

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Open abdomen (OA) with temporary abdominal closure (TAC) is an essential component of lifesaving damage control surgery (DCS) in trauma, which is associated with high morbidity, mortality, and hospital costs [1234]. Despite advances in trauma care, the selection of TAC is still dependent on the surgeon’s experience. Under ideal conditions, TAC serves as an effective barrier in preventing evisceration, contamination, and bowel injury. Moreover, it can remove unwanted peritoneal fluid and provide easy access for reoperation. Limiting fascial retraction to achieve early definitive fascial closure (DFC) is necessary while allowing for expansion to avoid abdominal compartment syndrome (ACS). Readiness, rapidity, and cost-effectiveness are also required [1256].
Diverse techniques have been developed for TAC, and these can be divided into 3 groups according to the methodology used: skin-only, patch, and vacuum closure techniques [5]. Skin-only closure is achieved by closing the skin with towel clips or sutures, leaving the fascia open. The patch closure technique comprises suturing plastic layers (such as with the use of Bogota bags, mesh [absorbable or nonabsorbable], Wittmann patches, or zippers) to the fascia or skin. Meanwhile, vacuum closure techniques include homemade or commercial negative-pressure wound therapy (NPWT) with or without continuous fascial traction (CFT). Another classification divides TAC into 2 groups depending on whether the fascia is tightened sequentially or not: static therapy (ST) and dynamic therapy (DT) [7]. CFT using dynamic retention sutures or abdominal reapproximation anchor represents DT. The Wittmann patch and mesh-mediated fascial traction can be classified as DTs, but a simple mesh fixation without mention of gradual reduction is considered an ST.
Many consensus guidelines have advocated the use of a vacuum closure as a TAC technique of choice [891011]. As a result, vacuum closure has gained prominence, particularly with the development of industrial versions of it. However, these guidelines depend mainly on the findings of extensive and heterogeneous previous studies that have evaluated TAC. Although the concept of damage control resuscitation (DCR) has transformed the trauma resuscitation practice over the last 20 years, data collected in the pre-DCR era are a significant portion of those studies [12]. Hence, this review aimed to answer the following PICO (Population, Intervention, Comparator, Outcomes) question: in trauma patients with OA in whom emergency laparotomy has been performed, which TAC category (skin-only vs. patch vs. vacuum closure; ST vs. DT) should be performed to obtain better clinical outcomes in terms of mortality, DFC, and abdominal complications?
METHODS
Data sources and search
This study was conducted following the updated PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 statement [13]. The protocol for this systematic review was registered in PROSPERO, an international prospective register of systematic reviews, in 2022 (CRD42022307506) [14]. The Institutional Review Board at Dankook University Hospital exempted the study from review as we conducted a secondary analysis of published, peer-reviewed findings (No. 2022-01-021). A comprehensive search was conducted from the date of database inception to June 2022 using standard web-based databases, including PubMed, Embase, the Cochrane Central Register of Controlled Trials, and Clinicaltrials.gov. The search terms are presented in Supplementary Fig. 1.
Study selection
We included published studies that met the following criteria: (1) study design: randomized controlled trials (RCTs), cohort studies, or case series; (2) study population: trauma patients only; and (3) results: including at least one of the aforementioned endpoints of interest. The exclusion criteria were: (1) studies on nontrauma or pediatric patients; (2) studies with inappropriate data (i.e., data not categorized by the TAC method); (3) case series and reports including <5 cases; (4) reviews, meta-analyses, study protocols, conference abstracts, letters, editorials, commentaries, and in vivo or in vitro research (i.e., research on animals or cell lines, respectively); and (5) non-English publications (except for including articles with English abstract). No restrictions were placed on indications for OA. The study selection process was conducted independently by the 2 study authors and any disputes were resolved by consensus.
Data extraction and definitions
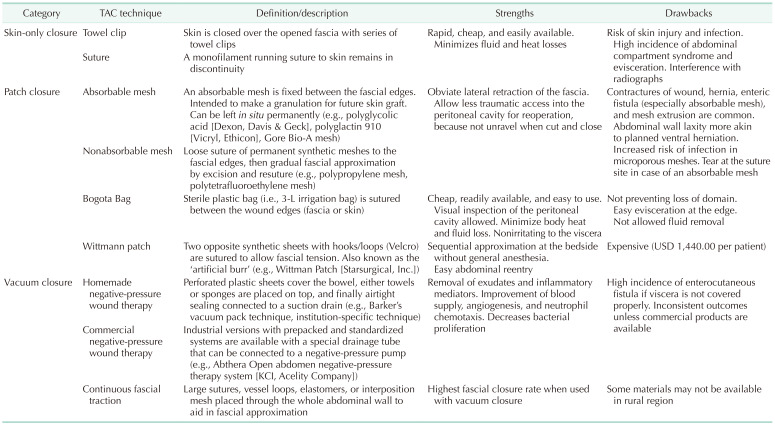
The 2 study authors collected the data independently. The extracted data included primarily basic information, such as the first author and year of publication, baseline study characteristics (including sample size, mean or median values for age, and the Injury Severity Score [ISS] for each group), and clinical endpoints. These endpoints included in-hospital mortality, DFC rates, and the incidence of 3 abdominal complications (enteric fistula [EF], ventral hernia [VH], and peritoneal abscess [PA]) by the TAC group. DFC was defined as the attainment of complete midline fascial closure without prosthesis, regardless of the number of days necessary for this to occur. EF includes both enterocutaneous and enteroatmospheric fistulas. Any mention of unplanned protrusion of the peritoneal contents between the fascia following DFC was considered VH. If the outcomes of interest were not mentioned in the published studies, they were considered unavailable. Recognized TAC techniques (NPWT with or without CFT, skin tension, meshes, Bogota bags, Wittman patches) were classified as skin-only vs. patch vs. vacuum closures and ST vs. DT. The descriptions, strengths, and drawbacks of each TAC technique (according to a comprehensive review of the literature) are summarized in Table 1.
Data synthesis and analysis
All the analyses were performed using the meta-analysis module in R (ver. 5.1-1; The R Project for Statistical Computing) [15]. Forest plots were created to display the results of the data synthesis visually (Supplementary Figs. 2, 3, 4, 5, 6). Weighted proportions and 95% confidence intervals (CIs) were generated for comparisons of each TAC category. If there was a statistically high heterogeneity (I2 ≥ 5 0%) a mong t he s tudy results for a given outcome, the random-effects model was used as a reference; otherwise (I2 < 50%), a fixed-effects model was used. The 2 authors independently evaluated the methodological quality of RCTs and non-RCTs using a revised Cochrane risk of bias tool for randomized trials (RoB 2) and the Newcastle-Ottawa scale (NOS), respectively [1617].
RESULTS
Characteristics of the included studies
A total of 1,065 relevant publications were identified during our initial literature search. Of these, 2 randomized controlled studies [1819], 29 retrospective observational studies [2021222324252627282930313233343536373839404142434445464748], and 6 prospective observational studies [495051525354] that were published between 1990 and 2022 met the inclusion criteria; these studies included a total of 2,582 patients (Table 2). The study selection process is depicted in Fig. 1.

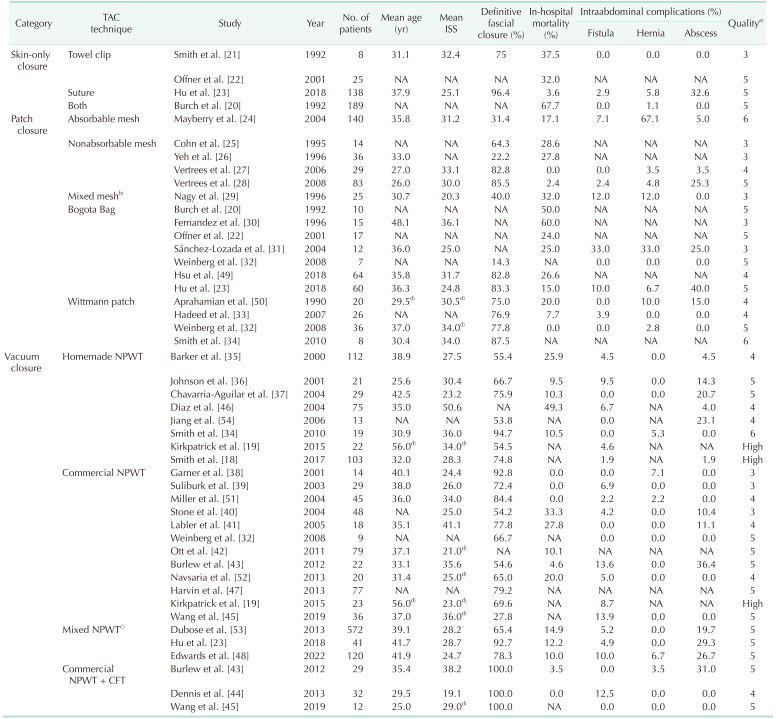
Fig. 1
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 flow diagram.
![]()
Table 2
Demographic and clinical characteristics of the included studies
TAC, temporary abdominal closure; ISS, Injury Severity Score; NA, not available; NPWT, negative-pressure wound therapy; CFT, continuous fascial traction.
a)Quality assessment using the Newcastle-Ottawa scale (out of 9 points) or Cochrane risk of bias tool for randomized trials (low risk or some concerns or high risk). b)Absorbable and nonabsorbable meshes. c)Both homemade and commercial NPWT, or not mentioned. d)Median values.
![]()
According to RoB 2, the risk of bias of the included RCTs was judged as either ‘low risk,’ ‘some concerns,’ or ‘high risk.’ Using the NOS, the quality of the included observational studies ranged from 3 to 6 stars. Although all the studies evaluated post-trauma patients, we identified various indications for TAC, including post-DCS, primary and secondary ACS, peritonitis, planned reoperation, necrotizing fasciitis, necrotizing pancreatitis, and abdominal wall defects. Vacuum closure was the most common TAC category used in 1,620 patients (73.3%, 23 studies) [1819233234353637383940414243444546474851525354] followed by patch closure in 602 patients (27.3%, 16 studies) [20222324252627282930313233344950] and skin-only closure in 360 patients (16.3%, 4 studies) [20212223]. DT was used in 163 patients (6.3%, 7 studies) [32333443444550], whereas the rest used ST.
Meta-analysis results
In-hospital mortality
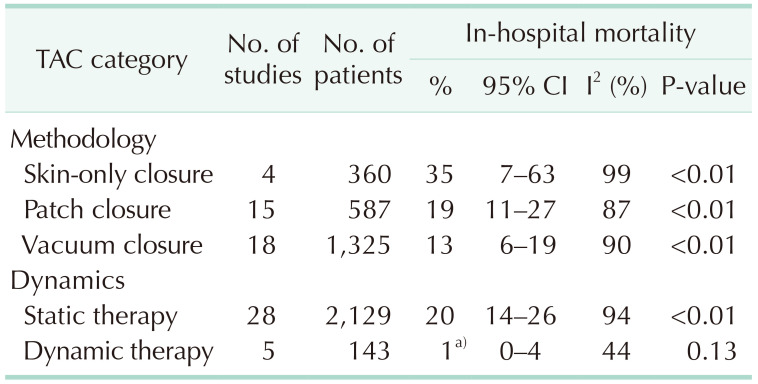
A total of 31 studies presented in-hospital mortality rates [20212223242526272829303133343536373839404142434446484950515253]. The lowest weighted in-hospital mortality rate was observed with the use of vacuum closure (13%; 95% CI, 6%–19%), whereas the highest rates were seen within the skin-only category (35%; 95% CI, 7%–68%) (Table 3). In the second group analysis, DT was superior to ST (1% [95% CI, 0%–4%] vs. 20% [95% CI, 14%–26%]).
Definitive fascial closure rates
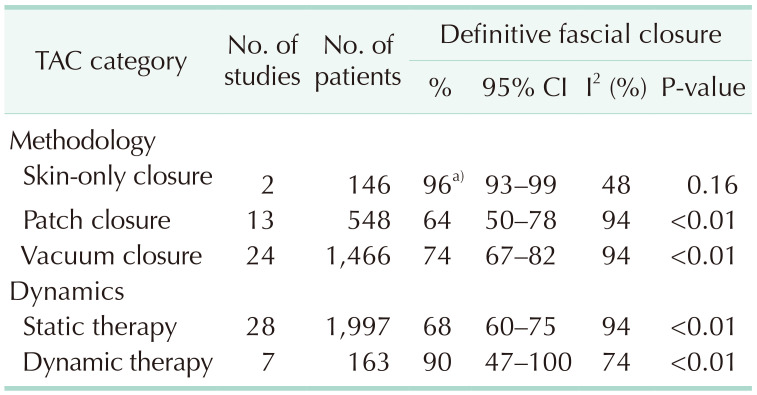
Overall, 31 studies reported DFC rates [18192123242526272829323334353637383940414344454748495051525354]. The highest weighted rate was observed in the skin-only group (96%; 95% CI, 93%–99%), whereas the lowest weighted rate was observed in the patch closure group (64%; 95% CI, 50%–78%) (Table 4). In the second group analysis, DT was superior to ST again (90% [95% CI, 47%–100%] vs. 68% [95% CI, 60%–75%]).
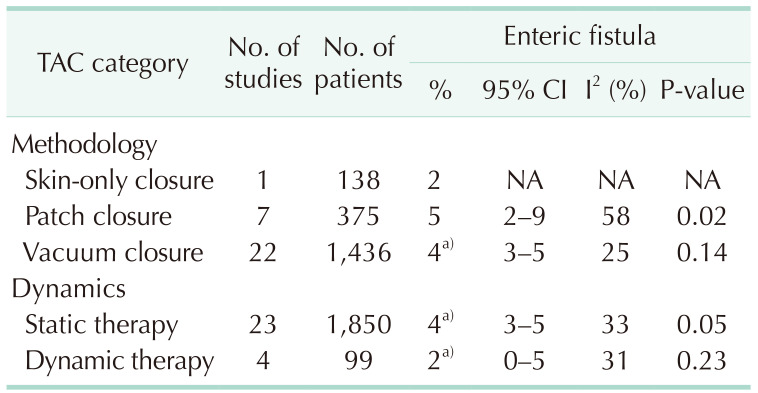
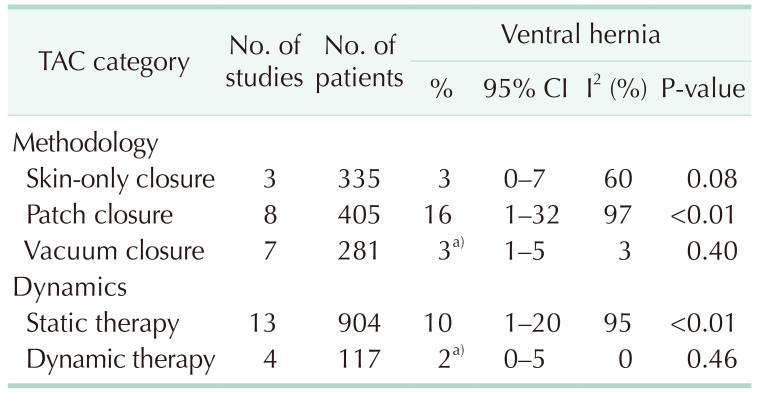
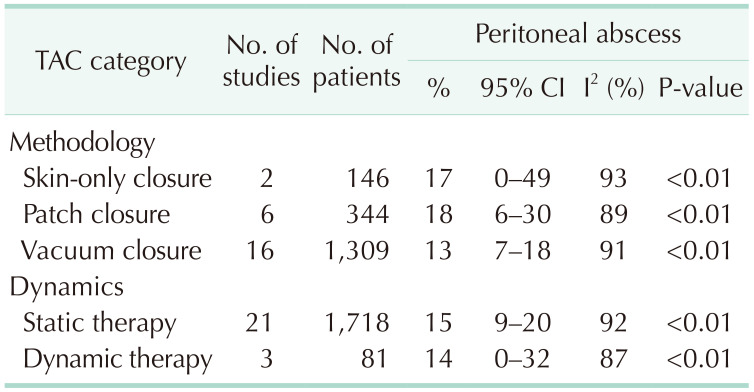
Intraabdominal complications
A total of 29 studies evaluated intraabdominal complications [1819212324272829313233343536373839404143444546485051525354]. Patch closure showed the highest weighted incidences of EF (5%; 95% CI, 2%–9%), VH (16%; 95% CI, 1%–32%), and PA (18%; 95% CI, 6%–30%) (Tables 5, 6, 7). In the second group analysis, DT was superior to ST in EF (2% [95% CI, 0%–5%] vs. 4% [95% CI, 3%–5%]), VH (2% [95% CI, 0%–5%] vs. 10% [95% CI, 1%–20%]), and PA (14% [95% CI, 0%–23%] vs. 15% [95% CI, 9%–20%]).
DISCUSSION
Apposition of the fascia without concern for ACS is the final goal of OA management. DFC failure is anticipated when OA persists beyond 5–8 days or following a third reexploration [655]. The longer the OA persists, the higher the risk of infectious complications because of repeated dressing changes. Among the patients with OA, 25% developed EF, PA, or wound infections; a greater tendency to develop these complications was observed after 8 days [5657]. Moreover, the achievement of DFC beyond 5 days was 4–16.8 times more likely to induce anastomotic leakage [5859]. Once in this downward spiral of abdominal infections hampering DFC, other systemic infections (such as bacteremia or pneumonia) may also arise. Failed DFC increased bloodstream infections (18.4% vs. 6.5%), thereby emphasizing the need to accomplish DFC rapidly when permitted by the patient’s physiology [53].
If DFC cannot be achieved within 8 days, the current trend advocates the initiation of DT [760]. Numerous reports have demonstrated that NPWT with CFT yields better results than NPWT alone, although most study participants evaluated in these prior studies were non-trauma patients [26162]. Accordingly, the World Society of Emergency Surgery and the Eastern Association for the Surgery of Trauma (EAST) recommended NPWT with CFT as the primary technique for TAC [863]. In another meta-analysis and guideline, the EAST recommended that CFT should be used over routine care in the management of OA after DCS [63]. However, the recommendation was limited to hemodynamically stable patients. The increase in the dynamics of TAC is in concordance with the results of the present meta-analysis, where DT showed better outcomes than ST at all endpoints. Nevertheless, these results should be interpreted carefully given the small number of studies that were included in this analysis. Additional protocol-based data using DT are needed to validate the positive findings.
Historically, high mortality of skin-only closure has been attributed to its innate feature of promoting ACS [576465]. ACS is associated with worse outcomes, including increased ventilator days, longer intensive care unit stay, and multi-organ failure [65]. According to our analysis, skin-only closure was significantly more likely to result in DFC than vacuum closure. However, caution is needed in the interpretation, as patients treated with a skin-only technique in the recent cohort have been found to experience less injury burden (selection bias) [23]. In the era of DCR, resuscitation strategies focus on the limitation of visceral edema. Therefore, skin-only closure might be an alternative in selected patients who are less likely to develop ACS (i.e., not require massive volume resuscitation), especially in rural areas where NPWT is unavailable [66]. Further studies are required to confirm whether strict compliance with DCR prevents ACS under the skin sutures.
Our study had some limitations mainly due to data heterogeneity. First, the mean age and ISS of the patients could not be calculated across all the included studies as well as in each category because some of the values were presented as medians. Second, the individual study-level inclusion and exclusion criteria differed markedly between the included studies. Moreover, the indications for OA after trauma were not uniform. DCS was the primary indication for OA with TAC in 22 of 37 (59.5%) studies [1820212223252830323334363941454748495253], with mixed indications reported in another 11 studies [1924273537384046505154]. Only 1 study reported severe peritonitis after trauma [31]. Two studies did not mention the indication for OA [2629]. In addition, 17 studies excluded patients with early mortality (i.e., intraoperative mortality, 24/48/72-hour mortality, and mortality before fascial closure) as this would have diminished the calculated in-hospital mortality rate [1820222433343739424344454749505153]. Third, other confounding factors (i.e., time to closure, variations in practice protocols, evolution of DCR, and reliability of critical care support) affecting permanent closure could not be controlled. The surgeon’s personal preferences in choosing a specific TAC method may likewise have introduced a selection bias into each cohort. Fourth, only 10 studies reported the duration of the study follow-up period [19212432344143444852], which may have impacted the accuracy of the VH incidence findings; this is because VH is usually a long-term complication of OA. The overall poor methodological quality of the available evidence was another limitation of this investigation. Most of the included studies were retrospective investigations. Inherent difficulties in conducting RCTs in trauma centers may explain this finding. Statistical methods to evaluate publication bias were not conducted, as they are not suitable for proportional meta-analysis [67]. Thus, small-study effects must be considered when interpreting our data. Future evaluations with well-designed, high-quality, and highly powered RCTs are warranted to provide more uniform and gold-standard recommendations. Despite these limitations, we provided a roadmap for the optimized selection of TAC methods for trauma surgeons. To the best of our knowledge, this is the first meta-analysis on the use of TAC, including studies performed purely within populations of trauma patients (both hemodynamically stable and unstable patients).
In conclusion, the vacuum closure may have advantages in terms of in-hospital mortality, VH, and PA. The utilization of the skin-only technique should be restricted, considering the potential risk of ACS. Although these study results have highlighted the importance of DT over ST, the potential limitations of data heterogeneity should be considered. Future investigations balancing various confounding variables are required to achieve a more comprehensive understanding of the best TAC technique for the management of OA in trauma patients.
 XML Download
XML Download