

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
While widespread coronavirus disease 2019 (COVID-19) vaccinations have been highly effective in reducing hospitalization and deaths in many countries, cases continue to surge, and many individuals, including immunocompromised individuals and those who cannot be vaccinated, remain at high risk.1 The discovery that people with preexisting immune dysfunction have an increased risk of developing a breakthrough infection, especially as new variants such as omicron occur that could result in lower vaccine efficacy despite receiving all of the recommended vaccinations, fits in with recent research showing that some people with autoimmune diseases, chronic inflammatory diseases, and solid organ transplants have a decreased antibody response to vaccination.2 The phase III PROVENT trial showed that tixagevimab and cilgavimab significantly (77%) reduced the risk of developing symptomatic COVID-19 in vulnerable populations.3 In December 2021, the US Food and Drug Administration (FDA) granted emergency use authorization for a long-acting monoclonal antibody (mAb) (brand name: Evusheld), which is a combination of two mAbs, given in two consecutive injections in one visit to eligible patients (those who do not have COVID-19 infection).4 They can thus be administered every 6 months to patients at risk for inadequate response to active immunization.3 In addition, sotrovimab is used for the treatment of early COVID-19 and is currently being investigated for pre-exposure prophylaxis (PrEP),567 as an additional option for SARS-CoV-2 PrEP.8 The single center study reported that with sotrovimab, breakthrough infections were rare (10% vs. 30%) when compared to overall infection rates during this period, with mild disease course and rapid viral clearance (median 10 days). However, larger, multi-center randomized trials are required to investigate the clinical effectiveness of sotrovimab PrEP in preventing infection, severe disease, and death.8
With the fast-evolving nature of variants of concern such as omicron BA.2.75., PrEP study about immunosuppressed patients (or unvaccinated patients for various reasons) remains important as they might contribute to the development of new COVID-19 variants, which PrEP may be useful in preventing this outcome.9 Yet, evidence regarding the cost-effectiveness of this preventative treatment intervention among different types of vulnerable populations under varying epidemic scenarios is lacking. Therefore, in this study, we estimated the cost-effectiveness of using long-acting mAbs (tixagevimab and cilgavimab) as PrEP for individuals at high risk of developing severe COVID-19.
METHODS
Effectiveness model and interventions
We used an extended COVID-19 transmission modeling framework structured to capture the demographic and epidemiological processes underpinning the COVID-19 epidemic in South Korea.10 We incorporated four key populations, namely immunocompromised (vaccinated/unvaccinated), severe allergic reactions, and unvaccinated elderly high-risk groups. Selected immunocompromised patients were determined based on the Centers for Disease Control and Prevention (CDC) category among moderately or severely immunocompromised groups.1112 Unvaccinated persons at a high risk of severe disease were defined as those aged over 75 years, among those aged under 65 years with cancer, cardiovascular disease, chronic kidney disease, chronic lung disease, diabetes, receipt of immunosuppressive medications, or obesity (body mass index ≥ 30), based on the CDC category among underlying medical conditions associated with higher risk for severe COVID-19.13 The severe allergic reaction risk groups were defined as those who received immediate anaphylactic shock to the COVID-19 vaccine and its ingredients based on the CDC’s category of allergic reaction after being vaccinated with COVID-19, not other vaccines.14 Considering the various circulating omicron subvariants (BA.2, BA.2.12.1, BA.4, and BA.5) in the US, the FDA recommended doubling the initial dose to tixagevimab 300 mg/cilgavimab 300 mg in February 2022, and we applied these doses and price to our modeling analysis.4
The model includes COVID-19-uninfected, exposed, asymptomatic, asymptomatic detected, symptomatic detected, vaccinated, recovered, and dead cases, and calibrated the detected cases to observed test-positive cases (by age and calendar time). Full details of the model population demography and COVID-19 natural history are described in the Supplementary Materials (Supplementary Figs. 1, 2, 3, Supplementary Table 1) and in a previous study.10 We calibrated the model output to the observed incidence from January 1 to May 30, 2022, and projected the expected incidence from June 1 to December 31, 2022, for the respective risk groups. We estimated the effectiveness of Evusheld as COVID-19 symptomatic cases (and deaths) averted and quality-adjusted life years (QALYs) lost over the analytic horizon based on 77% efficacy in reducing the risk of developing symptomatic COVID-19 compared with the base case scenario (without Evusheld) for each group.3 Due to the lack of data to estimate the respective target risk group among the COVID-19 infected population, we assumed that transmission of the omicron variant was widespread regardless of vaccination status or comorbid conditions and thus considered the same proportions of the total population (i.e., 3.4% for vaccinated immunocompromised group, 0.023% for unvaccinated immunocompromised group, 0.031% for severe allergic reaction group, and 1.86% for unvaccinated high-risk elderly group) among symptomatic test-positive patients for the respective risk groups.151617 These populations were considered independently without excluding overlaps; for instance, immunocompromised individuals may also be included in elderly high-risk populations or have severe allergic reactions. Our primary outcome was the incremental cost-effectiveness ratio (ICER), expressed as 2022 US dollars per QALY gained, comparing Evusheld intervention strategy to the baseline across respective risk groups.
QALY estimates
The QALY is a measure of disease burden, including health-related quality of life and quantity of life lived.18 We estimated the QALYs gained from the projected number of COVID-19 symptomatic severe cases averted by each intervention over a 1-year time horizon in 2022. We used published data to estimate the probabilities of hospitalization and case fatality of COVID-19 cases in South Korea within each key risk group population and the remaining life years of individuals who died of COVID-19 (based on the life expectancy and the mean age at COVID-19 diagnosis by risk populations estimated).192021222324 We also incorporated the disabilities associated with the existing risk conditions.25 We estimated QALY lost from the potential toxicity during the Evusheld preventive treatment (assuming that 35% of patients experienced toxicity), although it was almost negligible given the short treatment duration (1 day) and low disability (0.1). The net number of QALYs gained for each intervention was estimated as the difference between QALYs gained due to averted COVID-19 symptomatic cases and QALYs lost due to the toxicity of the Evusheld treatment.
Unit cost estimates
We used published literature and other publicly available sources to estimate unit costs per person treated for Evusheld and per case of COVID-19 symptomatic severe cases averted. In estimating these unit costs, we estimated the cost of Evusheld intervention, including drug, outpatient visit, and toxicity management costs.26 We then estimated the cost of COVID-19 symptomatic severe cases averted, including COVID-19 treatment cost without hospitalization (oral treatment with Paxlovid) and hospitalization (health system costs) based on the relevant percentage of hospitalization with existing risk conditions (Table 1).25272829
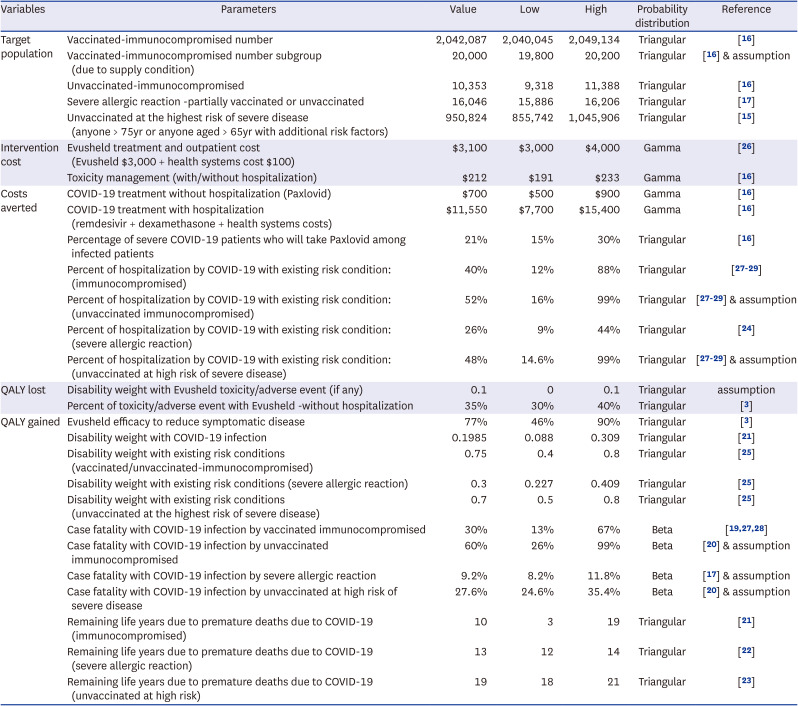
Table 1
Selected input parameters
| Variables | Parameters | Value | Low | High | Probability distribution | Reference |
|---|---|---|---|---|---|---|
| Target population | Vaccinated-immunocompromised number | 2,042,087 | 2,040,045 | 2,049,134 | Triangular | [16] |
| Vaccinated-immunocompromised number subgroup (due to supply condition) | 20,000 | 19,800 | 20,200 | Triangular | [16] & assumption | |
| Unvaccinated-immunocompromised | 10,353 | 9,318 | 11,388 | Triangular | [16] | |
| Severe allergic reaction -partially vaccinated or unvaccinated | 16,046 | 15,886 | 16,206 | Triangular | [17] | |
| Unvaccinated at the highest risk of severe disease (anyone > 75yr or anyone aged > 65yr with additional risk factors) | 950,824 | 855,742 | 1,045,906 | Triangular | [15] | |
| Intervention cost | Evusheld treatment and outpatient cost (Evusheld $3,000 + health systems cost $100) | $3,100 | $3,000 | $4,000 | Gamma | [26] |
| Toxicity management (with/without hospitalization) | $212 | $191 | $233 | Gamma | [16] | |
| Costs averted | COVID-19 treatment without hospitalization (Paxlovid) | $700 | $500 | $900 | Gamma | [16] |
| COVID-19 treatment with hospitalization (remdesivir + dexamethasone + health systems costs) | $11,550 | $7,700 | $15,400 | Gamma | [16] | |
| Percentage of severe COVID-19 patients who will take Paxlovid among infected patients | 21% | 15% | 30% | Triangular | [16] | |
| Percent of hospitalization by COVID-19 with existing risk condition: (immunocompromised) | 40% | 12% | 88% | Triangular | [272829] | |
| Percent of hospitalization by COVID-19 with existing risk condition: (unvaccinated immunocompromised) | 52% | 16% | 99% | Triangular | [272829] & assumption | |
| Percent of hospitalization by COVID-19 with existing risk condition: (severe allergic reaction) | 26% | 9% | 44% | Triangular | [24] | |
| Percent of hospitalization by COVID-19 with existing risk condition: (unvaccinated at high risk of severe disease) | 48% | 14.6% | 99% | Triangular | [272829] & assumption | |
| QALY lost | Disability weight with Evusheld toxicity/adverse event (if any) | 0.1 | 0 | 0.1 | Triangular | assumption |
| Percent of toxicity/adverse event with Evusheld -without hospitalization | 35% | 30% | 40% | Triangular | [3] | |
| QALY gained | Evusheld efficacy to reduce symptomatic disease | 77% | 46% | 90% | Triangular | [3] |
| Disability weight with COVID-19 infection | 0.1985 | 0.088 | 0.309 | Triangular | [21] | |
| Disability weight with existing risk conditions (vaccinated/unvaccinated-immunocompromised) | 0.75 | 0.4 | 0.8 | Triangular | [25] | |
| Disability weight with existing risk conditions (severe allergic reaction) | 0.3 | 0.227 | 0.409 | Triangular | [25] | |
| Disability weight with existing risk conditions (unvaccinated at the highest risk of severe disease) | 0.7 | 0.5 | 0.8 | Triangular | [25] | |
| Case fatality with COVID-19 infection by vaccinated immunocompromised | 30% | 13% | 67% | Beta | [192728] | |
| Case fatality with COVID-19 infection by unvaccinated immunocompromised | 60% | 26% | 99% | Beta | [20] & assumption | |
| Case fatality with COVID-19 infection by severe allergic reaction | 9.2% | 8.2% | 11.8% | Beta | [17] & assumption | |
| Case fatality with COVID-19 infection by unvaccinated at high risk of severe disease | 27.6% | 24.6% | 35.4% | Beta | [20] & assumption | |
| Remaining life years due to premature deaths due to COVID-19 (immunocompromised) | 10 | 3 | 19 | Triangular | [21] | |
| Remaining life years due to premature deaths due to COVID-19 (severe allergic reaction) | 13 | 12 | 14 | Triangular | [22] | |
| Remaining life years due to premature deaths due to COVID-19 (unvaccinated at high risk) | 19 | 18 | 21 | Triangular | [23] |
The impact of the Evusheld as “QALY gained” and “cost averted” by the reduced number of hospitalized patients and deaths of each group between with (intervention) and without (comparator) Evusheld under 2022 COVID-19 epidemic scenarios. QALY gained and loss were calculated based on the formula14: QALYs gained where, Qi is the quality of life weight with treatment, Q is the quality of life weight without treatment; L is the average duration of disease, and r is discounting rate.
- Triangular distribution was assumed for target population in probabilistic sensitivity analyses because we do not have enough information. We applied a symmetric triangular distribution with the lower/upper bound shown, taking the base case value as the mode.
- Gamma distribution was assumed for cost parameters in probabilistic sensitivity analyses because the cost data distribution is often long tailed left skewed shape. Parameters of Gamma (k, θ) were estimated with a method of moments: , where x̄ is the sample mean, v̄ is the sample variance.
- Beta distribution was assumed for rate parameters in probabilistic sensitivity analyses because its range is between 0 and 1. Parameters of Beta(α, β) were estimated using a method of moments: , , if ν̄ < x̄(1−x̄), where ν̄ is the sample variance.
QALY = quality-adjusted life year, COVID-19 = coronavirus disease 2019.
Sensitivity analyses
We performed one-way sensitivity analyses to describe the association between each input variable in our model and the primary outcome (i.e., ICER) for each key population in each state. We also performed threshold analyses to address uncertainties in Evusheld costs and real-world efficacy across risk groups, which may change owing to future epidemic conditions (epidemic surge with new variants). To better explore the simultaneous effect of uncertainty ranges across all of our model parameters, we also conducted a probabilistic sensitivity analysis (PSA), in which all model parameter values were randomly sampled over pre-specified distributions. This process was repeated 1,000 times to generate uncertainty estimates around the primary ICER estimate, with 95% uncertainty ranges reported as the 2.5th and 97.5th percentiles of the corresponding distributions.
RESULTS
In South Korea, the Evusheld intervention target population is estimated to be 2,042,087 vaccinated immunocompromised individuals (3.4% of the total population), 10,353 unvaccinated immunocompromised individuals (0.023% of the total population), 16,046 severe allergic reaction individuals (0.031% of the total population), and 950,824 unvaccinated high-risk elderly individuals (1.86% of the total population) in 2022. The cost of this intervention was estimated as $6.5 billion (in 2022 dollars) for the vaccinated immunocompromised group (including $6.3 billion for Evusheld costs and $151 million for toxicity management), $3 billion for the unvaccinated high risk elderly group, $33 million for the unvaccinated immunocompromised group and $51 million for severe allergic reaction group. Based on the observed and projected epidemic scenarios in 2022, treating this number of people was estimated to avert 179,798 COVID-19 symptomatic cases for the total vaccinated immunocompromised (1,042 for the unvaccinated immunocompromised group), 84,302 for the unvaccinated high-risk elderly group, and 1,410 for the severe allergic reaction group. This translates into $957 million ($831 million hospitalization cost averted and $126 million outpatient cost averted) for vaccinated immunocompromised group, $526 million ($467 million hospital cost averted and $59 million outpatient cost averted) for the unvaccinated high-risk elderly group, $7 million ($6.3 million hospitalization cost and $730,000 outpatient cost averted) for unvaccinated immunocompromised group, and $5 million ($4.2 million hospital cost averted and $987,000 outpatient cost averted) for the severe allergic reaction group (Supplementary Table 2).
The total QALY gained by averting COVID-19 symptomatic cases estimated by reflecting the risk group-specific mean age of COVID-19 diagnosis, expected life expectancy, disutility weight with existing conditions, probability of hospitalization, and case fatality rate due to COVID-19 as well as the number of expected severe symptomatic COVID-19 cases averted. There were 119,039 if treated in all vaccinated immunocompromised groups, 104,007 if treated in the unvaccinated high-risk elderly group, 1,336 if treated in the unvaccinated immunocompromised group, and 995 if treated in the severe allergic reaction group (Supplementary Tables 2 and 3). Greater COVID-19 case fatality and hospitalization with lower disutility from existing conditions resulted in a greater unit QALY gained (i.e., unvaccinated immunocompromised risk group as 1.31, unvaccinated high-risk elderly group as 1.23 compared to severe allergic reaction group as 0.71, or vaccinated immunocompromised group as 0.66) by averting COVID-19 symptomatic cases. Together, these resulted in 118,843, 103,916, 1,365, and 994 net QALY gains in the vaccinated immunocompromised, unvaccinated high-risk, unvaccinated immunocompromised, and severe allergic reaction groups, respectively (Table 2).
Table 2
Health impact and incremental cost-effectiveness in deterministic analyses
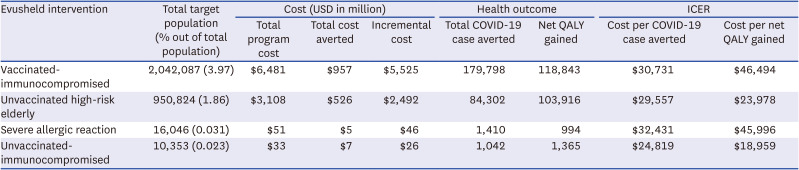
As shown in Table 2, Evusheld is more cost-effective for the unvaccinated immunocompromised group or unvaccinated high-risk group than for the severe allergic reactions or vaccinated immunocompromised groups because of the greater QALY gained by averting symptomatic COVID-19 cases. Evusheld treatment intervention resulted in an ICER for the baseline scenario of $46,464 per QALY gained (95% uncertainty interval, $6,029–$1.95 million) for vaccinated immunocompromised populations (and similar to $49,709 per QALY gained for the immunocompromised population subgroup, but the program costs were almost ten times lower, reflecting the relative population size), $23,978 per QALY gained unvaccinated high risk elderly groups ($7,424–$59,726), $18,959 per QALY gained ($3,028–$851,240) for the unvaccinated immunocompromised group, and $45,996 per QALY gained ($11,880–$73,325) for the severe allergic reaction group.
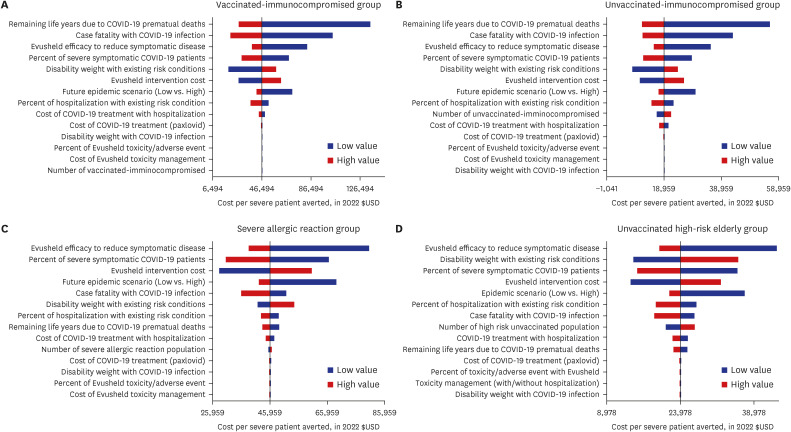
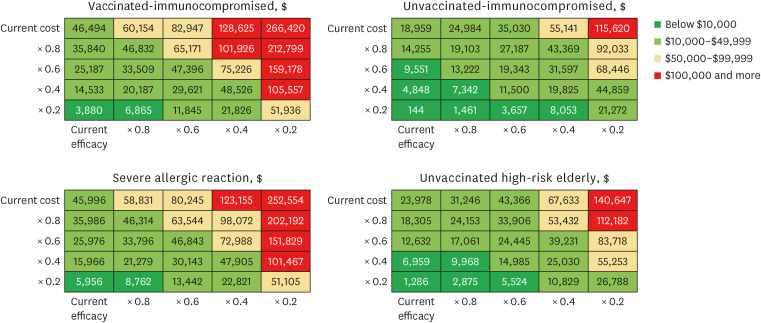
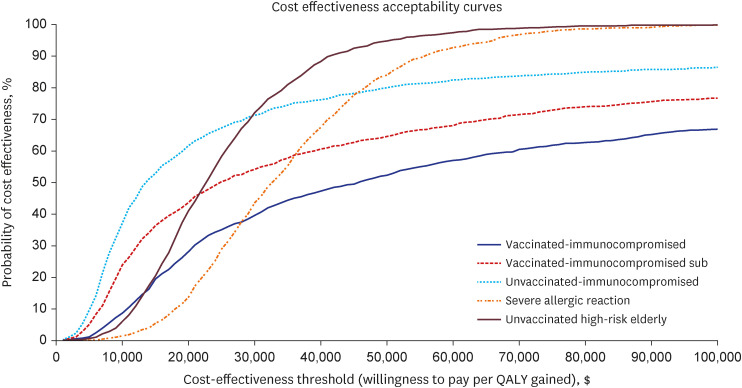
The most important determinants of overall Evusheld cost-effectiveness included the remaining life years due to COVID-19 premature death with existing conditions, case fatality from COVID-19 infection, the efficacy of Evusheld, percentage of severe symptomatic COVID-19 patients, and Evusheld intervention costs. The rank ordering of these variables in the one-way sensitivity analyses varied across the key populations (Fig. 1, Tornado diagram). The threshold analyses varying Evusheld cost and efficacy show that the future cost reduction (20% of the current level) may substantially reduce ICER, $3,880 per QALY gained for vaccinated immunocompromised group and $1,286 per QALY gained for the unvaccinated highest-risk group. The reduced real-world efficacy of 60% of the current level (77%) with the current cost, ICER, would be below $100,000 per QALY gained as a priori threshold value (about three times of South Korea’s gross domestic product per capita: $31,000) for any risk group (Fig. 2). The results of the PSA, displayed in the cost-effectiveness acceptability curves, show the probability of the intervention being cost-effective under different willingness-to-pay thresholds. Most risk groups show that almost 70% of the simulations fall below the threshold value of $100,000 per QALY gained (Fig. 3).
DISCUSSION
This model-based analysis describes how the cost-effectiveness of Evusheld for COVID-19 infection in South Korea varies across the key populations that we examined. Specifically, Evusheld’s cost-effectiveness was consistently the greatest among unvaccinated risk groups (immunocompromised and high-risk elderly groups) and moderate among individuals who were vaccinated immunocompromised or had severe allergic reactions. While we assumed a similar susceptibility of COVID-19 across risk groups, the increased risk of infection/reinfection, especially among unvaccinated groups, may result in Evusheld being more cost-effective in these groups than in other groups. The total intervention costs were the highest for the vaccinated immunocompromised group ($6.5 billion), following the unvaccinated high-risk group ($3 billion), severe allergic reaction group ($51 million), and unvaccinated immunocompromised groups ($33 million), reflecting the size of the target population. The net QALY gained, however, was similar for the vaccinated immunocompromised group (118,843) and unvaccinated high-risk elderly group (103,916), but relatively lower for the unvaccinated immunocompromised group (1,365) and severe allergic reaction group (994), reflecting risk group-specific demographic and disease conditions. Evusheld cost-effectiveness may be subject to assumptions regarding risk group-specific COVID-19 disease progression (hospitalization or case fatality rates) and Evusheld efficacy/cost, which may be influenced by future epidemic scenarios.
Interestingly, this analysis suggests that the cost-effectiveness of the immunocompromised group may substantially differ according to vaccination status ($19,484 for unvaccinated vs. $49,515 for vaccinated) due to their high case fatality with COVID-19 when unvaccinated. The greatest uncertainty and possible heterogeneity within this group include the remaining life years and case fatality with COVID-19 infection and Evusheld efficacy. If Evusheld’s real-world efficacy is lower for the unvaccinated group, the ICER may be higher than $18,959 for this group. As disease progression (hospitalization or case fatality) of COVID-19 in the severe allergic group is lower given the generally younger age population characteristics, the QALY gained by Evusheld of this group is the lowest compared to other groups resulting in relatively less benefit from Evusheld compared to unvaccinated risk groups. While we generally assumed 35% Evusheld toxicity across the risk groups, the level of increased risk/disutility of Evusheld toxicity/resistance among this group may result in Evusheld being less cost-effective.
Decisions about which populations should be treated and prioritized for Evusheld must consider the demographic/biological/behavioral characteristics of each person and also within risk groups (i.e., COVID-19 progression such as hospitalization and level of case fatality and social mixing/preventive treatment acceptance level as well as supply/demand condition of COVID-19 treatment such as Paxlovid), future epidemic waves, and the potential impact of new variants.30 For example, the risk-benefit balance of Evusheld of specific populations and their responses to future epidemic scenarios might be less favorable (with new variants with lower transmissibility and progression) or more beneficial (with new variants with high transmissibility and progression) than presented in this analysis. Similarly, Evusheld’s cost-effectiveness can be subject to the overall vaccination coverage in the population, which affects the extent of COVID-19 cases averted across the risk groups. In other words, in settings where the vaccination coverage is low, Evusheld’s cost-effectiveness may be greater, especially in those risk groups who are unvaccinated. However, this should not be considered a relative superiority of Evusheld over vaccination in preventing COVID-19 infection and progression among these populations. Cost-effectiveness can also be subject to the relative cost of the available COVID-19 treatment (e.g., Paxlovid) and preventive treatment (e.g., Evusheld) by the future epidemic conditions; For example, if another COVID-19 epidemic surge is expected or COVID-19 becomes seasonally endemic, Evusheld may be more cost-effective with potential price reduction with mass production (which may be balanced off to a certain degree by Paxlovid price reduction with its mass production).
This study has some limitations. First, since we were targeting small high-risk populations, we conservatively ignored the impact by preventing secondary infections from the target risk population. We also assumed that risk conditions/vaccination status may have no considerable difference in transmission/infections (under widespread omicron wave) and thus accounted for the health impact by assuming the same factions out of the general population among COVID-19 infections (due to lack of data on specific risk group profiles among the COVID-19 infected population). Similarly, while we defined our risk groups according to the recommended guidelines,30 there might be considerable heterogeneity within each risk group (e.g., the unvaccinated high-risk elderly group) that may increase or decrease some of our key input estimates. Therefore, we incorporated various sensitivity analyses to address this uncertainty. Second, our cost aversion is based on the estimated percentage (21%) of severe COVID-19 infected patients who may need treatment (e.g., Paxlovid) and did not include other costs associated with disease management. If these costs are considered, the amount of cost averted will be far greater, and the ICER of Evusheld will be lower (more cost-effective) than the estimated value. Third, our costs only included the healthcare system costs of treatment and excluded program implementation costs (identification of populations for unvaccinated immunocompromised/high-risk populations, etc.), patient costs, and other societal costs. Given the potential vaccine hesitancy or social stigma toward these at-risk populations, the actual uptake of Evusheld may be less than the estimated target population, while the cost of intervention may be higher. In this case, Evusheld may be less cost-effective than our estimate. Fourth, long-term Evusheld cost-effectiveness is affected by assumptions about long-term efficacy in terms of averted COVID-19 cases and deaths over the following years in a non-static population.31 As the risk group-specific durable efficacy, toxicity (and/or resistance), and optimal dosing of Evusheld remain uncertain, better empirical estimates are needed to inform these values in different epidemiological contexts.32
Recently, there are some concerns and uncertainties regarding the efficacy of Evusheld(tixagevimab/cilgavimab) or other monoclonal antibodies therapeutics such as REGEN-COV (casirivimab/imdevimab) against newer omicron variants which led the UK government and the US FDA to limit its use or purchase of Evusheld.31333435 Other previous studies of post-exposure prophylaxis (PEP) with mAbs such as casirivimab/imdevimab demonstrated that the intervention can be highly cost effective for patients with COVID-19 in ambulatory and hospitalized settings.3637 Another study also demonstrated that PEP with mAbs against household exposure to COVID-19 can be largely cost-saving but depending on transmission scenarios and age thresholds of household contacts.38 None of the studies however have evaluated the cost-effectiveness of Evusheld as PrEP with anti-SARS-CoV-2 mAbs. Our findings therefore may be useful for identifying the areas of key uncertainty across risk groups and prioritizing Evusheld (or other PrEP with similar efficacy) interventions and resource allocation while awaiting additional data. Research on better ways to target efforts to prevent COVID-19 in populations at risk for infection and progression and cheaper but equally effective treatment strategies would help reduce program costs and increase cost-effectiveness. For equitable and inclusive protection against COVID-19, global support for Evusheld provision (with reduced cost) should be considered in developing countries where a high future COVID-19 incidence (with new variants) and high prevalence of immunocompromised populations (e.g., people living with HIV) are present.
As the fight against COVID-19 likely continues with new variants and booster vaccinations, identifying and targeting high-risk and marginalized populations who may not be protected by vaccination would become more critical in controlling future COVID-19 epidemics. Our study demonstrated that the Evusheld’s cost effectiveness for COVID-19 infection in South Korea was consistently the greatest among unvaccinated risk groups (immunocompromised and elderly high-risk groups) and moderate among individuals who were vaccinated immunocompromised or had severe allergic reactions. As the risk group-specific durable efficacy, toxicity (and/or resistance), and optimal dosing of Evusheld remain uncertain, better empirical estimates are needed to inform these values in different epidemiological contexts. These results may help decision makers prioritize resources toward more equitable and effective COVID-19 control efforts.
 XML Download
XML Download