

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Myasthenia gravis (MG) is a rare classic autoimmune disease caused by a target-specific antibody-mediated process.1 The blockade of neuromuscular transmission at acetylcholine receptors results in varying degrees of muscle disorders including eyelid movement, facial expression, chewing, talking, swallowing, shortness of breath and weakness in the arms, hands, fingers, legs, and neck.2 The annual incidence of MG ranges from 0.3 to 2.8 per 100,000 people worldwide.3 In current treatment guidelines, non-target-specific immunosuppressive drugs, such as corticosteroids or non-steroidal immunosuppressive agents (ISAs), are used as first-line therapy for all patients who have not met treatment goals with acetylcholinesterase inhibitors (AChEIs).4 Those immunosuppressant therapies are fairly successful over the last 80 years, reducing MG-attributable mortality from 70% in the 1930s to < 10% today.5 Compared to markedly increased MG mortality until few decades ago, life expectancy is now close to normal in developed countries.67 A relative mortality of 1.41 was reported for Acetylcholine Receptor MG in individuals diagnosed between 1985 and 2005 in Denmark.6 A study conducted in Norway did not present any increased mortality in patients with MG compared with controls after 1995.7 Despite the considerable advancements in MG treatment, some patients still poorly respond to therapy. For those patients with refractory MG (rMG) who fail to respond to substantial use of conventional treatment, chronic intravenous immunoglobulin (IVIG) or plasma exchange (PE), or cyclophosphamide can be considered as rescue therapy.8 Nonetheless, patients with rMG had a high fatality rate and experience frequent MG exacerbation, hospital admission, and respiratory failures that require mechanical ventilation.9101112 In addition, studies on patients with rMG are quite limited to case series or short descriptive studies,13141516 it is difficult to establish their clinical features and estimate their outcomes. Given the need to address the current treatment gap for rMG, the clinical characteristics and prognoses of rMG must be defined in real-world practice. Thus, we formulated two aims: 1) determining the major clinical outcomes of rMG; and 2) describing the pattern of pharmacotherapy regimens for patients with rMG.
METHODS
Study design and data sources
We conducted a longitudinal, retrospective, and nationwide cohort study using the National Health Insurance Service (NHIS) database of South Korea between January 01, 2002 and December 31, 2017. The national health insurance program provides universal healthcare coverage for the entire South Korean population of ≥ 50 million. The NHIS database contains inpatient and outpatient medical service utilization records and includes information on de-identified individual patient data, sociodemographic characteristics, procedures, diagnoses coded by the International Classification of Diseases Tenth Revision (ICD-10) code system, and drug prescriptions.17 The drug prescription records include the date of prescription, generic name, dosage, the days of supply, and route of administration. Death records were obtained from the NHIS database linked to death certificate data provided by Statistics Korea.
Study population
The cohort was constructed of actively treated patients with MG (aMG) who satisfied the following criteria: 1) a principal diagnostic code of MG (ICD-10 code G70.0) between 2003 and 2016, 2) no history of MG diagnosis within the previous year to restrict inclusion to patients with incident MG, 3) ≥ 18 years old at the time of first MG diagnosis, 4) completed at least a 1-year follow-up after MG diagnosis to secure a minimum follow-up period to determine whether they are patients with rMG or not, and 5) prescriptions of corticosteroids with mean daily prednisolone-equivalent dose > 20 mg (Supplementary Table 1 for corticosteroid equivalent dose conversion) for > 2 months within 2 years after MG diagnosis to exclude patients with mild or ocular MG who were generally treated with a lower dose of corticosteroids.
Among the aMG cohort, patients with rMG were defined based on a previous study as those who were administered PE or IVIG at least 3 times per year after treatment with more than one corticosteroid or ISA following MG diagnosis, and the remaining patients were defined as patients with non-rMG.8 The date of cohort entry was defined as the first date of MG diagnosis. The date of rMG incidence (index date for rMG) was defined as the date of first PE or IVIG prescription in a period when rMG criteria was satisfied having at least three PE or IVIG prescriptions in a year.
Outcome measures
The outcome measures were all-cause mortality, myasthenic crisis, hospital admission, pneumonia or sepsis, and emergency department (ED) visits, as captured at 1, 3, and 5-year and overall follow-up period. When multiple records refer to the same outcome, the earliest recorded date was the event date. Mortality, hospital admission, and ED visits data were identified from the healthcare utilization and death records in the NHIS database. The myasthenic crisis was defined as having a procedure code for endotracheal intubation, mechanical ventilation, or continuous or bilevel positive airway pressure noninvasive ventilation,10 and pneumonia or sepsis which was confirmed using diagnostic ICD-10 codes (Supplementary Table 2).
Treatment pattern
The patterns of pharmacotherapeutic regimens were compared between patients with rMG and non-rMG. In patients with rMG, we determined treatment patterns in the 2-year period before and after the date of rMG incidence. For the patients with non-rMG, we determined the treatment patterns in the 2-year period before and after the date of initial IVIG or PE procedure (this criterion was set to be comparable to the index date for the patients with rMG; only patients with non-rMG who received IVIG or PE were included in this analysis). We calculated the proportion of patients who used AChEIs (pyridostigmine), corticosteroids (methylprednisolone, prednisone, betamethasone, dexamethasone, triamcinolone, and hydrocortisone), and ISAs (azathioprine, tacrolimus, mycophenolate mofetil [MMF], cyclosporine, and methotrexate). Rituximab was not included in this analysis as the agent was not eligible for reimbursement for the indication of MG in South Korea. We determined the mean and median daily doses of corticosteroid using the prednisolone-equivalent dose every 3 months.18 In this analysis, the prescriptions of low-dose corticosteroid (prednisolone-equivalent dose ≤ 5 mg/day) were excluded, as these prescriptions would be for low-dose long-term maintenance treatment of MG.
Statistical analysis
We assessed baseline characteristics 1 year before the date of cohort entry, including sex, age, Charlson comorbidity index (CCI),19 and comorbid conditions that commonly accompany MG2021 (Supplementary Table 2). To compare the characteristics between patients with rMG and non-rMG, the t-test was used for continuous variables and the χ2 test or Fisher's exact test (expected frequency < 5) for binary variables. The Cochran-Mantel-Haenszel test was used to compare subgroups of age and CCI. The Cox proportional hazards model was used to estimate the hazard ratios (HRs) and 95% confidence intervals (CIs). The model was adjusted for all baseline characteristics and whether a patient had thymoma (including malignant and benign neoplasm) or thymectomy, before and after the MG diagnosis. Kapan-Meier analysis and log-rank test were used to estimate the time to occurrence of clinical outcomes in rMG compared to non-rMG. To identify the difference in patterns of treatment regimen between groups, we used the χ2 test for a linear trend. A P value of < 0.05 was considered statistically significant. All statistical analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Characteristics of the study cohort
We identified 4,298 patients with incident aMG; 47 with rMG and 4,251 with non-rMG (Fig. 1). The number of patients with prevalent aMG increased from 732 in 2003 to 4,401 in 2016 (Supplementary Table 3). Patients with rMG were younger (45.5 vs. 52.2 years, P = 0.017), included more female (72.3% vs. 54.4%, P = 0.014), and had more severe CCI scores (≥ 3: 14.9% vs. 6.8%, P = 0.025) than patients with non-rMG. All comorbidities were comparable between groups except for malignant neoplasm of the thymus (P = 0.027). Thymoma and thymectomy were more prevalent in patients with rMG than in patients with non-rMG (Table 1, Supplementary Tables 4 and 5). In addition, 53.2% of patients with rMG entered rMG status within 1 year after MG diagnosis (Supplementary Table 6). The mean follow-up period was 7.1 ± 3.9 years for rMG and 6.9 ± 4.0for non-rMG, which enabled us to fully identify potential rMG transition from non-rMG.
Fig. 1
Flowchart for the identification and selection of the study cohort.
MG = myasthenia gravis, aMG = actively treated myasthenia gravis, rMG = refractory myasthenia gravis.
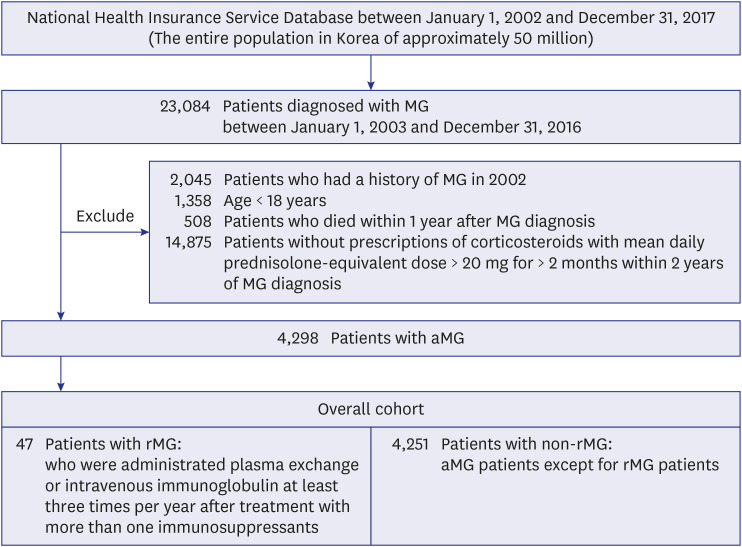
Table 1
Baseline characteristics of the patients with incident rMG and those with non-rMG
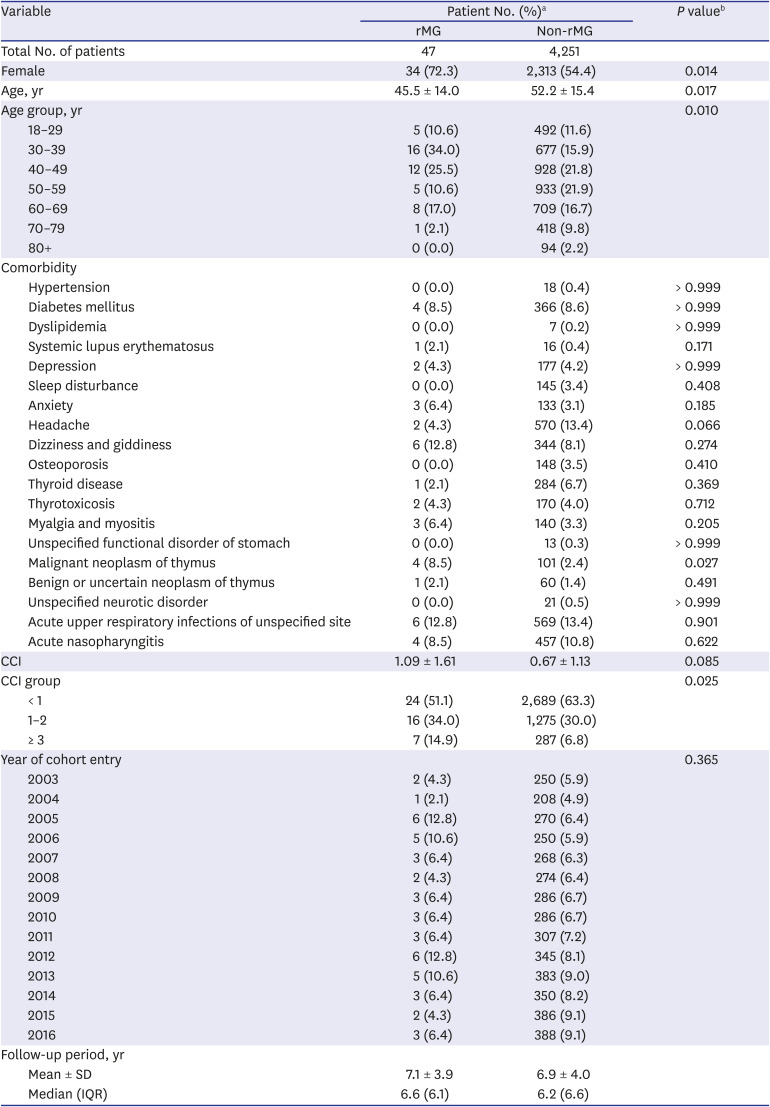
Data are shown as mean ± SD or number (%).
rMG = refractory myasthenia gravis, CCI = Charlson comorbidity index, SD = standard deviation, IQR = inter quartile range.
aPercentages may not total 100 because of rounding; bThe t-test was used for continuous variables, χ2 test or Fisher's exact test (expected frequency < 5) was used for binary variables, and Cochran-Mantel-Haenszel test was used for the subgroup difference in age and CCI. P values of < 0.05 were significant.
Clinical outcomes
The risk of adverse clinical outcomes was significantly higher in rMG than in non-rMG in both unadjusted and adjusted analyses (Table 2). The adjusted HRs were 2.49 (95% CI, 1.26–4.94) for all-cause mortality, 3.14 (2.25–4.38) for the myasthenic crisis, 1.54 (1.15–2.06) for hospital admission, 2.69 (1.74–4.15) for pneumonia or sepsis, and 1.81 (1.28–2.56) for ED visits in the overall follow-up period. Kaplan-Meier curves for the five outcomes showed a significant difference in long-term prognoses between groups (Fig. 2). The cumulative probability of mortality in 15 years was 0.53 and 0.21 in patients with rMG and non-rMG, respectively (P = 0.040). The probability of the myasthenic crisis was 0.85 in 5 years in rMG and 0.25 in non-rMG (P < 0.001). Both groups had a high probability of hospital admission in the early phase (0.91 and 0.68 in 1 year in rMG and non-rMG, respectively; P < 0.001). The risks of pneumonia or sepsis and ED visits gradually increased in both groups but were higher in rMG than in non-rMG over the follow-up period (P < 0.001).
Table 2
Risk of adverse clinical outcomes in patients with rMG compared to that in patients with non-rMG
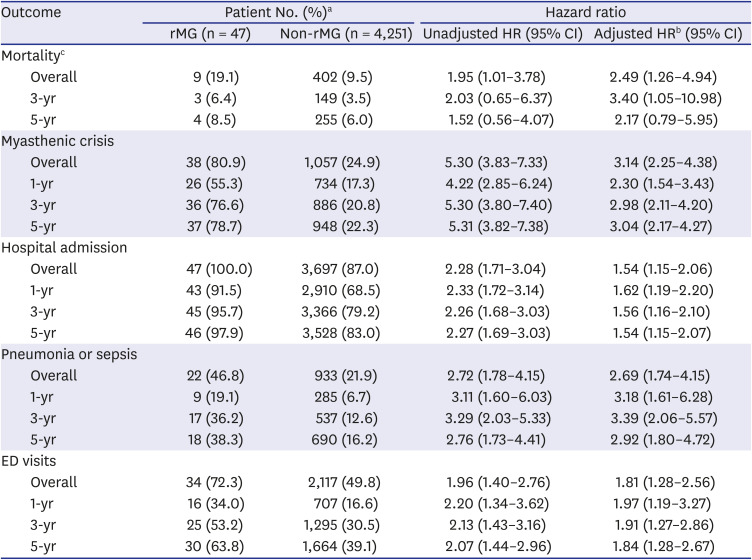
rMG = refractory myasthenia gravis, HR = hazard ratio, CI = confidence interval, ED = emergency department.
aTotal percentage may not be 100 because of rounding; bAdjusted for baseline characteristics as shown in Table 1 and whether they had thymoma or thymectomy before and after the date of myasthenia gravis diagnosis; cMortality within 1-year could not be estimated owing to the cohort inclusion criterion that patients were to be followed up for at least 1-year.

Treatment pattern
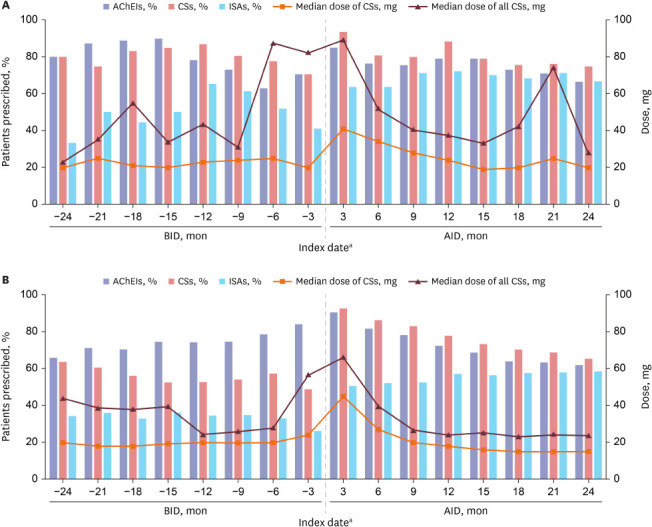
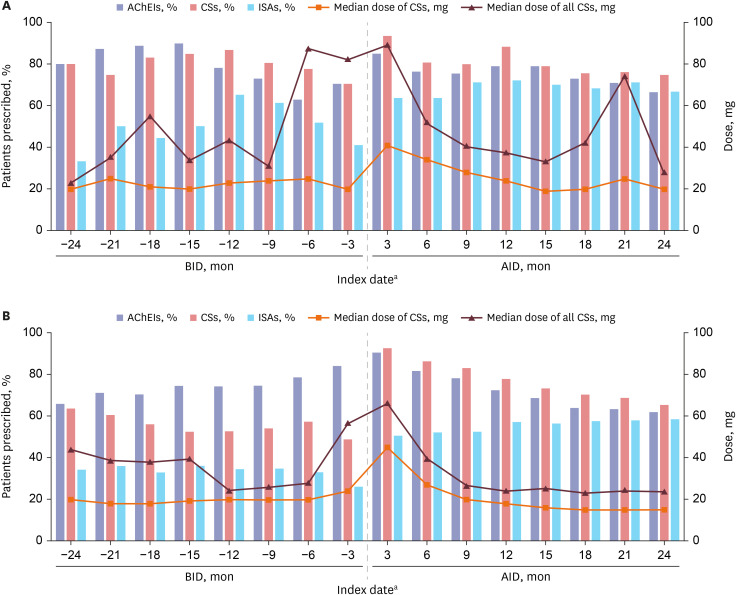
The prescription rate of AChEIs was high for both rMG and non-rMG (Fig. 3 and Supplementary Table 7). There were more prescriptions of corticosteroids and ISAs for rMG than for non-rMG, even before the index date (BID). The proportion of patients who used corticosteroids 12 months BID was 87.0% and 52.8% in rMG and non-rMG, respectively; the proportion of patients who used ISAs was 65.2% and 34.6%. After the index date (AID), > 90% of the patients used corticosteroids 3 months AID in both groups but the subsequent downward trend of corticosteroid use was more conspicuous in patients with non-rMG. For both groups, ISA use in AID was almost doubled compared to that of BID, where the most used ISA was azathioprine, followed by tacrolimus, MMF, and cyclosporine (Supplementary Tables 8 and 9). For rMG patients, the mean dose of corticosteroids in BID was fluctuated and peaked at 6 months BID; for non-rMG patients, the mean dose of corticosteroids was steadily decreased until 3 months BID, although a slight increase was shown at 3 months BID (P < 0.001). The corticosteroid dose was gradually decreased but peaked at 21 months AID for patients with rMG, whereas it was consistently decreased for patients with non-rMG (Fig. 3 and Supplementary Table 7).
Fig. 3
Comparative pattern of drug prescriptions in the 2-year period BID and AID for the (A) patients with rMG and (B) patients with non-rMG.
AChEI = acetylcholine esterase inhibitor, CS = corticosteroid, ISA = non-steroidal immunosuppressive agent, rMG = refractory myasthenia gravis, BID = before the index date, AID = after the index date.
aThe index date: the date of rMG incidence defined as the date of first PE or IVIG procedure when the procedures were provided at least three times per year (in rMG) and the date of initial IVIG or PE procedure (in non-rMG).
DISCUSSION
We conducted a longitudinal, retrospective, and nationwide cohort study to examine the risk of major adverse clinical outcomes and treatment patterns in patients with rMG. We observed distinct demographic and clinical features of refractory patients at the baseline. The patients with rMG were significantly younger, predominantly female, more frequently associated with thymoma, and received active treatment with ISAs and thymectomy than the patients with non-rMG. In unadjusted and adjusted analyses, we identified significantly higher risks for all-cause mortality, myasthenic crisis, hospital admission, pneumonia or sepsis, and ED visits for patients with rMG than for those with non-rMG.
These results were comparable to those of previous studies, wherein the patients with rMG were younger and had more female than the patients with non-rMG.112223 The higher prevalence of thymoma and thymectomy rate for rMG also were reported previously.11 A recent randomized trial showed that thymectomy improved clinical outcomes in patients with nonthymomatous MG.24 Among patients without thymoma in our study, the proportion of those who underwent thymectomy was 30.8% and 15.8% for rMG and non-rMG, respectively (Supplementary Table 4). Despite the use of preemptive thymectomy, some patients progressed to rMG. Moreover, although the thymectomy rate for patients without thymoma was higher in rMG, the risks of adverse clinical outcomes were higher in rMG.
There were significantly high risks of adverse clinical outcomes in rMG compared to non-rMG, including mortality (2.49 times), myasthenic crisis (3.14 times), hospital admission (1.54 times), pneumonia or sepsis (2.69 times), and ED visits (1.81 times). These results were in line with previous studies. A 1-year followed-up cohort study in the US, which included 403 and 3,811 patients with rMG and non-rMG, respectively, reported higher risks for mortality (5.1% vs. 2.7%), myasthenic crisis (21.3% vs. 6.1%) in rMG than in non-rMG.25 In a Chinese cohort study of 2,195 patients with MG, the mortality rate was 5.88% in 10 years. They reported that the majority of deaths occur 5–10 years after the onset of MG and rarely within 5 years,26 while our results showed a gradual increase in the risk of mortality over 15-year follow-up period. A Japanese study of 165 and 3,137 patients with rMG and non-rMG, respectively, followed-up for 1 year after the onset of MG, reported much higher risks in rMG (19.5 times for myasthenia exacerbation and 9.6 times for hospitalization) than in non-rMG.27 These high risks may be an overestimation, as patients with rMG in this Japanese study were compared with patients with non-rMG, which included patients with mild symptoms or ocular MG. In our study, we restricted the study cohort to aMG; thus, patients with mild symptoms or ocular MG were excluded.
In pharmacotherapeutic regimen analyses, the rate of using all drug classes and doses of corticosteroids was generally higher in rMG. This difference of the drug regimens was more remarkable BID rather than AID, which suggested that patients with rMG are unresponsive to treatment before the refractoriness became apparent in patients with rMG and the ongoing deterioration of disease status might have required more intensive treatment.
For both groups, the proportion of patients using corticosteroids and ISAs was near the lowest 3 months BID. We speculated that discontinuation of corticosteroids or ISAs in stable patients might induce symptom rebound. On the other hand, we also observed an increase in mean corticosteroid dose at the corresponding period, which might reflect suboptimal treatment response in some patients with a potential to progress into rMG. Thus, a requirement for a sudden increase in corticosteroids dose (above the mean dose of 80 mg) before the incidence of rMG should warn the physicians to monitor the patients more carefully and prepare an additional treatment plan. In accordance with the International Consensus Guidance,8 the main treatment options for aMG are AChEIs, prednisolone, and azathioprine in Korea (Supplementary Tables 8 and 9). Among the ISAs, azathioprine was used the most, whereas tacrolimus and MMF were used less. Of note, ISA use AID almost doubled compared to that BID. The use of ISAs, especially tacrolimus and MMF, was more prevalent in rMG than in non-rMG: 41.9% vs. 36.5% for azathioprine, 20.9% vs. 8.7% for tacrolimus, and 14.0% vs. 7.5% for MMF 1 year AID, respectively. This suggests that patients with rMG may have switched to tacrolimus or MMF after the use of azathioprine first. Nevertheless, patients with rMG seemed to remain unstable and there are not many different strategies to treat these refractory patients, requiring PE or IVIG therapy on a regular basis.
Considering the high rate of mortality and morbidity in patients with rMG, the use of alternative treatment options that target novel immunological pathways or pathogenetic mechanisms of MG would be beneficial.28 Recent advancements in the use of monoclonal antibody enable their application for rMG treatment, such as rituximab, which targets CD20+ B cells,2930 and eculizumab, a humanized monoclonal antibody that specifically binds with high affinity to human terminal complement protein C5 and prevents the formation of the membrane attack complex.3132 Although experts' consensus could not be reached, rituximab is already used as a rescue medication for rMG, and recent studies suggested that rituximab is associated with favorable treatment response in patients with rMG or new-onset MG compared to conventional immunosuppressant therapy.3033 Eculizumab also has been approved in other countries,343536 and a phase II study of eculizumab37 and the subsequent phase III study in rMG (REGAIN study) presented a potential benefit of eculizumab treatment in patients with rMG.38 The long-term safety and efficacy of eculizumab were favorable with no meningococcal infection, a reduction in MG exacerbation rate, and an improvement in the quality of life over 3 years.3940
This study has several strengths and reported novel results. First, we demonstrated a higher risk of major adverse clinical outcomes for patients with rMG than for those with non-rMG using the nationwide data. Second, we extensively examined and compared the pharmacotherapeutic regimen for patients with rMG and non-rMG, providing detailed and useful insights into the treatment of MG in real-world practice. Third, based on the time to rMG development from aMG diagnosis, the first year of aMG diagnosis may be a critical period wherein intensive monitoring is required to prevent transition to rMG and consider appropriate treatment options. Last, usually claim data cannot retrieve information on non-reimbursed prescriptions. However, the insurance system in Korea currently covers most of the treatments for severe cases of MG. Moreover, as MG is classified as a rare intractable disease (RID) in Korea, the necessary clinical information to register MG patients as RID should be provided by physicians, which guarantee precise diagnosis ascertainment. Therefore, we are sure that the NHIS database utilized in this study offered highly accurate diagnosis and treatment information for MG cohort.
This study also had several limitations. First, we used stringent criteria to identify patients with certain rMG; thus, some patients with rMG may have been excluded from the study cohort or misclassified as non-rMG group. However, as we also construct aMG cohort with strict criteria, excluding patients suggestive of mild or ocular MG, we provided more precise clinical evidence and practical insight ensuring clinical comparability between rMG and non-rMG cohorts, while showing results consistent with previously known facts regarding MG. Second, given the criteria of rMG already implicate the higher predisposition to having MG crisis in rMG, the higher adverse clinical outcomes such as MG crisis and hospital admission presented in rMG seem for granted. However, our main aim was to evaluate the adverse clinical outcomes between rMG and non-rMG at certain periods and provide clear comparisons statistically and quantitatively. We are sure at least in this perspective, our limitation might be mitigated. Third, as the crude mortality rate or standardized mortality rate of aMG and risk factors associated with prognosis in aMG need more epidemiological findings as well, these focuses would be further interesting areas in the future which couldn't be researched in this study. Last, although we included the entire patients in South Korea, the number of defined patients with rMG was small, which suggests the need to interpret the results with caution and to conduct further large-scale studies.
In conclusion, this study reported the high risks of adverse clinical outcomes in rMG compared to non-rMG. Despite the unstable and severe disease prognosis in the patients with rMG, their pharmacotherapeutic strategies were similar to those of non-rMG. Intensive monitoring and the introduction of timely treatment options in the early phase of MG are required in patients with potential rMG. Our findings suggest that healthcare practitioners and policy makers should focus on practical decision-making when caring for patients with rMG.
 XML Download
XML Download