

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Delirium is characterized by symptoms such as fluctuating cognition, disorientation, confusion, and hallucinations. It is well-documented that delirium is associated with extended hospital stays, increased medical expenses, and elevated mortality rates in patients with various ailments.1 Since the outbreak of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), there have been numerous reports of delirium among COVID-19 patients.2 Several pathophysiological mechanisms have been proposed to explain the relationship between delirium and SARS-CoV-2. COVID-19 infection tends to exacerbate the neuroinflammatory response, which may lead to encephalopathy34 and subsequently delirium. Additionally, glucose hypometabolism in the cerebral cortex has been suggested as a potential contributing factor to delirium in COVID-19 patients.5 Social isolation due to limited physical contact and restrictions on family visits during the pandemic might also be contributing factors.4 A recent meta-analysis has established a significant link between delirium and mortality among COVID-19 patients.2 Additionally, delirium is associated with poor outcomes in COVID-19 patients, such as respiratory distress, reduced oxygen saturation, critical complications, and admission to the intensive care unit.6
Given the clinical significance of delirium, ongoing research seeks to identify risk factors to facilitate its prevention. Delirium can be attributed to various factors depending on the clinical setting; generally recognized risk factors include older age, cognitive impairment, frailty, medical comorbidities, psychiatric illness, alcohol use, malnutrition, sensory impairment, trauma, surgery, dehydration, drug use, and medication changes.7 Recent studies focusing on delirium in COVID-19 patients have identified risk factors such as advanced age, smoking, alcohol abuse, mechanical ventilation, and the use of certain medications like antipsychotics, benzodiazepines, and opioids.8 While strategies such as increasing engagement with elderly patients have been suggested as countermeasures for delirium,9 many of these risk factors are challenging to modify directly in clinical settings.10 Given the isolation requirements for COVID-19 patients, modifiable factors are even more limited, making medication adjustment one of the most feasible strategies. There have been reports on the effects of medications that either induce or alleviate delirium,11 but the association between psychotropic medications and delirium, a condition characterized by global brain dysfunction and various psychiatric symptoms, remains unclear. Psychotropic medications are commonly prescribed among the general population, particularly in the elderly.12 However, recent studies have reported a prevalence of potentially inappropriate psychotropic prescriptions of 10.73%, often accompanied by polypharmacy.13 Moreover, it has been reported that there are significant drug-drug interactions between several psychotropic medications and antiviral agents used for the treatment of COVID-19.14
In this context, this study aimed to explore the relationship between delirium in COVID-19 patients and the use of psychotropic medications. While previous studies have often associated benzodiazepines with an increased risk of delirium,15 a recent systematic review suggests that anticholinergics increase the risk of delirium, whereas benzodiazepines, antidepressants, and antipsychotics do not have a significant impact.16 It is also recognized that cholinergic deficiency not only contributes to the pathogenesis of delirium but is also associated with neurocognitive disorders such as dementia.7 Recent randomized controlled trials (RCTs) have explored the therapeutic or preventive effects of acetylcholinesterase inhibitors, commonly used for neurocognitive disorders, on delirium.171819 While the results from these studies are mixed, indicating a lack of conclusive evidence on their effectiveness, they underscore the need for further research. Accordingly, our study aimed to further investigate the association between cholinergic medication and the incidence of delirium, particularly in the context of COVID-19, where the impact of such medications may differ. Moreover, most studies have focused on critically ill patients, and there is limited research on other medications such as antidepressants or mood stabilizers.20 Consequently, it is imperative to validate the efficacy of psychotropic medications in a general inpatient setting by analyzing nationwide cohort data to establish the temporal relationships between drug prescriptions and the diagnoses of delirium and COVID-19. Analyzing these relationships specifically in COVID-19 patients could yield valuable insights for delirium interventions.
In this study, we aimed to ascertain the long-term relationship between COVID-19, delirium, and mortality, utilizing a nationwide dataset. Furthermore, our objective was to explore the risk factors for delirium occurrence among COVID-19 patients. It is well-established that COVID-19 and delirium are risk factors for mortality. However, most studies have only explored short-term mortality2 or have omitted delirium from their models,2122 thus failing to concurrently examine the influence of delirium and COVID-19 on long-term mortality. Therefore, in Study 1, we used 1-year mortality as the dependent variable and included both delirium and COVID-19 as independent variables to ascertain whether these variables are risk factors for long-term mortality. For this purpose, Study 1 consisted of a group of COVID-19 patients and a propensity score (PS)-matched control group. In Study 2, we aimed to identify the factors contributing to delirium in COVID-19 patients. Specifically, our goal was to integrate psychotropic medication into the model to assess its role in the occurrence of delirium among individuals with COVID-19. Furthermore, we conducted subgroup analysis on the risk factors for delirium to elucidate how various risk factors, particularly psychotropic medication, operate within different age groups.
METHODS
Design and participants
The NHIS in South Korea is the sole provider of mandatory health insurance for the entire Korean population, maintaining a nationwide health database that records all diagnoses and drug prescriptions. The NHIS collaborated with the Korea Disease Control and Prevention Agency to provide medical data on COVID-19 patients who tested positive through polymerase chain reaction tests for research objectives. An independent technician extracted the data used in this research.
We recruited adults (aged ≥ 19 years) diagnosed with COVID-19 between October 2020 and December 2021. The control group in Study 1 comprised randomly selected adults without COVID-19 during the same period (15 times the COVID-19 patients). Subsequently, 1:1 PS matching was conducted. Study 2 only involved COVID-19 patients, where the non-delirium group was formed through 1:38 matching with the delirium group.
Procedures
In Study 1, the index date for COVID-19 patients was their first COVID-19 diagnosis, while for the control group, it was the date of their first hospital visit during the study period. The control group was created through 1:1 PS matching with the patient group. The primary outcome was 1-year all-cause mortality, measured from the index date to the date of death or March 2022. Study 1 assessed the effects of delirium and COVID-19 on mortality. In Study 2, the primary outcome was delirium incidence (identified by International Classification of Diseases 10th Revision [ICD-10] code F05) within 3 months among COVID-19 patients. A 1-month washout period was set for patients with a history of delirium before the index date. As a nested case-control study, the non-delirium group was constructed through exact matching with the delirium group. Study 2 aimed to identify delirium risk factors among COVID-19 patients. Subgroup analyses by age (< 60 vs. ≥ 60 years) were conducted in Study 2. Supplementary Fig. 1 provides a visual representation of all procedures.
Demographic and clinical variables
Potential confounders included demographic characteristics (age, sex) and socioeconomic factors such as insurance type (health insurance, medical aid), area of residence (Seoul, metropolitan cities, rural areas), and the Charlson Comorbidity Index (CCI; computed using ICD-10 codes assigned within 1 year before the index date). In Study 2, additional variables considered were psychotropic medication prescriptions (antipsychotics, antidepressants, mood stabilizers, benzodiazepines, cholinergic medications), COVID-19 treatment duration (in days), and history of delirium (ICD-10 code F05 assigned within 1 year before the index date). A longitudinal study design examined medication patterns from a predetermined index date, with a 3-month follow-up or until delirium onset. Antipsychotics, frequently used for delirium symptomatic management, were not part of the baseline medication regimen if patients who had no history of antipsychotic use started using them within 2 weeks prior to the onset of delirium. This approach was taken to mitigate the potential confounding effect of initiating antipsychotics in response to or in anticipation of emerging symptoms of delirium. In the additional model, diseases covered by the CCI that had an incidence rate of > 5% and are known to be associated with delirium were individually identified. Detailed medication lists are in Supplementary Table 1.
Statistical analysis
Demographic data were analyzed using Pearson’s χ2 test for categorical variables and t-test for continuous variables. In Study 1, a control group was established through PS matching, utilizing logistic regression analysis for PS computation. The greedy nearest neighbor algorithm was applied with caliper widths set at 0.1 times the pooled standard deviation of the logit of the PS. Matching was performed on a 1:1 basis with the COVID-19 patient group, considering sex and age. To control for immortal time bias, a time-dependent Cox model was utilized, incorporating delirium as a time-dependent covariate. All time frames preceding the initial diagnosis of delirium were coded as 0, while those following the first diagnosis were coded as 1. The extended Kaplan-Meier estimator compared mortality rates between COVID-19 patients and a controls, as well as delirium and non-delirium groups. The log-rank test compared survival curves. A multivariable Cox regression analysis assessed whether COVID-19 and delirium were independent risk factors for mortality while controlling for demographic variables.
In Study 2, which included only COVID-19 patients, the non-delirium group was 1:38 matched with the delirium group based on sex and age using the PROC SURVEYSELECT procedure of SAS software (version 7.1; SAS Institute, Cary, NC, USA). Random sampling was performed with stratification by age (in 5-year increments) and sex to achieve exact matching of their distributions. In our dataset, the prevalence of delirium was significantly lower than that of the non-delirium population. To address this imbalance and ensure a robust statistical comparison, we determined that the maximum feasible extractable ratio of non-delirium to delirium cases was 38 to 1. Consequently, we implemented a matching ratio of 1:38 based on sex and age. This approach was designed to maximize the sample size for the control group while maintaining the representativeness of both groups. Multivariable logistic regression analysis calculated delirium incidence within 3 months of the index date among COVID-19 patients, identifying risk factors for delirium. A subgroup analysis by age group was performed using the same regression model.
Cox regression models result as hazard ratios with 95% confidence intervals (CIs), and logistic regression outcomes as odds ratios with 95% CIs are reported. The variance inflation factor (VIF) was calculated to check for collinearity, and no collinearity was detected (VIF < 2.0).
All analyses were conducted using R (version 3.6.2; R Project for Statistical Computing, Vienna, Austria) and SAS (version 7.1; SAS Institute) software. P values < 0.05 were deemed statistically significant.
Ethics statement
This study followed the Reporting of Observational Studies in Epidemiology guidelines, and obtained approval from the Institutional Review Board of Seoul National University Bundang Hospital (approval No. X-2109-711-903) as well as the Health Insurance Review and Assessment Service (approval No. KDCA-NHIS-2022-1-630). Informed consent requirements were waived by both committees, as all personal data were anonymized by the South Korean National Health Insurance Service (NHIS).
RESULTS
Study population
Table 1 presents the baseline characteristics of the study cohort following matching. The mortality rate was higher in the COVID-19 patient group. Notably, the incidence of delirium was 0.09% in the control group compared to 0.23% in the COVID-19 patient group. There were significant differences in all demographic variables, and the rates of all comorbidities were higher among COVID-19 patients. COVID-19 patients with delirium showed demographic differences, including variations in CCI, compared to those without delirium. Moreover, the delirium group contained higher proportions of patients with cerebrovascular disease, congestive heart failure, dementia, diabetes, metastatic solid tumors, hemiplegia, peripheral vascular disease, and renal disease. Except for antipsychotics, the rates of psychotropic medication usage were higher among patients with delirium.
Table 1
Demographic differences between COVID-19 group and control group and between COVID-19 patients with delirium group and COVID-19 patients without delirium group
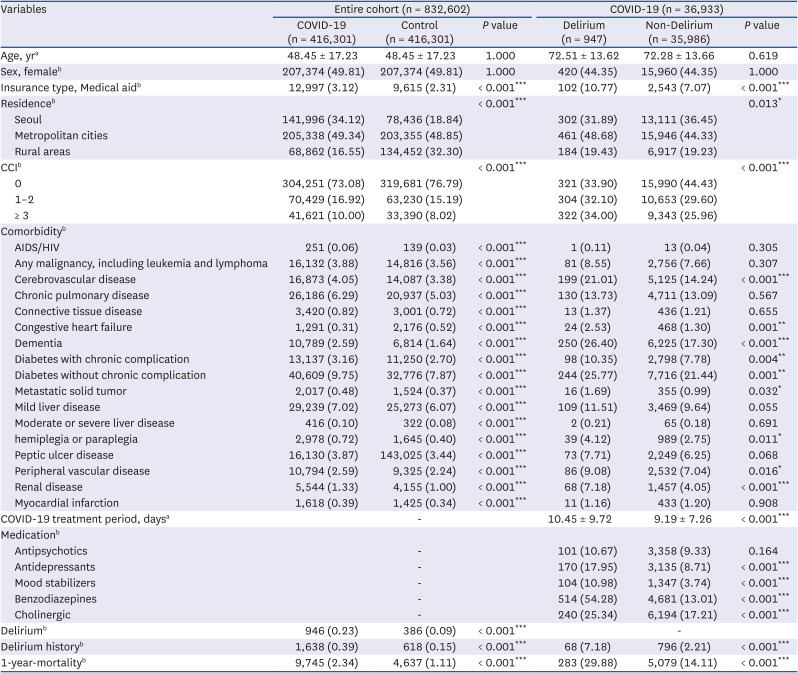
Medication usage data covered from the index date to either after 3 months or to the date of delirium incidence.
COVID-19 = coronavirus disease 2019, CCI = Charlson Comorbidity Index, AIDS = acquired immuno-deficiency syndrome, HIV = human immunodeficiency virus.
aData given as mean ± standard deviation.
bData given as number (%).
*P < 0.05, **P < 0.01, ***P < 0.001.
Study 1: one-year all-cause mortality
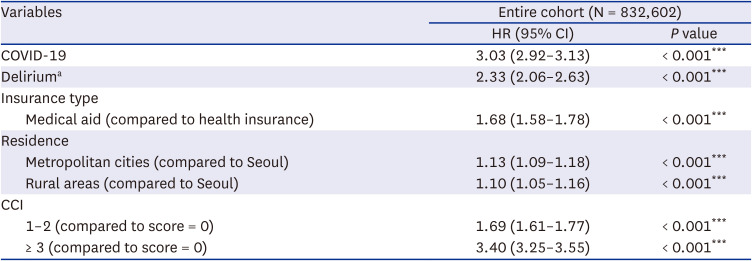
An analysis of the extended Kaplan-Meier curve indicated that the mortality rate among COVID-19 patients was significantly higher than that of the control group (Fig. 1A). Additionally, the mortality rate was higher among patients with delirium compared to those without delirium (Fig. 1B). In the entire study population, both COVID-19 and delirium were associated with an elevated risk of 1-year all-cause mortality after controlling for all demographic variables (Table 2). Specifically, patients with COVID-19 exhibited a 3.03-fold higher risk of death compared to non-COVID-19 patients, while patients with delirium had a 2.33-fold higher risk of death than those without delirium. The type of insurance, residing outside Seoul, and the CCI were also identified as independent predictors of mortality. All comorbidities, with the exception of peripheral vascular disease, mild liver disease, and AIDS/HIV, were risk factors for mortality (Supplementary Table 2).
Fig. 1
Extended Kaplan–Meier curves between COVID-19 patients and the control group (A), as well as between patients with delirium and those without delirium (B) in study 1.
COVID-19 = coronavirus disease 2019.
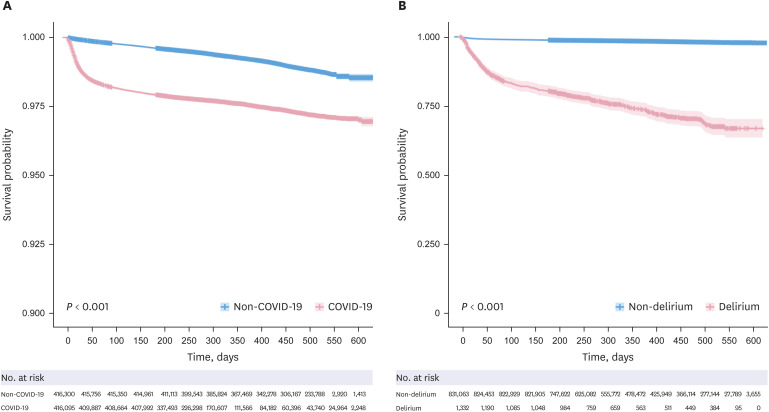
Table 2
Time-dependent Cox regression results for 1-year all-cause mortality of entire cohort (study 1)
Study 2: development of delirium in COVID-19 patients
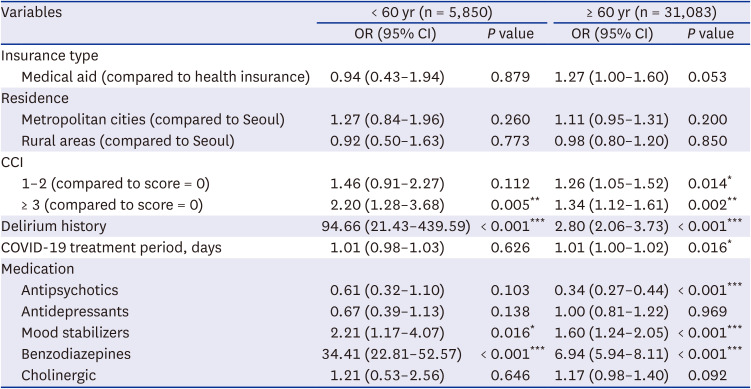
Table 3 identifies factors that elevated the incidence of delirium in COVID-19 patients. Multivariable logistic regression revealed that the type of insurance, CCI score, duration of COVID-19 treatment, and a history of delirium were risk factors for the development of delirium. In particular, mood stabilizers and benzodiazepines were associated with an increased incidence of delirium, while antipsychotics were linked to a lower incidence. Additionally, underlying diseases that increased the risk of delirium included renal disease, cerebrovascular disease, and dementia (Supplementary Table 3). Subgroup analysis was performed based on age, and the results are presented in Table 4. Both mood stabilizers and benzodiazepines emerged as risk factors for delirium in patients aged < 60 and ≥ 60 years. However, the use of antipsychotics was associated with a reduced incidence of delirium only in patients aged ≥ 60 years.
Table 3
Multivariable logistic regression results on the incidence of delirium in COVID-19 patients (study 2)
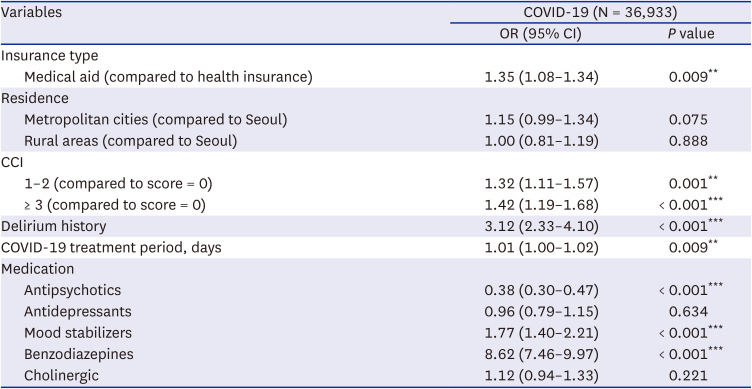
Table 4
Subgroup analysis of delirium incidence in COVID-19 patients by age
DISCUSSION
In this study, we investigated the effects of COVID-19 infection and delirium on long-term mortality using a nationwide cohort dataset. Our findings confirm that both COVID-19 infection and delirium serve as independent risk factors for 1-year all-cause mortality. Previous studies have examined 1-year mortality rates among COVID-19 patients and analyzed factors influencing these rates.23 Uniquely, our study not only established that COVID-19 infection independently increases overall mortality, but also explored the factors affecting this increase through PS matching by comparing individuals infected with COVID-19 to an uninfected control group. Furthermore, while most preceding studies primarily focused on the direct impact of COVID-19 on mortality, such as short-term mortality, our study investigated the indirect, relatively long-term mortality (> 1 year). As the phenomenon of “long COVID,” or post-acute sequelae of SARS-CoV-2 infection (PASC; persistent symptoms following a COVID-19 infection), is increasingly being acknowledged,24 it is imperative to consider the long-term indirect consequences of COVID-19 infection. Moreover, we highlighted that delirium independently contributes to long-term mortality, corroborating findings from earlier studies.25 Delirium has been linked to both internal and external medical complications, such as patients removing medical devices or engaging in violent behavior, and the use of sedatives might cause additional issues, potentially delaying recovery and impacting mortality.25 Our study also found that insurance type and area of residence, both proxies for socioeconomic status, were associated with mortality, suggesting that disparities in access to medical services might influence mortality rates. In terms of comorbidities, the CCI encompasses diabetes, hypertension, and renal, respiratory, and cardiac disorders, which have previously been identified as risk factors for overall mortality.26
Our findings suggest a higher delirium incidence and increased mortality in COVID-19 patients compared to non-COVID-19 individuals (Table 1), supporting a potential association between COVID-19 and delirium. The incidence of delirium among COVID-19 patients was 0.23%, lower than that reported in earlier studies,27 which might be attributed to the composition of our study population. Throughout the pandemic, all individuals testing positive for COVID-19 were mandated to be admitted to isolation units in medical centers, regardless of symptom severity. As such, the nationwide data encompassed patients with mild symptoms. A recent meta-analysis reported that COVID-19 patients with delirium exhibited higher all-cause mortality than those without delirium.27 Another study revealed that the occurrence of delirium during hospitalization led to increased 8-month mortality in COVID-19 patients,28 emphasizing the importance of delirium prevention in this population. Previous studies identified risk factors for delirium in COVID-19 patients, including older age, male gender, area of residence, and prolonged COVID-19 treatment duration.8 In this context, the impact of pre-infection medications becomes paramount.
Among psychotropic medications, antipsychotics were linked to reduced delirium incidence in COVID-19 in our study. Antipsychotics are frequently employed to manage delirium symptoms, and some RCTs have suggested their potential in reducing the risk of delirium, though findings have been inconsistent.29 Notably, our study associates antipsychotic use with a lower incidence of delirium, even after excluding cases where antipsychotics were used to manage symptoms of delirium. While the mechanism by which antipsychotics may reduce delirium in COVID-19 patients remains unclear, several hypotheses can be proposed based on our findings and recent reviews. Firstly, antipsychotics could ameliorate symptoms such as anxiety and confusion, which are often precursors to delirium, potentially decreasing its incidence among COVID-19 patients.3 This aligns with observations from the systematic review,30 which suggests that antipsychotics may improve delirium outcomes. Furthermore, it is plausible that the severity of the central nervous system infection induced by COVID-19 could be mitigated by the administration of antipsychotics.31 Additionally, other research has postulated benefits of some antipsychotics despite the risk of drug-drug interactions.32 Although direct confirmation of these interactions is challenging in our study, the evidence suggests that discontinuing antipsychotics during COVID-19 infection could potentially increase delirium risk, underscoring the need for cautious management of antipsychotic therapy in these patients. Our examination of COVID-19 patients uncovered a possible association between antipsychotics and reduced delirium, underscoring the need for further investigation of this relationship in the context of COVID-19-associated delirium. In contrast, benzodiazepines have consistently been shown to elevate the risk of delirium.33 This is attributed to their high affinity for gamma-aminobutyric acid receptors in the central nervous system, possibly inducing delirium through alterations in neurotransmitter levels.34 Additionally, we sought to explore the relationship between mood stabilizers and delirium, which is less well-established in the existing literature. While limited research is available on this topic, some studies suggest that gabapentin, which shares mechanisms with other mood stabilizers, might heighten the risk of delirium.35 Although certain studies advocate the use of valproate to manage specific delirium symptoms,36 our study suggests that baseline use of valproate mood stabilizers could increase the risk of delirium, impacting not just the elderly but also patients < 60 years old. Meanwhile, antidepressants and cholinergic medications did not display significant associations. These insights emphasize the need to carefully adjust pre-existing medications, particularly psychotropics commonly used in polypharmacy, in strategies to prevent delirium in acutely infected patients. Further research, including RCTs, is necessary to determine whether adjustments in medication regimens produce tangible preventive benefits.
Subgroup analysis by age revealed that antipsychotics significantly decreased the incidence of delirium only in individuals aged ≥ 60 years. This suggests that aging affects neurotransmitter systems and neural circuits, making older individuals more susceptible to neurotransmitter imbalances, possibly associated to delirium onset.37 Antipsychotics, through modulating the balance of neurotransmitters in the central nervous system, might be more efficacious in preventing delirium among the elderly.38 Previous studies have demonstrated that antipsychotics exert a prophylactic effect in elderly patients with delirium,39 but further investigation is warranted.
Our study is not without limitations. First, within the scope of the exploratory analysis of variables linked to mortality and delirium, the control group was matched based solely on age and sex. Second, NHIS data lacks specific delirium assessment tools like CAM, leading to potential underestimations of mild cases such as subsyndromal or hypoactive delirium. However, using ICD codes for diagnosis shows high positive (94.3%) and negative (92.8%) predictive values, indicating reliable identification of clear-cut cases.40 Future studies should integrate comprehensive tools and multimodal approaches to enhance accuracy and interpretation. Third, the study design made it difficult to establish causality between psychotropic medications and delirium due to the strong correlation between psychiatric diagnoses and psychotropic prescriptions, complicating the isolation of medication effects from underlying conditions. Lastly, in addressing data imbalance in a dataset of 832,602 entries, we matched delirium and non-delirium patients using broad criteria like sex and age, but analyzed only 36,933 entries due to the low incidence of delirium. This extensive matching led to the exclusion of many samples, limiting the generalizability of our findings.
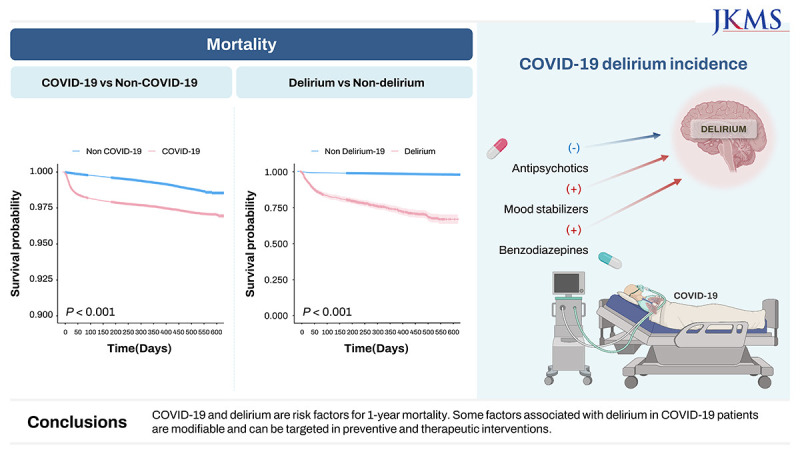
In summary, our study identified COVID-19 and delirium as independent risk factors for 1-year mortality. Delirium incidence among COVID-19 patients exceeded that in the control group. Medical aid insurance, high CCI, delirium history, and prolonged COVID-19 treatment were risk factors for delirium in COVID-19 patients. Antipsychotics correlated with a decreased delirium incidence, while mood stabilizers and benzodiazepines were associated with an increased incidence. Analyzing a nationwide cohort, our study establishes a connection among COVID-19, delirium, and long-term mortality, highlighting the impact of psychotropic medications on COVID-19-associated delirium. Evaluating their role provides insights for future preventive research and clinical guidelines in the context of COVID-19-related delirium.
 XML Download
XML Download