aged > 50 years, corresponding to nearly half in each group. Patients aged ≤ 50 years had fewer outbreak-related associations than those aged > 50 years (2.8% vs. 14.8%), but the difference was not significant (Table 1). Of the entire population, only 31.0% were fully vaccinated, and only 15 of 71 patients aged ≤ 50 years had complete vaccination, significantly lower than the complete vaccination rate in patients aged > 50 years (21.1% vs. 35.9%, P = 0.019).Compared with death group (29.3%), survivor group have a higher vaccine completion rate(34.8%), but no stastically significant.(Table 2).
Table 1
Patient characteristics
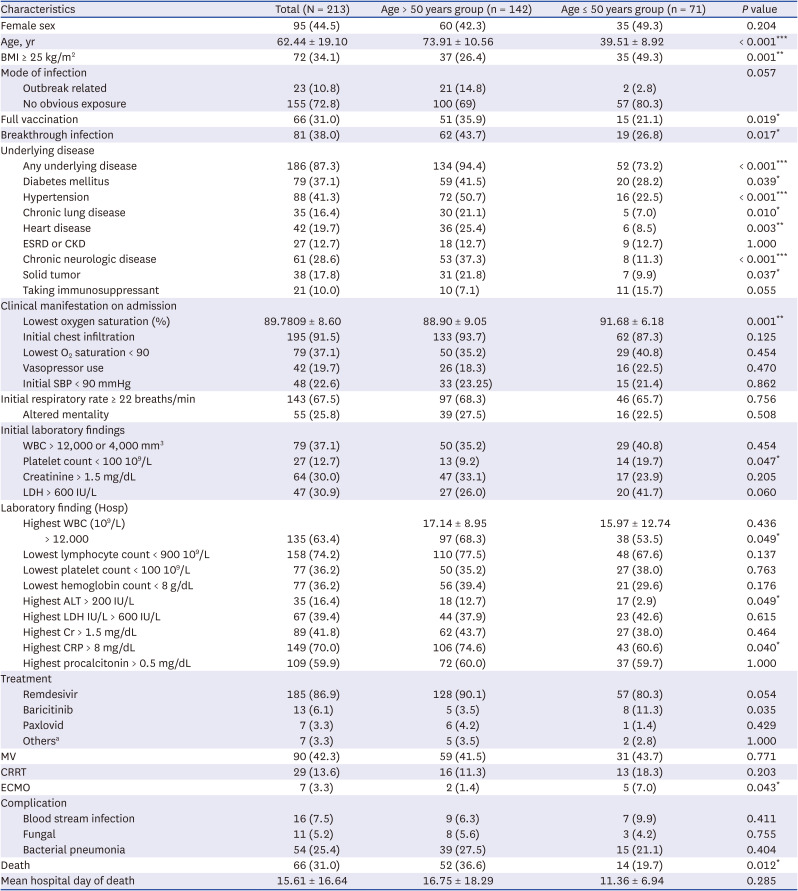
Values are presented as mean ± standard deviation or number (%).
BMI= body mass index, ESRD = end-stage renal disease, CKD = chronic kidney disease, O2 = oxygen, SBP = systolic blood pressure, WBC = white blood cell, ALT = alanine aminotransferase, LDH = lactate dehydrogenase, Cr = creatinine, CRP = C-reactive protein, MV= mechanical ventilation, CRRT = continuous renal replacement therapy, ECMO = extracorporeal membrane oxygenation.
aOther treatments: antibiotics, prone position, immunoglobulins, etc.
*P < 0.05, **P < 0.01, ***P < 0.001.
Table 2
Predictors of mortality
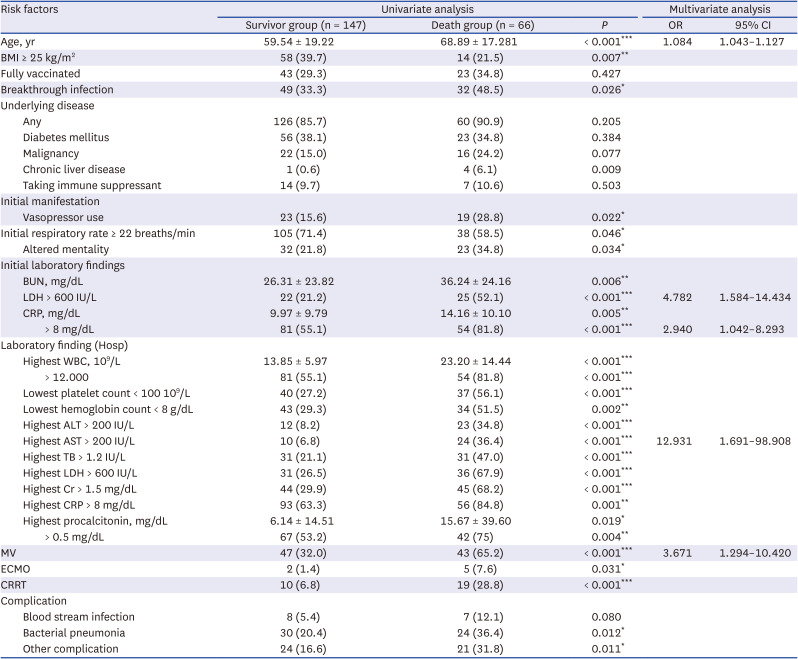
Values are presented as mean ± standard deviation or number (%).
OR = odds ratio, CI = confidential interval, BMI= body mass index, BUN= blood urea nitrogen, LDH = lactate dehydrogenase, CRP = C=reactive protein, WBC = white blood cell, ALT = alanine aminotransferase, AST = aspartate aminotransferase, TB = total bilirubin, Cr = creatinine, CRP = C-reactive protein, MV= mechanical ventilation, ECMO = extracorporeal membrane oxygenation, CRRT = continuous renal replacement therapy.
*P < 0.05, **P < 0.01, ***P < 0.001.
The ≤ 50 years group included a significantly higher percentage of patients with a BMI > 25 kg/m2 than did the > 50 years group (49.3% vs. 26.4%, P < 0.001) (Table 1); however, overall, there were fewer patients with a BMI of ≥ 25 kg/m2 during this omicron epidemic period than that during the delta epidemic period (Supplementary Table 1). The number of patients aged ≤ 50 years and had underlying diseases was also significantly lesser in the omicron epidemic period than in the delta epidemic period (73.2% vs. 94.4%, P < 0.001) (Table 1), but the number of underlying diseases in the patient was nearly three times higher than that in the delta epidemic period (Supplementary Table 1). Only 6 (8.4%) of the 71 critical patients aged ≤ 50 years had no risk factors (BMI ≥ 25 kg/m2 or underlying diseases). The most frequent underlying diseases in those aged ≤ 50 years were diabetes mellitus (28.2%) and hypertension (22.5%) followed by immunosuppression (15.7%).
Patients aged ≤ 50 years had higher oxygen saturation (91.68 ± 6.18 vs. 88.90 ± 9.05, P = 0.001) and had more frequent thrombocytopenia (19.7% vs. 9.2%, P = 0.047) than those aged >50 years. There was no significant difference between the two groups in the usage of MV and CRRT during the treatment course. However, ECMO was used significantly more in patients aged ≤ 50 years, which was attributed to the reduced usage of futile ECMO in elderly patients (7% vs. 1.4%; P = 0.043). The mean time to death in patients aged ≤ 50 years was 11.36 ± 6.94 days, shorter than that in patients aged > 50 years (16.75 ± 18.29 days) (Table 3).
Table 3
Risk factors for mortality in the young (age < 50 years) critical patients (N = 71)
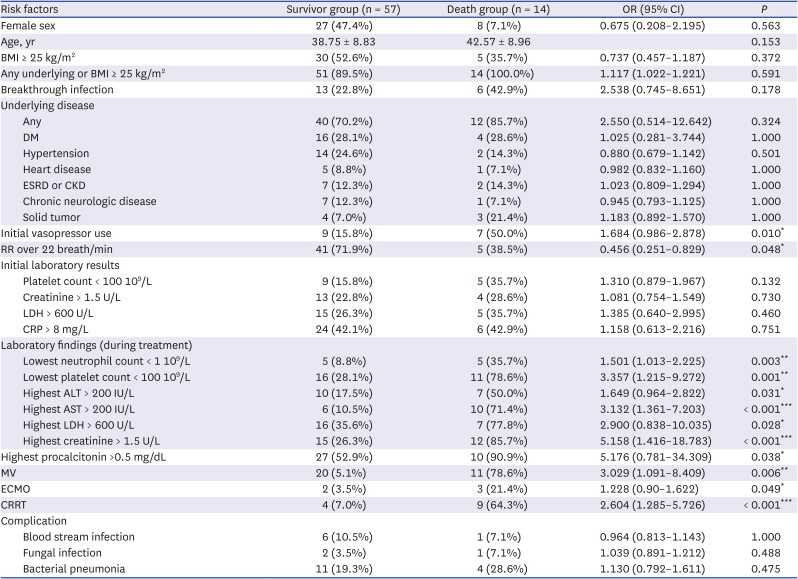
OR = odds ratio, CI = confidential interval, BMI = body mass index, DM = diabetes mellitus, ESRD = end-stage renal disease, CKD = chronic kidney disease, RR = respiratory rate, LDH = lactate dehydrogenase, CRP = C=reactive protein, ALT = alanine aminotransferase, AST = aspartate aminotransferase, LDH = lactate dehydrogenase, MV= mechanical ventilation, ECMO = extracorporeal membrane oxygenation, CRRT = continuous renal replacement therapy.
*P < 0.05, **P < 0.01, ***P < 0.001.
Risk factors for mortality in the whole population
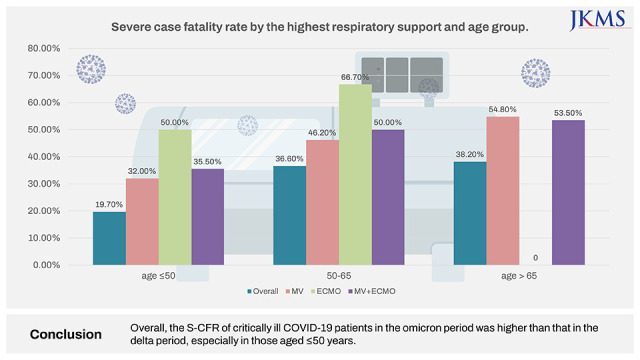
The total case fatality rate among severe patients (S-CFR) was 31.0%, higher than the 21.0% in the delta period (Supplementary Table 1). The fatality rate increased with age, from 19.7% in those aged ≤ 50 years to 36.6% in those aged > 50 years and 38.2% in those aged ≥ 65 years. Particularly, the mortality rate in patients aged ≤ 50 years was higher during the omicron epidemic than during the delta epidemic (Fig. 1, Supplementary Table 1). With respect to the survival rate by age, the mortality rate significantly increased as the age increased in the groups aged 50 years or younger (19.7%), 50–65 years (36.6%), and 65 years or older (38.2%) (P = 0.032) (Fig. 1). In MV patients, the mortality rate in those aged ≤ 50 years was 32%, lower than the mortality rate in those aged ≥ 65 years (46.2%). In ECMO patients, the mortality rate of those aged ≤ 50 years was close to 50% (Fig. 1).
Fig. 1
Severe case fatality rate by the highest respiratory support and age group.
MV = mechanical ventilation, ECMO = extracorporeal membrane oxygenation.
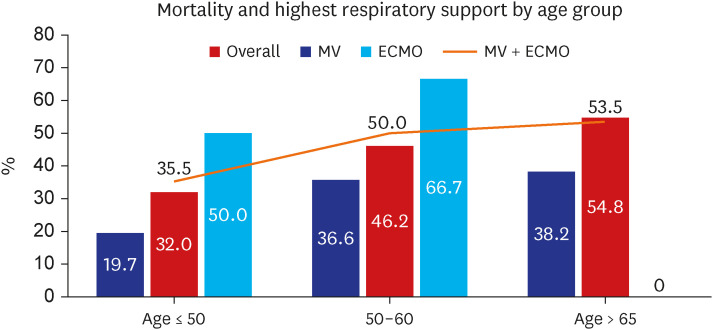
Table 2 shows the analysis results of predictive factors of mortality in all critical patients (N = 213) during the omicron wave period. The frequency of vasopressor use (28.8% vs. 15.6%, P = 0.022) and decreased consciousness (34.8% vs. 21.8%, P = 0.034) were significantly higher in the death group than in the survivor group. This finding along with the significant differences in initial laboratory findings indicate that the severity of disease at the time of initial hospitalization was higher in the death group than in the survivor group (Table 2). In the univariate analysis, age, breakthrough infection, initial vasopressor use, initial respiratory rate ≥ 22 breaths/min, altered mental status, initial blood urea nitrogen (BUN) >20 mg/dL, initial lactate dehydrogenase (LDH) > 600 IU/L, initial C-reactive protein (CRP) >8 mg/dL, poor laboratory findings during treatment (thrombocytopenia, low-density lipoprotein [LDL] elevation, creatinine elevation, and CRP elevation), application of MV, ECMO, or CRRT, and occurrence of bacterial pneumonia all showed significant differences between the death and survivor groups. The results of the multivariate analysis showed that five factors, age (OR, 1.084; 95% CI, 1.043–1.127), initial LDL > 600 IU/L (OR, 4.782; 95% CI, 1.584–1434), initial CRP > 8 mg/dL (OR, 2.940; 95% CI, 1.042–8.293), highest AST > 200 IU/L (OR, 12.931; 95% CI, 1.691–98.908), and application of MV (OR, 3.671; 95% CI, 1.294–10.420), were independent predictors of mortality in critical COVID-19 patients (Table 2). Initial saturation, infiltration, and treatment drugs (steroid, baricitinib, tocilizumab, Paxlovid, Lagevrio, remdesivir) had no significant effect on mortality (data not shown). The vaccination completion rate in all critical patients was only 31%, and there was no difference between the nonsurvivor and survivor groups (34.8% vs. 29.3%, P = 0.427) (Table 2).
Risk factors for mortality by age group
A subgroup analysis was performed in critical patients aged ≤ 50 years based on the characteristics evaluated in all critical COVID-19 patients (Table 3). Of the 71 patients, 14 patients died, corresponding to a significantly higher mortality rate of 19.7% during the omicron epidemic than the 5.6% rate during the delta epidemic (Supplementary Table 2). The proportion of patients with a BMI ≥ 25 kg/m2 was lower in the death group than in the survival group (35.7% vs. 52.6%). This indicated that the survival group included a greater number of obese patients, but the difference was not statistically significant (P = 0.372). All 14 patients aged ≤ 50 years (100%) who died had an underlying disease or had a BMI ≥ 25 kg/m2. Only two patients who died had no underlying disease, and 70% of the survivors also had underlying diseases. The importance of BMI decreased relatively as the severity of hospitalized critical patients increased (Table 3, Supplementary Table 3). There was no significant difference between the death and survivor groups with respect to the initial laboratory results, and most of the laboratory tests during treatment showed significantly worse values in patients aged ≤ 50 years (Table 3). MV, ECMO, and CRRT were all significantly more common in critical patients aged ≤ 50 years (Table 3).
In elderly critical patients aged > 50 years, 92.3% of patients in the death group had underlying disease. Further, similar to the entire critical patient group, the risk of death was high according to age; state of consciousness at admission; and the initial laboratory results such as platelet count, BUN, Cr, LDH, and CRP (Supplementary Tables 3 and 4). In patients who were older than 50 years, both MV (61.5% vs. 30.0%, P < 0.001) and CRRT (19.2% vs. 6.7%, P = 0.029) were used significantly more often in the death group. ECMO was not performed in any of the patients in the survivor group and in only two patients in the death group (3.8%), reflecting a lower ECMO implementation rate in the elderly than that during the delta wave (Supplementary Tables 2 and 4).
MV, ECMO, and CRRT were significantly more frequently performed in the death group, both in patients aged ≤ 50 years and > 50 years. Patients who had leukocytosis, lymphopenia, thrombocytopenia, AST/alanine aminotransferase levels 5 times higher than the upper limit of normal, LDH > 600 IU/L, Cr > 1.5 mg/dL, and procalcitonin > 0.5 during treatment had a significantly higher mortality rate (Table 3, Supplementary Table 4), while there was no difference in mortality rate according to chest radiography results and treatment at admission (data not shown).
The completion rate of vaccination in the patients aged ≤ 50 years was only 21.3%, which corresponded to only one-third of the national average at 87%. There was no difference in the vaccination rate between the survivor and death groups, possibly because of the low vaccination completion rate in both groups.
General characteristics of deceased patients younger than 50 years
In this study, 14 patients aged ≤ 50 years (19.7%) died; among them, 12 patients had underlying diseases, and 9 patients had a BMI of ≥ 25 kg/m2 (Supplementary Table 5). Overall, more than half of the patients had underlying diseases and had two or more underlying diseases. At the time of admission, 12 patients had findings of bilateral chest infiltration, and 7 patients (50%) had decreased consciousness or use of vasopressors from the time of admission. One patient developed complications of CLABSI and hospital-acquired pneumonia, and the mean time to death was 11.35 days. Although the national vaccination rate was over 80% during the study period, 50% of the patients aged ≤ 50 years who died were not vaccinated (never vaccinated, n = 7), and only three patients, who were all immunocompromised (having a tumor or taking immunosuppressants), received the third vaccine dose.
Comparison of clinical characteristics between periods
Data of severe patients with COVID-19 hospitalized during the delta period (between July 1, 2021 and November 30, 2021) were compared to those of severe patients with COVID-19 hospitalized during the omicron period. The overall mortality rate increased from 21.0% during the delta period to 30.6% during the omicron period. Particularly, the mortality rate in those aged ≥ 65 years was not significantly different between the delta and omicron periods (38.1% vs. 38.2%). In contrast, the mortality rate of in those aged ≤ 50 years was more than three times higher in the omicron period than in the delta period (19.7% vs. 5.6%, P = 0.003) (Supplementary Table 2).
With respect to the route of infection, the rate of unknown infection route was significantly higher during the omicron period than during the delta period (72.8% vs. 33.9%, P < 0.001). Although the vaccination completion rate increased from 13.6% in the delta period to 31.0% (P < 0.001), the overall vaccination completion rate was still only 31.0% (Supplementary Table 1). When examining the underlying diseases and risk factors, the percentage of patients with a BMI of 25 kg/m2 was lower in the omicron period than in the delta period (34.1% vs. 53.4%, P < 0.001), but the frequency of the underlying disease was higher than in the delta period (87.3% vs. 60.9%, P < 0.001). With respect to underlying disease, there were significantly more patients with any underlying disease or BMI ≥ 25 kg/m2 in the omicron period than in the delta period (93.9% vs. 82.4%, P < 0.001). Particular, all patients aged ≤ 50 years who died during the omicron period either had any underlying disease or had a BMI ≥ 25 kg/m2.
The rate of initial vasopressor usage or altered mental status was higher in the omicron period than in the delta period regardless of age, and both MV and CRRT usage rates were significantly higher in the omicron period (P < 0.001) (Supplementary Table 1). With respect to treatment, Paxlovid and Lagevrio were newly used in the omicron period, and the frequency of other treatments (plasma treatment, antibiotics, and conservative treatment) significantly decreased from 22.7% in the delta period to 3.3% in the omicron period as a standard treatment was established (P < 0.001) (Supplementary Table 1). In contrast to the higher mortality in the omicron period, the rate of complications such as CLABSI and fungal infection did not differ significantly between the omicron and the delta periods. However, the incidence of bacterial pneumonia was approximately 10% higher in the omicron period (21.0% vs. 31.0%, P = 0.008). The period from the time of diagnosis to death was shorter by 5 days in the omicron period than in the delta period (16.68 ± 16.758 days vs. 22.51 ± 17.137 days, P = 0.032) (Supplementary Table 1).
For patients aged ≤ 50 years, the percentage of those with BMI ≥ 25 kg/m2 significantly decreased from 69.7% in the delta period to 49.3% in the omicron period (P = 0.004), but there was no significant difference in the percentage of patients with BMI ≥ 30 kg/m2 between the two periods. Meanwhile, the percentage of patients who had any underlying disease or BMI ≥ 25 kg/m2 was higher by more than 10% in the omicron period than in the delta period (77.5% vs. 91.5%, P = 0.013) (Supplementary Table 2). The proportion of patients with underlying diseases more than doubled to 73.2%, and the number of underlying diseases in each patient also increased.
DISCUSSION
A previous study21 conducted in early 2022 analyzed the fatality rate and mortality risk factors in critical COVID-19 patients aged ≤ 50 years who received HFNC or higher respiratory therapy in the delta period, and we attempted to identify the specific characteristics of critical patients aged ≤ 50 years with the same condition in the omicron period. The overall S-CFR reported in the current study was 30.6%, much higher than the overall mortality rate of 1.54% based on the WHO data.1 Further, it was higher by more than 10% compared to the 21% mortality rate reported by a study conducted during the delta period in patients with similar characteristics and conditions. By age, the CFR for those aged ≤ 50 years increased from 5.6% to 19.7%, which was steeper than that in those aged > 50 years (from 29.3% to 36.6%). The CFR in the current study differs from those in epidemiological reports of the overall COVID-19 omicron pandemic. This is because the CFR analyzed in the current study is the S-CFR, which is the rate of death in severely ill patients. One of the important findings of this study is that unlike the overall population, severely ill patients had high S-CFR, and additional research for other variants are needed.
Among the critical patients in the omicron period, in addition to age, initial LDL >600 IU/L, initial CRP > 8 mg/dL, highest AST > 200 IU/L, and MV implementation were significant independent risk factors of mortality, consistent with previous studies.212324 Meanwhile, BMI, underlying disease, and vaccination status were not significant factors, possibly owing to the higher prevalence of BMI > 25 kg/m2 and underlying disease in the entire critical patient group than in the general patient population and to the small proportion of fully vaccinated patients.
In a study on adults aged ≥ 65 years in South Korea,24 HAI, diabetes mellitus, chronic lung disease, chronic neurologic disease, hypoxia, altered mental status, and CRP > 8.0 mg/dL were reported as risk factors for mortality in COVID-19 patients. Unlike data from the delta wave, no significance was observed for underlying diseases in both univariate and multivariate analyses in this study. This result is thought to be because underlying disease is a common risk factor for severity and death. Although the fatality rate was high in the patients with underlying diseases, it did not show any significance as the rate of underlying diseases increased in all critical patients. In contrast to previous findings of underlying diseases such as nosocomial infection24 and hypertension being a risk factor, the current study found no significance for underlying diseases. This is believed to be possibly owing to the higher frequency of underlying disease among all patients in the omicron period than in the delta period. The current study showed that the frequency of underlying disease in critical patients was significantly higher in the omicron period than in the delta period (87.3% vs. 60.9%, P < 0.001). The KDCA report3 showed that 16,118,490 cases were confirmed during the omicron outbreak (fifth period), which corresponded to 95.2% of the cumulative confirmed cases. The daily average number of confirmed cases was 187,424, with a minimum of 17,075 and a maximum of 621,177. This corresponded to 60 times the daily average number of confirmed cases with a total of 649,534 confirmed cases and 3,137.8 daily average confirmed cases during the delta period (fourth period). As mentioned previously, reports have shown that it is difficult to find consistent mortality predictors except for age in large-scale studies in the real world, and the actual prediction rates of several known risk factors are even not high.2526 Moreover, further studies are needed to explore whether the underlying disease status, age, or the severity of condition at the time of admission predicts morbidity and mortality in a large-scale epidemic. This will be helpful in efficient bed management in the future. With limited resources (hospitals, health care workers), it is crucial to predict the risk of aggravation or mortality of infectious disease because it is a key component of hospital operation.
Although 73.2% of critical patients aged ≤ 50 years during the omicron wave had an underlying disease, Paxlovid and Lagevrio were not prescribed. This was despite their proven effectiveness in preventing exacerbations and their recommendation to be prescribed in patients with COVID-19 with underlying medical diseases. Paxlovid was initially allowed only for limited patients; these included patients aged ≥ 65 years, immunosuppressed patients aged ≥ 12 years, and patients with underlying diseases aged ≥ 50 years or older. After February 21, 2022, the indication for Paxlovid was expanded to senior citizens aged ≥ 60 years, patients with underlying diseases aged ≥ 40 years, and immunocompromised patients aged ≥ 12 years. However, the prescription rate was still very low. This may be proof that there are many cases of late detection in young people who have already progressed to severe disease at the time of diagnosis. Further, it can also be reflection of the low rates of drug prescription for COVID-19 in the general public. The March report of the KDCA27 showed that Paxlovid, which was introduced on January 13, 2022, was prescribed for only 47,000 cases nationwide over a 2-month period, supporting the above finding. Currently used treatment drugs for COVID-19 have already been proven to be effective.272829 It is considered that early pharmacological intervention in patients with underlying diseases and risk factors (e.g., obesity), along with an active initial diagnosis, will markedly reduce the severity and mortality related to COVID-19 infection.
A previous study reported that compared to critical patients aged > 50 years, critical patients aged ≤ 50 years had a higher BMI and a lower fatality rate because of a lower severity of their condition at admission. The current study also found that the average BMI of patients in this age group was higher than that of the general population. Further, for patients in this age group, those critical patients during the omicron period had worse S-CFR at the time of hospitalization than those infected in the delta period. Regarding obesity, 49.3% of all critical patients aged ≤ 50 years were obese (BMI ≥ 25 kg/m2), which is higher than the average in adults. In a study evaluating Korean pediatric COVID-19 patients,30 8 of the 39,000 pediatric patients had severe disease, and their mean BMI was 29.3 kg/m2, higher than the national average. Similar trends were observed in our study. Overseas studies1431 also support the hypothesis that obesity is associated with exacerbation of COVID-19 and mortality. One study explored the mechanism by which obesity is associated with the critical severity of COVID-1932 and found that the cytokine storm caused by interleukin-6 secretion by adipocytes increased the risk of complications and led to hospitalization and intensive care unit admission. A recent report33 also showed that 38% of the adult population in 2020 had a BMI ≥ 25 kg/m2; accordingly, proper COVID-19 management in the increasing obese population should be emphasized.
In the current study, among the 14 patients aged ≤ 50 years who died, 5 patients had a BMI of ≥ 25 kg/m2 (35.7%) (Supplementary Table 5), which was not significantly different from the average BMI of adults. However, when the underlying diseases were also considered, all of these 14 patients who died had an underlying disease or BMI ≥ 25 kg/m2. These results can be explained by the relatively low evaluation of BMI in critically ill patients who died as the epidemic increased and the number of critically ill patients increased. Furthermore, some studies abroad have reported that omicron has a lower correlation with BMI than delta,7 which requires further investigation.
Examining Tables 1-3 and Supplementary Table 1, the laboratory test results or the severity of condition at the time of hospitalization increased significantly in the omicron period from the delta period, and many patients with severe conditions were hospitalized. We hypothesized that this was because of the difference in the epidemic size rather than the effect of the omicron variant itself. As previously mentioned, the total number of confirmed cases during the omicron epidemic was 16,118,490, with an average of 187,424.3 daily confirmed cases, and this was 60 times higher than that during the delta epidemic. The number of beds for severe cases differed only by 500 beds from the maximum estimate of 2,360 beds in the delta period to the maximum estimate of 2,825 (private + public) in the omicron period. As a result, the severity of severe hospitalized patients seems to have differed significantly between the periods. There have been reports that the epidemic during the omicron period was more large scale in South Korea than in other countries because the confirmation rate in previous epidemics was not high.89 Accordingly, it is thought to have shown different characteristics compared to those of previous epidemics. Hospitals have limited capacity for increasing the number of beds, especially for critically ill patients, owing to limited human resources and facility equipment. Thus, efficient management of severely ill patients using limited beds is more emphasized. In addition, it will be of great help if further studies are conducted for each variant to determine which of the various risk factors are significant in large-scale epidemic situations.
The disease severity, vaccine effectiveness, and mortality rate of the omicron variant infection have not yet been standardized, and findings have been conflicting. Most studies showed that the infection caused by the omicron variant has lower severity and mortality rates than those caused by the delta or alpha variant.3435 However, there is also evidence that omicron variant has low severity but not mortality.36 Although some studies reported that for the omicron variant, the probability of critical aggravation was 0.23%,37 the infectivity was 13 times higher. 38 Moreover, the overall number of critical cases did not seem to decrease significantly, considering the high reinfection rate and immune evasion. In addition, there are still unknown effects of the omicron variant in the real world because there are reports of increasing deterioration of other diseases, 39 in addition to the mortality rate being not low or rather high in specific patient groups,40 unvaccinated groups,618 or partially vaccinated groups.1941 Studies from other countries540 have also reported that it is difficult to predict the severity, vaccine effectiveness, and mortality rate of the omicron variant infection.
The main reasons why it is challenging to predict the effect of COVID-19 variants like omicron are related to the acquisition of immunity from vaccination and previous infections and the need to analyze different risk factors in specific groups. Studies have shown high mortality related to the omicron variant in certain patient groups,40 including the hospitalized, solid organ transplantation, chronic dialysis, and hematologic malignancy patients. In this study, only Korean critical patients who needed hospitalization were evaluated, and although there was a difference by age, the mortality rate was as high as 19.7% even for those aged 50 years or younger. These results highlight that with the omicron variant, disease severity at the time of diagnosis was worse in certain groups of patients, and further studies should explore this in other critical patients.
Some studies also that showed high mortality in the unvaccinated618 or partially vaccinated1941 patients, and consistent results were found in this study. The mortality differs by 3 to 23 times between unvaccinated and vaccinated individuals, but several studies in Europe,41 South America,19 Africa,6 and Asia18 consistently reported a low mortality rate with the omicron variant owing to the effect of vaccination and immunity. Although the vaccination rate of critical patients during the omicron period was significantly higher than that during the delta period, it was still only 31.0%, which corresponded to less than 50% the national data. In addition, only 15 of the 71 critical patients aged ≤ 50 had completed their vaccination, accounting for only 20%. In particular, only 3 of the 14 patients aged ≤ 50 years who died were vaccinated, showing that the vaccination completion rate was relatively low for all critically ill patients. In this study, which recruited critical patients, although there was no significant difference in the vaccination completion rate between the survivor and death groups, the results highlighted a low vaccination rate in the overall population of critically ill patients.
This study has several limitations. First, there were many cases in which the variant type was not identified, and these cases could not be analyzed according to the variant. However, considering the KCDA report42 that more than 90% of all patients during the omicron period had omicron and sub-variants, it was thought there would be no significant bias even if all patients were considered to have an omicron variant.
Second, as pointed out in the previous study, we only included severely ill inpatients, which may not be representative of all COVID-19 patients. It is challenging to directly compare the fatality rate before and after the omicron period. Death and survival were compared among critically ill patients, and thus, it was possible that factors found to be significant in other studies (e.g., vaccination and obesity) were found to be insignificant in the current study. While we recognize the limitations of our study design, it is important to note that the title of our study specifically focuses on severely ill patients, which is consistent with the study population we included. Despite these limitations, our study provides important insights into the impact of the Omicron variant on critically ill COVID-19 patients aged ≤ 50 years.
Finally, there may be outcome variables that did not derive a significant outcome value, as there were only 14 deaths among those aged ≤ 50 years. This is believed to be the result of restricting the study population to a specific age range and to specific time periods of the epidemic. Nevertheless, the 14 deaths in patients aged ≤ 50 is significant considering their age and the fact that they are critical patients. We tried to compensate for this by analyzing characteristics of 14 deaths (Supplementary Table 5). In addition, we compared the delta wave group and the omicron wave group by recruiting the same patient population (i.e., those who had similar characteristics).
Compared to other studies, the current study included a larger number of critical patients aged ≤ 50 years, and data were compared between periods of variant infection. The findings provide important baseline evidence for determining the risk factors of critical disease in the future. Furthermore, because this study was a multicenter study that conducted an additional comparison between epidemic periods, the results have important implications in developing the risk factor criteria for critical patients with COVID-19 omicron infection.
In conclusion, critically ill COVID-19 patients aged ≤ 50 years infected during the omicron period, more than 70% patients have underlying disease. Further, disease severity at the time of hospitalization was worse than that during the delta period owing to the increased epidemic size and the limited number of beds. The effect of obesity on disease severity was relatively low, and the S-CFR reached 20% even for those aged ≤ 50 years. Compared with general population, those with severe infection in the overall population, the age ≤ 50 years group, and the age > 50 years group had significantly lower vaccination rates. All the patients aged ≤ 50 years who died had an underlying disease or had a BMI of ≥ 25 kg/m2. Notably, there was a lack of prescription for Paxlovid for these patients although they satisfied the prescription criteria. Although the severity of the omicron variant epidemic was expected to be relatively low, the total number of critical patients increased as the epidemic size increased. In addition, there was a possibility of progression to critical illness or death in young adult patients infected with the omicron variant. Early diagnosis and active initial treatment was necessary, along with the proven methods of vaccination and personal hygiene. Further studies are needed to explore the difference in mortality among SARS-CoV-2 variants, especially in critical patients.
 XML Download
XML Download