

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
There has been a steady trend toward axillary conservatism in patients with early-stage breast cancer. The surgical approach to the axilla has become less invasive, from complete axillary lymph node dissection (ALND) to sentinel lymph node biopsy (SLNB) to reduce potential morbidity.12 ALND has been the treatment of choice for patients with positive SLNB.3 However, clinical paradigms have been modified after the American College of Surgeons Oncology Group (ACOSOG) Z0011 trial,45 which found that SLNB without ALND did not compromise survival in patients with clinically T1-2 N0 breast cancers who underwent breast conserving therapy (BCT) if there were one or two nodal metastases at SLNB.45 The trial results raised question about the value of SLNB in clinically node-negative patients.6 Although SLNB had lower surgical morbidity compared to ALND, surgical complications still exist in patients with SLNB and omission of SLNB could leave out complications.24 Therefore, several randomized clinical trials such as SOUND (Sentinel Node versus Observation after Axillary Ultrasound),7 INSEMA (Intergroup-Sentinel-Mamma),8 and BOOG 2013-08 (Dutch randomized controlled multicenter trial) are currently underway to evaluate whether SLNB could be safely omitted in patients with T1-2 N0 breast cancers who have a negative axillary ultrasound (AUS) findings.68 As AUS was reported to have a high negative predictive value (NPV) of 84%, it has been suggested as a non-invasive alternative to SLNB.9
Given the evidence from the Z0011 trial, the role of breast magnetic resonance imaging (MRI) has also been challenged. Although breast MRI is controversial in early-stage breast cancer, MRI can depict potentially metastatic lymph nodes (LNs) in patients with negative AUS findings because it can provide objective and global views of the axilla irrespective of the patient’s body habitus and operator’s ability.10 Axillary MRI evaluation with a high NPV could result in omission of SLNB, whereas a high positive predictive value (PPV) could further guide ALND or neoadjuvant chemotherapy (NAC).11 Previous studies that retrospectively compared the diagnostic performance of MRI and ultrasound for depicting axillary LN metastasis showed that MRI had comparable performance to ultrasound.1213 However, there has been no published studies which evaluated the role of MRI in detecting additional LN metastases in patients with negative AUS.
For providing evidence for determining which patients can be included in the omission of SLNB, it is important to develop a reliable prediction model to predict axillary LN metastasis. Several nomograms have been developed for assessment of axillary burden.1415 However, these nomograms were mainly aimed at predicting non-sentinel LN metastasis in the presence of positive SLNB. Previous studies using ultrasound or MRI features of primary tumor reported that artificial intelligence might predict axillary LN metastasis.1617181920 However, advanced artificial intelligence is not widely applicable in clinical practice.
Therefore, this study aimed to evaluate the false negative result (FNR) and the rate of high nodal burden (HNB) in patients with clinically T1-2 N0 breast cancers who had negative AUS and assess the diagnostic performance of breast MRI and clinical-imaging nomogram for predicting axillary LN metastasis.
METHODS
Study designs and patients
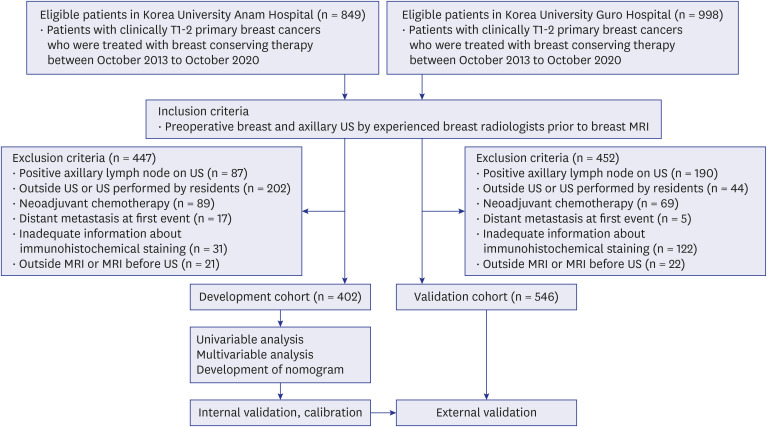
By retrospectively reviewing two tertiary medical centers’ database (October 2013 and October 2020), we identified 948 clinically T1-2 N0 patients who had negative AUS, subsequent breast MRI, and BCT. At first, a primary development set of 402 patients from Korea University Anam Hospital were retrospectively analyzed. Inclusion criteria were having preoperative breast and AUS by experienced breast radiologists prior to breast MRI and negative axillary result on ultrasound. Exclusion criteria were positive axillary result on ultrasound, ultrasound performed by an outside hospital/resident, NAC before operation, distant metastasis at diagnosis, inadequate information about immunohistochemical staining, and outside MRI. A validation set of 546 patients from Korea University Guro Hospital was further analyzed. The diagram for establishing the development and validation sets is summarized in Fig.1.
Breast and AUS examinations
To evaluate the clinical T and N stage, one of three breast radiologists (K.R.C., S.E.S., E.K.P., with 21,11, and 8 years of experience in breast imaging, respectively) in Korea University Anam Hospital and one of two breast radiologists (O.H.W. and H.S., with 19 and 7 years of experience) in Korea University Guro Hospital performed preoperative breast and AUS with a Logiq 9 unit (General Electric, Milwaukee, USA), and an Aixplorer system (SuperSonic Imagine, Aix en Provence, France) within a median of 14 and 12 days before surgery in the two sets. All cancers were assessed using the breast imaging reporting and data system (BI-RADS) categories 4A, 4B, 4C, and 5 (Fig. 2A). Axillary results on AUS were recorded as either negative or positive (Fig. 2B). Based on BI-RADS, positive axilla was considered when a LN with at least one of the following features was found: eccentric cortical thickening, diffuse cortical thickening of 3 mm or large, rounded hypoechoic, complete or partial effacement of the fatty hilum, and nonhilar cortical blood flow on color Doppler images.2123 If the assessment for axillary LN were equivocal or borderline, two breast radiologists (K.R.C., S.E.S. with 21 and 11 years of experience in breast imaging, respectively) re-evaluated the axillary LN status and categorized it into negative or positive by consensus. For obtaining clinical T stage, the longest tumor size on ultrasound was measured.
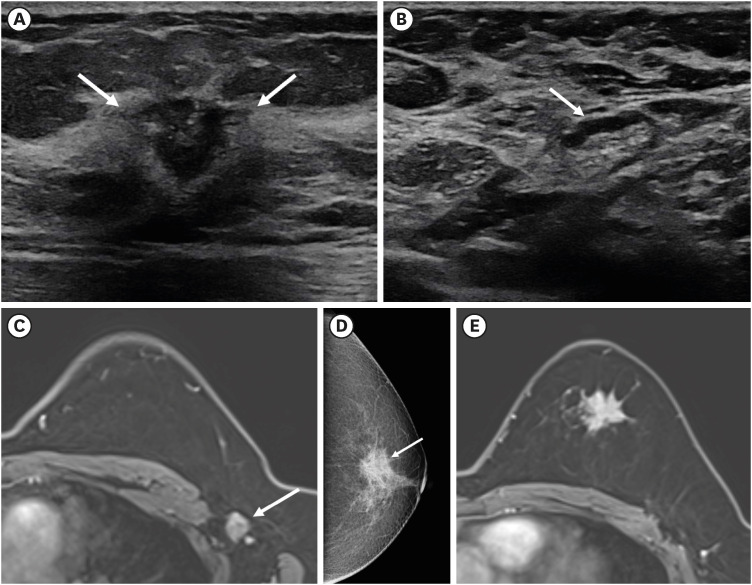
Fig. 2
Findings in a 53-year-old woman with clinically T1N0 breast cancer in her left breast. (A) Breast US shows a 1.3-cm mass with breast imaging reporting and data system category 5 assessment (arrows). (B) Axillary US shows a benign looking LN with an assement of negative axilla (arrows). (C) Axial T1-weighted postcontrast MRI covering entire axilla shows a suspicious metastatic LN (arrow) which was enlarged with cortical thickening, round shape, and a long axis to short axis ratio of less than two at level I of the left axilla. (D) Right craniocaudal view of mammography shows a mass without calcifications (arrow) in the outer breast. (E) Axial T1-weighted postcontrast MRI shows an irregular shaped and marginated, heterogeneously enhancing mass in her left breast.
US = ultrasound, LN = lymph node, MRI = magnetic resonance imaging.
Breast MRI examinations
Breast MRI examinations were performed using two 3.0T scanners (Achieva 3.0T TX; Philips Healthcare, Best, the Netherlands and MAGNETOM Skyra; Siemens Healthcare, Erlangen, Germany) in Korea University Anam Hospital and a 3.0T scanner (MAGNETOM Skyra; Siemens Healthcare) in Korea University Guro Hospital with a dedicated breast array coil in the axial orientation. All MRI scans were taken with the patients in a prone position. Detailed protocols were described in Supplementary Data 1.
One of three breast radiologists in Korea University Anam Hospital and one of two breast radiologists in Korea University Guro Hospital read breast MRI. Axillary MRI results were recorded as negative or positive (Fig. 2C). Positive axilla on MRI was considered when a LN with at least one of the following features was observed: markedly enlarged and morphologically grossly abnormal LNs, especially when they are distinctly different from other visible LNs, cortical irregularity or apparent spiculation, loss of fatty hilum, round shape, or a long axis to short axis ratio of less than two.2324 Axillary LN with equivocal or borderline assessment at radiologic report were re-evaluated in same way as breast ultrasound.
Image analysis
The mammographic and MRI features were retrospectively analyzed in a blinded manner without clinical information by two breast radiologists (K.R.C., S.E.S., with 21 and 11 years of experience in breast imaging, respectively) using the 2013 BI-RADS lexicon.25 Mammographic findings were evaluated with regard to the calcifications (presence vs. absence), and tumor location (outer vs. inner) (Fig. 2D). The shape, margin, density and echogenicity of tumors on mammography and ultrasound were not evaluated because we intended to use those findings from MRI. MRI features were evaluated in terms of mass shape (round to oval vs. irregular), mass margin (circumscribed or irregular vs. spiculated), mass internal enhancement (homogeneous or heterogeneous vs. rim), intratumoral high signal intensity and peritumoral edema on T2-weighted image (presence vs. absence) (Fig. 2E).
Data analysis
Clinical data (menopause, symptom, family history of breast cancer) were reviewed from the electronic medical records. Imaging data were obtained from radiology reports. Pathological data were acquired from histopathological reports of surgery. Pathologic data of primary breast cancer and LN metastasis were evaluated from surgical and pathologic reports. According to the eighth edition of the American Joint Committee on Cancer (AJCC) staging, pN1mi which means micrometastases (larger than 0.2 mm, but none larger than 2.0 mm) at LN was defined as pN1.21 At least one LN metastasis including pN1mi was considered as disease positive. In addition, HNB was defined as ≥ 3 positive LNs and low nodal burden was defined as 1–2 positive LNs according to the Z0011 trial.45 Estrogen receptor (ER) and progesterone receptor (PR) positivity were defined as the presence of positive staining in at least 1% of the nuclei in ten high-power fields. Human epidermal growth factor receptor 2 (HER2) negativity was defined as an immunohistochemical score of 1+ or 2+ staining with negative HER2 gene amplification on fluorescence in situ hybridization. Histologic type was categorized as ductal or other, and histologic grade was categorized as low (grade 1 or 2) or high (grade 3). Molecular subtypes were categorized as luminal (ER and/or PR-positive and HER2-negative), HER2-enriched (ER/PR-positive or negative, HER2-positive), or triple-negative (ER-negative, PR-negative, and HER2-negative).22 The Ki-67 proliferation index was dichotomized as low (< 14%) or high (≥ 14%).22
Statistical analysis
Baseline characteristics were compared using the Mann-Whitney U test, independent t-test, or independent χ2 test. The diagnostic performance of breast MRI and nomogram was assessed using sensitivity, specificity, PPV, and NPV. Logistic regression analysis was performed to identify clinical and imaging factors associated with axillary LN metastasis. For multivariable analysis, covariates with P values < 0.05 in the univariable analysis with forward elimination were used. Based on the adjusted odds ratio (OR) from multivariate analysis, clinical-imaging model was constructed and the nomogram was developed to visualize the results of the predictive model. Internal and external validation of nomogram was performed in development and validation sets. For validation, discrimination and calibration were assessed using area under the curve (AUC) and calibration slope. All statistical analyses were performed by using SPSS for Windows (version 20.0; IBM Corp., Armonk, NY, USA) and open-source R software (version 3.5.1; R Foundation for Statistical Computing, R Foundation, Vienna, Austria).
RESULTS
Characteristics of the sets
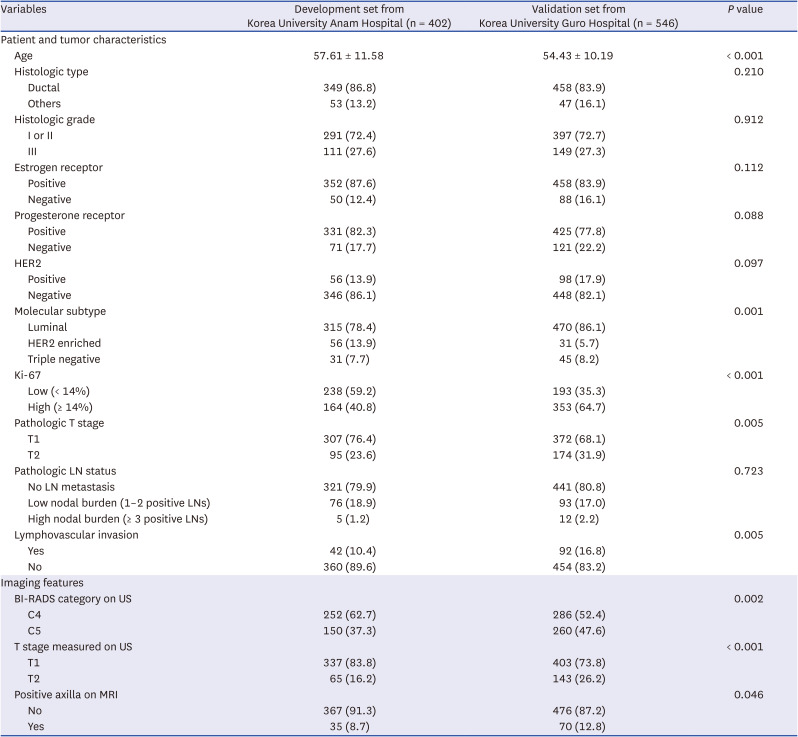
A total of 948 consecutive female patients were included (mean age ± standard deviation, 55.8 ± 10.9; range, 28–87 years) with 402 female patients (57.61 ± 11.58) in the development set and 546 patients (54.43 ± 10.02) in the validation set. A comparison of characteristics between the two sets is listed in Table 1. Compared to the development set, the validation set was composed of younger patients, pathologic T2 stage, lymphovascular invasion, luminal subtype, higher Ki-67, BI-RADS 5 assessment category on US, and positive axilla on MRI (all P < 0.05).
Table 1
Patient and tumor characteristics in two medical centers
FNRs of AUS
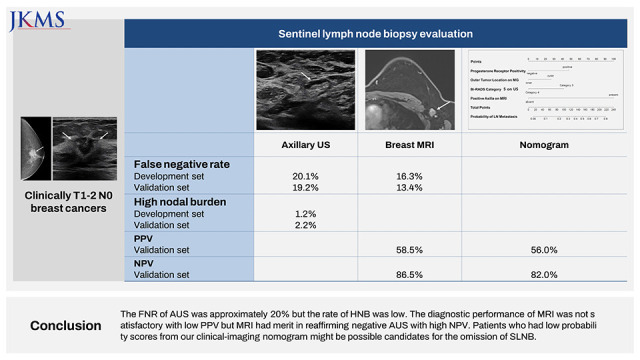
The FNRs of AUS were 20.1% (81 of 402 patients) within development set and 19.2% (105 of 546 patients) within validation set. The rates of HNB were 1.2% (5/402) and 2.2% (12/546), respectively. According to the clinical T stage, the rates of HNB were 0.6% (2/337) in T1 stage and 4.6% (3/65) in T2 stage within development set, and 2.5% (10/403) in the T1 stage and 1.4% (2/143) in the T2 stage within validation set.
Predictable factors for HNB
To investigate the factors that can predict HNB, multivariable analysis was performed (Supplementary Table 1). Interestingly, positive axilla on MRI showed marginal significance for predicting HNB (adjusted OR, 2.7; P = 0.059), following after lymphovascular invasion (adjusted OR 3.4; P = 0.023).
Diagnostic performance of breast MRI
FNR of breast MRI were 16.3% (60 of 367 patients) within development set and 13.4% (64 of 476 patients) within validation set. For predicting additional LN metastasis in patients with negative AUS, the NPVs of breast MRI in both development and validation sets were high (83.6% [307/367] and 86.5% [412/476]) while PPVs were low (60.0% [21/35] and 58.5% [41/70]). The sensitivities were low (25.9% [21/81] and 39.0% [41/105]), whereas the specificities were high (95.6% [307/321] and 93.4% [412/441]) (Table 2).
Table 2
Diagnostic performance of breast MRI in patients with negative axillary ultrasound finding

Development of nomogram with clinical-imaging factors
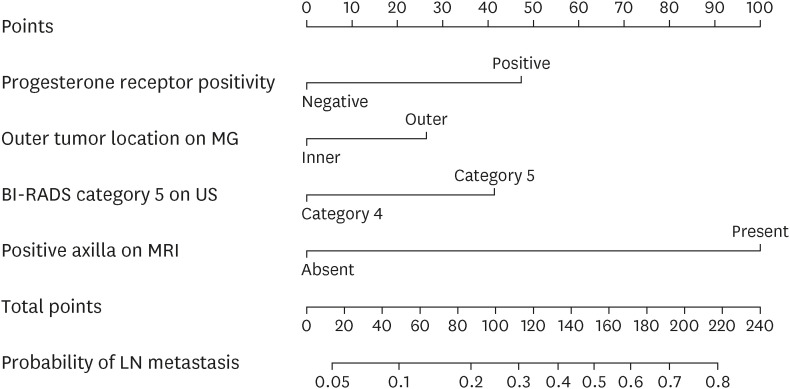
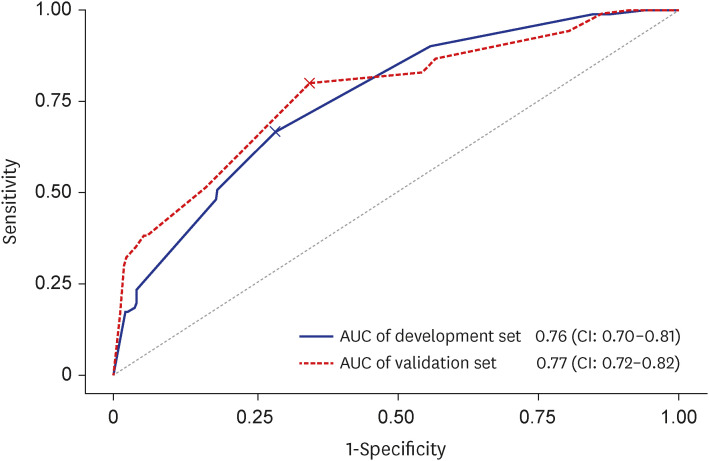
Among clinical factors, lymphovascular invasion, higher pathologic T stage, and PR positivity were factors associated with LN metastasis at univariable analysis (Table 3). Among imaging factors, outer tumor location on mammography, higher clinical T stage measured on US, BI-RADS 5 assessment category on ultrasound, and positive axilla on MRI were significant factors (Table 4). For development of clinical-imaging nomogram which could be used preoperatively, we selected significant clinical and imaging predictors which could be obtained before operation. Therefore, pathologic T stage and lymphovascular invasion which could be assessed after operation were not selected. At multivariable analysis, significant clinical-imaging predictors were PR positivity (adjusted OR, 2.8; P = 0.017), outer tumor location on mammography (adjusted OR, 1.8; P = 0.043), BI-RADS category 5 on US (adjusted OR, 2.6; P = 0.002), and positive axilla on MRI (adjusted OR, 7.8; P < 0.001). However, clinical T2 stage measured on ultrasound did not acquire the significance (adjusted OR, 1.5; P = 0.260) (Table 5). The nomogram integrating clinical and imaging factors was constructed (Fig. 3). The AUC of the clinical-imaging nomogram was 0.76 (95% confidence interval [CI], 0.70–0.81) in the development set and 0.77 (95% CI, 0.70–0.81) in the validation set (Fig. 4). The NPV of clinical-imaging nomogram in the validation set was 82.0%.
Table 3
Univariable analysis of axillary LN metastasis in relation to clinical characteristics in the development set
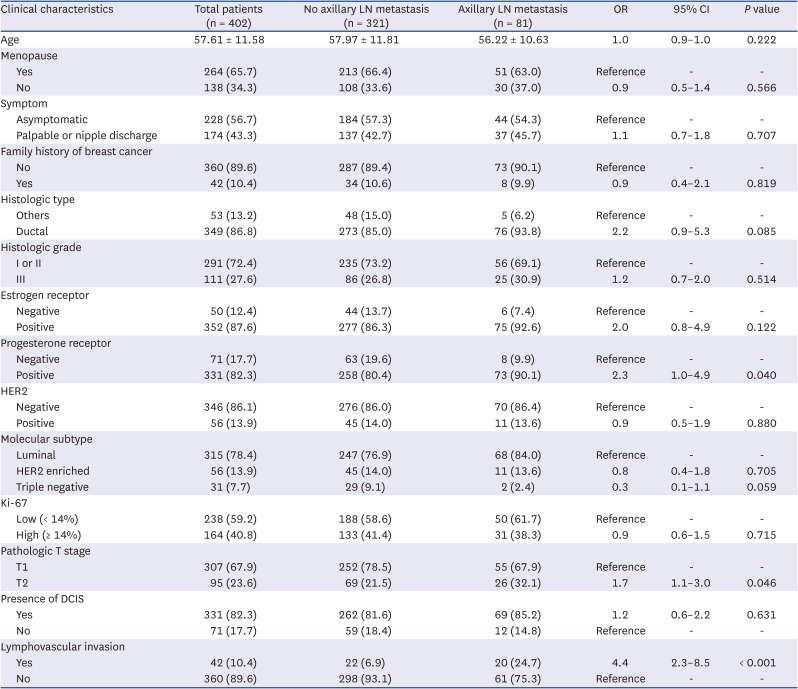
Table 4
Univariable analysis of pathologic LN metastasis in relation to imaging features in the development set
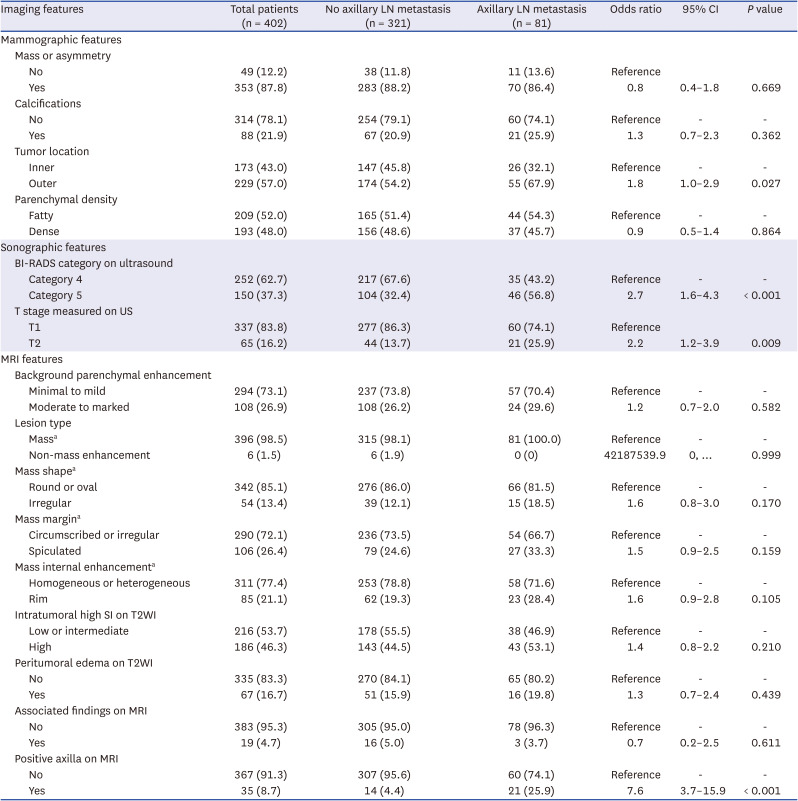
Table 5
Diagnostic performances of clinical-imaging nomogram in validation set

CI = confidence interval, AUC = area under the curve, MG = mammography, US = ultrasound, BI-RADS = breast imaging reporting and data system, MRI = magnetic resonance imaging.
aNumbers in parentheses are 95% CIs.
bP value was acquired from comparison with the reference standard using the Delong method.
Fig. 3
Clinical-imaging nomogram. Each point that corresponds to each feature is on the uppermost point scale, and the sum of all points is the total points. The total points projected at the bottom scale indicate the probability of LN metastasis.
MG = mammography, BI-RADS = breast imaging reporting and data system, US = ultrasound, MRI = magnetic resonance imaging, LN = lymph node.
DISCUSSION
Although imaging strategies for the axilla vary among institutions,20 many centers routinely include AUS as part of the clinical examination because the false negative rate of physical examination has been reported as high as 45%.26 AUS was recently added as a routine workup for axilla in patients with invasive breast cancer according to the National Comprehensive Cancer Network (NCCN) guidelines.22 Moreover, AJCC manual defined clinically suspicious nodes as having palpability on physical examination or suspicious imaging features.21 Considering clinically ongoing trials such as SOUND, INSEMA, and BOOG 2013-08, the role of negative AUS in triaging omission of SLNB has become more important. In our study, the FNR of AUS was 19.2% and 20.1%, which were slightly lower than the 23.4–25% of previous studies.2728 These studies reported that the rate of HNB was 4.2% and 6.7%, which were higher than our rates of 1.2% and 2.2%, respectively.2728 Accordingly, we can conclude that negative AUS can miss LN metastasis in approximately 20% of cases. However, the rate of HNB, according to the Z0011 trial, was low.
Breast MRI is usually recommended for patients with advanced cancers who will receive NAC.2930 Controversy remains regarding the use of MRI in early-stage breast cancer. For omission of SLNB in T1-2 N0 breast cancers, the role of MRI needs to be re-evaluated because it can detect additional LN metastasis missed by AUS.10 In this study, the diagnostic performance of MRI was not satisfactory with low PPVs. However, MRI had merit in reaffirming negative axilla by AUS with high NPVs. Furthermore, predictors for HNB were only lymphovascular invasion and positive axilla on MRI, concordant with a recent study that demonstrated that positive axilla on MRI could predict pathologic N2-3 stage.31 Therefore, surgeons should be careful when omitting SLNB in the presence of positive axilla on MRI.
In our study, three imaging features such as outer tumor location on mammography, BI-RADS 5 assessment category of tumor on ultrasound, and positive axilla on MRI were valuable factors for predicting axillary LN metastasis. Previous study also insisted that outer tumor location was the significant factor affecting LN metastasis in clinically T1-2 N0 breast cancer patients.32 In addition, BI-RADS 5 assessment category on US is known to be associated with larger tumor size, axillary LN metastasis, and lymphovascular invasion.33 Therefore, outer tumor location on mammography and BI-RADS 5 assessment category of tumor on ultrasound, as well as positive axilla on MRI should be considered with significance for predicting LN metastasis.
Among clinicopathological factors, lymphovascular invasion was the most powerful predictor, followed by PR positivity and pathologic T stage. While lymphovascular invasion is a well-known predictor for axillary LN metastasis,141517 the reason why PR positivity affects LN metastasis is less known. It can be assumed that progestins support metastasis of tumor cells,33 and the short PR isoform is a major driver in promoting metastasis of luminal breast cancer by suppressing estrogen/ER action.34 As lymphovascular invasion and pathologic T stage were not factors that could be acquired before surgery, we made a nomogram using significant clinical and imaging predictors which could be obtained preoperatively. Although clinical-imaging nomogram is not perfect considering NPV of 82.0%, our nomogram might be helpful to find possible candidates for the omission of SLNB in patients with clinically T1-2 N0 breast who had negative AUS.
Regarding T stage, the rate of HNB according to the T stage is an important issue in ongoing trials. The inclusion criteria for the SOUND trial were T1 stage, while those for INSEMA and BOOG 2013-08 trials were the T1-2 stages. A recent study advocated the continued use of SLNB in T2 stages because negative AUS has a rate of 6.2% of HNB in T2 stages, higher than 2% in T1 stages.27 In our study, the rates of HNB were 0.3% and 1.9% in the T1 stage and 4.2% and 2.9% in the T2 stage in development and validation sets. Anticipatory to our expectations, clinical T stage measured on ultrasound did not acquire the significance at multivariable analysis. These findings would help provide evidence for determining whether the T2 stage is included in the omission of SLNB in clinical trials.
Our study has several limitations. First, we excluded patients with negative US-guided fine-needle aspiration biopsy (FNAB) results because their AUS findings were positive. FNAB was routinely performed in hospital A, but not hospital B. So, we decided to exclude those patients despite NCCN guidelines and ongoing clinical trials6782135 considered patients with negative FNAB results as negative axilla. Second, this was a retrospective study with small sample size. Third, there were significant differences in the clinical features between the two sets. However, this inherent limitation is unavoidable, and we believe that these differences can reflect the real clinical situation among different institutions. Fourth, the assessment of axillary LN and BI-RADS category depends on the radiologists’ expertise and can be subjective. Because of the nature of retrospective study design, consensus on the criteria was not exactly established and criteria may differ according to the radiologists and institutions. This can limit the application of the clinical-imaging nomogram using imaging features assessed by other radiologists who are likely to have different results interpreting axillary LN status and BI-RADS category.
In conclusion, negative AUS by experienced radiologists missed LN metastasis in approximately 20% of case but the rates of HNB were low in clinically T1-2 N0 breast cancer patients. Breast MRI had merit in reaffirming negative AUS and positive axilla on MRI can help predict HNB. Although clinical-imaging nomogram is not perfect considering NPV of 82.0%, patients who had low probability scores from our nomogram might be candidates for the omission of SLNB. In line with the upcoming results of ongoing trials, our investigation could contribute to future national/international guidelines about axillary LN management.
 XML Download
XML Download