

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Mortality from cardiovascular diseases (CVDs) had increased in both developing and developed countries.1)2) In developing countries, CVD has become a leading cause of disease burden.3) However, a decreasing trend in the mortality rate has been observed in developed and high-income countries, such as the United States, United Kingdom, Australia, Japan, and Republic of Korea, owing to improved lifestyle and better disease management.1)2) In Korea, CVDs, in particular total heart diseases, are the leading causes of death among single-organ diseases.4) Understanding the trends in CVD related mortality is important in reducing healthcare burden and developing strategies for reducing CVD mortality. Studies have reported 30-year trends in CVD mortality.5)6) However, the CVD mortality rates and trends vary across age. Few studies have examined temporal trends in CVD mortality by age group. Considering the rapidly aging population structure, it deems crucial to examine age- and sex-specific CVD mortality trends. Hence, we updated and examined crude, age-standardized, and age-stratified CVD mortality rates in Korea over the 36-year period based on the Cause of Death Statistics.
METHODS
Annual microdata on mortality were obtained from the Korean Statistical Information Service (KOSIS) and Microdata Integrated Service (MDIS) managed by Statistics Korea (formerly known as the Korea National Statistical Office). Mortality statistics with cause of death were available from 1983 to 2018. Causes of death were coded according to the International Classification of Disease, 10th Revision. For the purpose of this study, one category was analyzed for all diseases of circulatory system (I00-I99), and the following 6 subcategories (not mutually exclusive) were considered: total heart diseases (I00-I13 and I20-I51), hypertensive heart diseases (I10-I13), ischemic heart diseases (I20-I25), myocardial infarction (I21-I23), heart failure (I50), and cerebrovascular diseases (I60-I69).
The total heart diseases category (I00-I13 and I20-I51) includes acute rheumatic fever and chronic rheumatic heart diseases (I00-I09), hypertensive heart diseases (I10-I13), ischemic heart diseases (I20-I25), and other heart diseases (I26-I51). The acute rheumatic fever and chronic rheumatic heart diseases category (I00-I09) includes rheumatic fever without cardiac involvement (I00), rheumatic fever with cardiac involvement (I01), rheumatic chorea (I02), rheumatic mitral valve diseases (I05), rheumatic aortic valve diseases (I06), rheumatic tricuspid valve diseases (I07), multiple valve diseases (I08), and other rheumatic heart diseases (I09). The hypertensive heart disease category (I10-I13) includes essential primary hypertension (I10), hypertensive heart disease (I11), hypertensive renal disease (I12), and hypertensive heart and renal disease (I13). The ischemic heart diseases category (I20-I25) includes angina pectoris (I20), acute myocardial infarction (I21), subsequent myocardial infarction (I22), certain current complications following acute myocardial infarction (I23), other acute ischemic heart diseases (I24), and chronic ischemic heart disease (I25). Conduction disorders and cardiac arrhythmias (I44-I49) were included among other heart diseases (I26-I51). The cerebrovascular diseases category (I60-I69) includes hemorrhagic stroke (I60-I62), cerebral infarction (I63), unspecified stroke (I64), and other cerebrovascular diseases (I65-I69). The hemorrhagic stroke category (I60-I62) includes subarachnoid hemorrhage (I60), intracerebral hemorrhage (I61), and other nontraumatic intracranial hemorrhage (I62).
All analyses were stratified by sex, except for the absolute number of deaths from CVDs. We calculated the crude and age-standardized CVD mortality rate using the direct standardization method, with sex- and 5-year age interval-specific 2018 Korean population structure as the standard population. The crude and age-standardized mortality rates were calculated in all age groups. We also calculated age-stratified mortality rate to explore the patterns of age-specific mortality rate using 10-year age intervals. Lastly, we calculated male to female ratios of age-standardized mortality rates using the overall (men and women combined) 2018 Korean population as the standard population. All statistical analyses were performed using R Statistical Software version 4.0.1 (R Foundation for Statistical Computing, Vienna, Austria).
The study protocol was approved by the Institutional Review Board of the Yonsei University College of Medicine (4-2020-0207).
RESULTS
Number of deaths from cardiovascular diseases
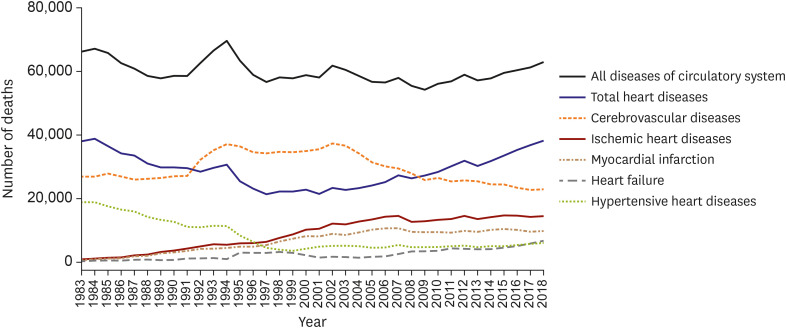
Figure 1 shows the number of CVD deaths from each year (additional data available in Supplementary Figure 1, Supplementary Tables 1 and 2). The absolute number of deaths from CVDs, though there were some fluctuations, decreased overall until 2009. After 2009, the number of CVD deaths increased until 2018; specifically, total heart diseases showed an increasing trend, whereas cerebrovascular diseases showed a decreasing trend. The biggest contributor to the increase in deaths from total heart diseases was heart failure.
Mortality from all diseases of circulatory system
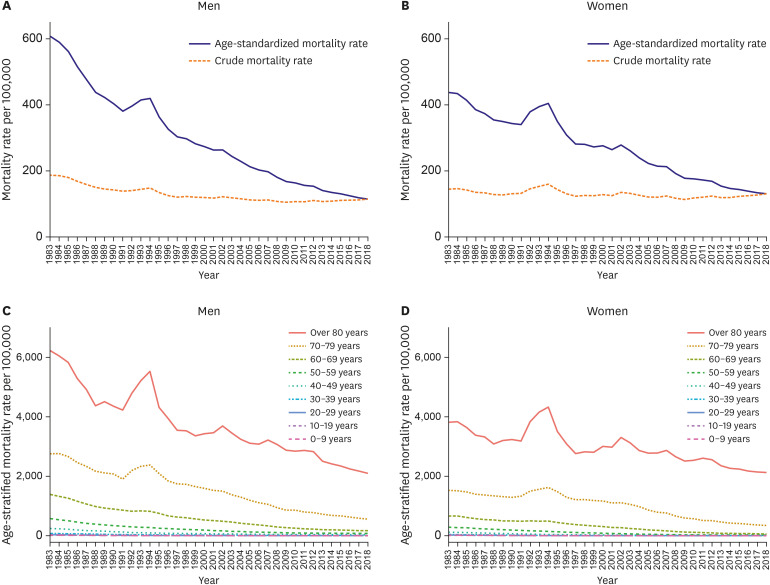
Although there were small changes in the crude mortality rate for all diseases of circulatory system in both sexes over the last 36 years, there has been a slight increase in both sex over the recent 5 years (Figure 2). In 2013, the crude mortality rate for all diseases of circulatory system was 107.2 per 100,000 in men and 119.0 per 100,000 women. By 2018, the rate has increased to 114.6 per 100,000 men and 130.8 per 100,000 women (Supplementary Tables 3 and 4). In both sex, the age-standardized mortality rate has decreased, except in the early 1990s (Supplementary Tables 5 and 6). The age-stratified mortality rate has also decreased in all age groups, except in the early 1990s (Figure 2, Supplementary Tables 7 and 8).
Mortality from heart diseases and cerebrovascular diseases
The age-standardized mortality rate for total heart diseases consistently decreased in both sexes. In 1983, the age-standardized mortality rate per 100,000 was 337.6 in men and 229.8 in women. In 2018, the age-standardized mortality rate per 100,000 was 68.2 in men and 80.8 in women. This translates to a 79.8% decrease in men and a 64.8% decrease in women over the 36-year period. The crude mortality rate for total heart diseases decreased until early 2000s; thereafter, it showed a slight upward trend, showing a U-shaped curve. The crude mortality rate for total heart diseases in 1983 was 110.2 per 100,000 in men and 80.1 per 100,000 in women. By 2018, the crude mortality rate per 100,000 was 68.2 in men and 80.8 in women (Figure 3, Supplementary Figure 2, Supplementary Tables 9 and 10).
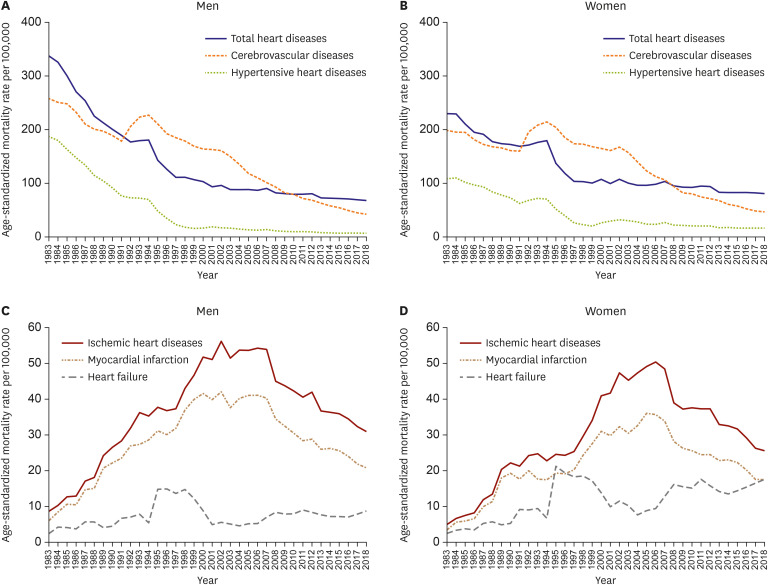
The age-standardized mortality rate for hypertensive heart diseases has rapidly decreased until the late 1990s and stabilized thereafter. The age-standardized rate showed a 96.2% decrease in men and a 84.8% decrease in women over the 36-year period. The crude mortality rate for hypertensive heart diseases showed a downward trend until the early 2000s in both sexes; it has stabilized thereafter in men but slightly increased in women (Figure 3, Supplementary Figure 3, Supplementary Tables 11 and 12).
The age-standardized and crude mortality rate trends for ischemic heart diseases and myocardial infarction were alike. Based on the number of deaths, deaths from myocardial infarction account for about 66–88% of deaths from ischemic heart diseases each year. The age-standardized mortality rate for ischemic heart diseases increased rapidly until the early 2000s and gradually decreased thereafter in both sexes. In 1983, the age-standardized mortality rate for ischemic heart diseases per 100,000 was 8.7 in men and 5.0 in women. In 2018, the age-standardized mortality rate per 100,000 was 30.9 in men and 25.6 in women. The age-standardized mortality rate showed a 257.3% increase in men and a 413.9% increase in women. The crude mortality rate for ischemic heart diseases rapidly increased until the mid-2000s and fluctuated thereafter in both sexes. The age-standardized mortality rate for myocardial infarction showed a 245.2% increase in men and a 409.0% increase in women over the 36-year period. The crude mortality rate for myocardial infarction showed an 899.0% increase in men and a 1,425.9% increase in women (Figure 3, Supplementary Figures 4 and 5, Supplementary Tables 13-16).
The age-standardized mortality rate for cerebrovascular diseases decreased until recently. Over the 36-year period, it showed a 83.5% decrease in men and a 76.5% decrease in women. The crude mortality rate for cerebrovascular diseases fluctuated until 2002 and decreased afterwards. (Figure 3, Supplementary Figure 6, Supplementary Tables 19 and 20).
Mortality from heart failure
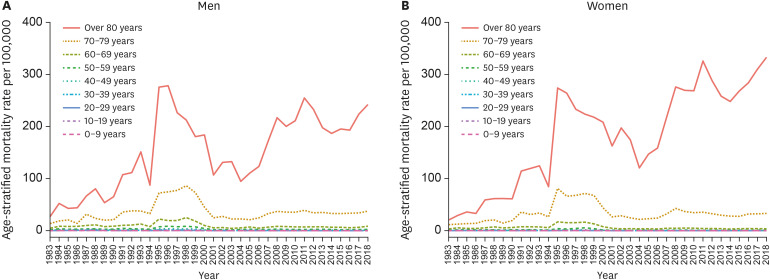
There was a significant increase in heart failure mortality over the 36-year period. Except in the late 1990s, the age-standardized mortality rapidly increased, especially in women. The mortality rate soared in 1994 and sharply declined in 2001. The age-standardized mortality rate showed a 261.7% increase in men and a 608.1% increase in women. The rate of increase has accelerated in the recent years, largely owing to the age group above 80 years. In 1983, the age-stratified mortality rate of the age group above 80 years was 26.9 per 100,000 in men and 20.5 per 100,000 in women. In 2018, the rate increased up to 242.2 per 100,000 in men and 332.9 per 100,000 in women. Likewise, the crude mortality rate followed similar trend over the 36-year period (Figures 3 and 4, Supplementary Tables 17 and 18).
Male to female ratio of age-standardized mortality rate from cardiovascular diseases
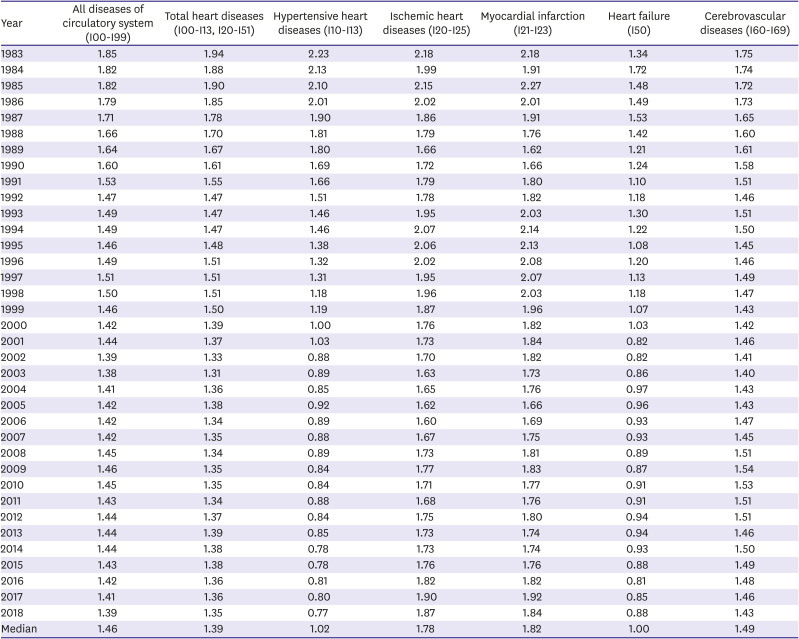
In all diseases of circulatory system, the male to female ratio (M/F ratio) has decreased over the 36-year period but did not fall below 1.00. Age-standardized total heart disease mortality rate was approximately 40% higher in men: the median (minimum to maximum) M/F ratio was 1.39 (1.31 to 1.94). Ischemic heart disease (1.78 [1.60 to 2.18]) and myocardial infarction (1.82 [1.62 to 2.27]) showed much higher M/F ratio. On the contrary, hypertensive heart disease (1.02 [0.77 to 2.23]) and heart failure (1.00 [0.81 to 1.72]) mortality rates were similar for both sexes (Table 1).
Table 1
Male to female ratio of age-standardized mortality rate from cardiovascular diseases
DISCUSSION
Our study reports the mortality rates and trends for major CVDs in Korean population over a 36-year period from 1983 to 2018. The absolute number of deaths and crude mortality rate from all diseases of circulatory system have been on the rise in the last 10 years, largely due to increasing trend in ischemic heart diseases and heart failure. In contrast, the number of deaths and crude mortality rate from cerebrovascular diseases are decreasing. However, age-standardized and age-stratified mortality rates markedly declined for all diseases of circulatory system, total heart diseases, hypertensive heart diseases, and cerebrovascular diseases between 1983 and 2018; although there were brief increases in early 2000s, possibly due to changes in the classification of the Cause of Death Statistics in Korea. Age-standardized mortality rates for ischemic heart diseases and myocardial infarction peaked in the early 2000s and decreased thereafter. Exceptionally, heart failure showed rapid increases in the number of deaths, crude mortality, and age-standardized mortality rates.
The decreasing trends in CVD mortality can be largely attributed to better prevention and management of risk factors.7)8)9)10)11)12) A recent nationwide study reported that the prevalence of low high-density lipoprotein cholesterol, smoking, and high risk drinking significantly decreased between 2007 and 2015.13)14) The prevalence of obesity, which is an important risk factor for hypertension, dyslipidemia, and diabetes, has increased in Korean adults, especially in men.13) But, at the same time, the management of hypertension, dyslipidemia, and diabetes has greatly improved.15)16)17)18) Major pharmacological and technological advances in acute and long-term CVD management may also have fueled such improvements.1) Improvement in the surgical outcomes of heart diseases in Korea also contributed to the decreasing trends both in children and adult CVD mortality.19)
In our study, the decreasing CVD mortality was most evident for deaths from hypertensive heart diseases. As the prevalence of hypertension did not change significantly, the decrease in hypertension-related mortality may be partially attributed to improved management of hypertension. Alternatively, poor standardization in the previous Korean Standard Classification of Diseases (KCD) coding may also have affected such results.20)21)22) Many deaths from undiagnosed cerebrovascular disease or acute myocardial infarction would have been classified as hypertension-related mortality in the 1980s before the widespread use of computed tomography and coronary angiography. Indeed, age-standardized mortality rates for ischemic heart disease and myocardial infarction increased simultaneously with the decline of hypertension-related mortality until the mid-2000s.
The increasing trend of heart failure mortality deserves attention. Even aside from a temporary spike between 1994–2001 possibly due to changes in the cause of death classification, a continuous upward trend prevailed and appeared more evident in the elderly population. As mortality rates decline for ischemic heart diseases and myocardial infarction, survivors may progress to heart failure, given that ischemic heart disease is its leading cause.23) In the Korean Heart Failure study, the prevalence of heart failure increased approximately two times (from 0.75% in 2002 to 1.53% in 2013), while the prevalence in aged 80 years or older was approximately 8-times higher than its overall prevalence.23) Similarly, among other types of heart diseases (I26-I51), conduction disorders and cardiac arrhythmias (I44-I49) showed a steep rise. As both heart failure and arrhythmia are common sequelae of other heart diseases, greater life expectancy may naturally accompany increased disease burden from heart failure and arrhythmia.24)25)
While the mortality rate of cardiovascular disease other than heart failure is rapidly decreasing in middle-aged and older adults, the CVD mortality rate was not decreasing recently among younger adults under the age of 40. Current CVD prevention guidelines can disproportionately underestimate the risk in the younger population, thereby undermining primordial prevention effects.26) Although young adults may have relatively low absolute risk of CVD than older people and less immediate health concerns, the lifetime cumulative effect of improving health behavior and risk factors can be much greater in younger ages.27)28)
As indicated by the male to female mortality ratios, almost all diseases of circulatory system mortality rates were higher in men than in women, except for hypertensive heart diseases and heart failure. In particular, we observed a steeper heart failure mortality increase in women than in men, especially above age 80 years. This is in line with a higher prevalence of heart failure in women than in men.23) Sex discrepancy is also plausible as the omission of heart failure diagnostic codes for ischemic heart diseases is more common in men than in women. Also for hypertension, the prevalence in women is higher than that in men above age 70 years.17) Likewise, such finding is plausible as women have much higher age distribution than men, even within the very old age group.29)
In the Global Burden of Disease study, declines in the age-standardized CVD mortality rate occurred between 1990 and 2015 in all high-income countries and some middle-income countries.30) But, age-standardized CVD mortality shows less decline in the past 5 years than over the past 25 years. This stagnation in declining CVD mortality was also shown in our study. In Korea, comparing the 2013–2018 period to the 2007–2012 period shows that the trend of mortality reduction has slowed recently. Stagnation in declining CVD mortality and rise in the absolute number of CVD deaths demonstrate the importance of continuous monitoring and increased investment in prevention and treatment of CVD to reduce health burden.
The major strength of the present study is its sex- and age-specific analyses of nationwide mortality data over a 36-year period. Furthermore, we produced both crude and age-standardized mortality rates of overall and CVD subtypes, in attempt to illustrate temporal trend as well as to elucidate causes behind such changes. However, several limitations needed to be discussed. First, the cause of death is subjected to misclassification from changes in KCD coding and temporal difference in diagnostic accuracy. A previous study examined the accuracy of death statistics, and reported that the overall accuracy rate of statistics about the causes of death was 91.9%.20) Moreover, from 1983 to 2018, the KCD was revised 5 times. Until 1994, the KCD was based on the International Classification of Diseases, 9th Revision (ICD-9); since then, the KCD was updated to the 3rd revision which was based on ICD-10. Thus, there has been a major change in the coding system, which could have affected the mortality rate of diseases. Second, the Causes of Death Statistics included deaths with an unknown age. These deaths were included in the crude mortality rate but were excluded from the age-standardized and age-stratified mortality rates. Hence, the number of deaths based on crude and age-standardized mortality rates are different.
In conclusion, CVD mortality in Korea has significantly decreased over the 36-year period. However, the recent rise in the absolute number of cardiovascular deaths, especially from heart failure, calls for attention in prevention and management of CVD. The trends in mortality from CVDs need to be continuously monitored to reduce health burden.
 XML Download
XML Download