

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In 2020, 157,903 new patients with drug-resistant tuberculosis (TB) were diagnosed worldwide, and 150,359 enrolled in treatment, down 22% and 15%, respectively, from 2019.1 This is related to the decrease in TB diagnosis and treatment due to restrictions on patients’ access to medical services in the coronavirus pandemic. Although the number of new patients decreased, in 2020, the deaths from TB increased by 5.6% compared with 2019, and the treatment target for patients with drug-resistant TB in 2018–2022 was far behind at 32%.1 The number of patients with TB, including drug-resistant TB, is expected to increase from 2021. The World Health Organization (WHO) is desperately trying to normalize TB case detection and treatment to achieve its original goals in the next few years.12 In Korea, multidrug-resistant tuberculosis (MDR-TB) showed a decreasing trend of 787, 852, 681, 618, 580, 399, and 371 new patients from 2015 to 2021, and it was estimated that the rapid decrease over the past two years was affected by the pandemic like the global trend.345
For MDR-TB treatment, the WHO recommends all-oral regimens, which consists of only oral drugs, including new drugs, instead of injectables that have more side effects and are inconvenient to use than oral drugs.12 The study, which underlined the revision of WHO recommendations, meta-analysed the data of 12,030 individual patients with MDR-TB included in 50 cohort studies published from January 2009 to April 2016 to analyse the effects of individual drugs associated with treatment outcomes. In this meta-analysis, the drugs that contributed to treatment success and mortality reduction were linezolid, levofloxacin, moxifloxacin, and bedaquiline. In contrast, clofazimine and carbapenem, classified as key drugs, only showed moderate benefits, and kanamycin and capreomycin were associated with poor prognosis.6
In the new all-oral regimens recommended by the WHO, bedaquiline and linezolid are core agents,7891011 and injectables, which had long been classified as core drugs, were excluded from the new regimens. Currently, 90 countries have adopted all-oral longer regimens, and 65 countries use all-oral shorter regimens.12 Many countries have accepted clinical outcomes related to the effectiveness and safety of all-oral regimens, but the high cost of new oral drugs is a barrier to adopting all-oral regimens under the national health insurance benefits, especially in countries with a significant burden for MDR-TB. Although the addition of bedaquiline to background regimen (conventional injectable-containing regimen) was evaluated as cost-effective compared with the background regimen, the health economics of the new all-oral longer regimens and conventional injectable-containing regimens has rarely been evaluated.12131415
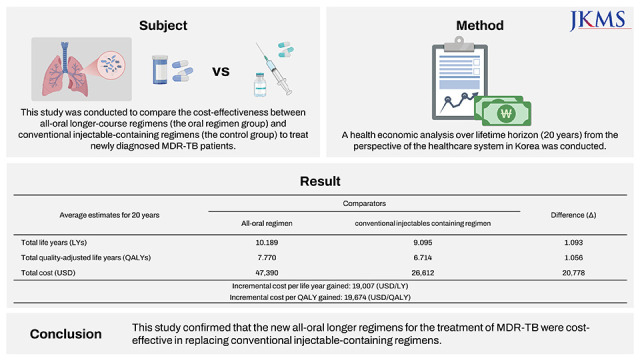
Korea has also updated its MDR-TB treatment guideline to all-oral longer regimens from injectable-containing regimens in accordance with the WHO in 2020 and recommends that all-oral shorter regiments be used selectively only under appropriate patient selection conditions.16 Bedaquiline was approved in Korea in 2014 and has been reimbursed by the government since August 2016 if used to treat MDR-TB patients who cannot be treated with conventional TB drugs. The eligible patients for bedaquiline have been expanded from limited MDR-TB patients who could not be treated with conventional drugs to all MDR-TB patients according to the revision of the TB treatment guidelines and health insurance benefit criteria. The cost-effectiveness of the all-oral regimens in newly expanded patients has not been evaluated in Korea. Thus, this study aimed to evaluate the cost-effectiveness of the all-oral longer regimens compared with the conventional injectable-containing regimens in newly diagnosed MDR-TB patients.
METHODS
Analysis source, target population, and comparators
The analysis source to define the target population and cost data was health big data of Korea, which is combined data of insurance benefits and health examination data from national health insurance sharing service, TB registry data of Korea disease control and prevention agency, and medical claims from the health insurance and review and assessment service (Supplementary Fig. 1). Target patients were newly diagnosed MDR-TB patients in Korea, and the demographic and clinical characteristics were assumed based on the analysis results of health big data of Korea. The average age and proportion of male patients were assumed as 46.99 ± 16.78 years old and 66.75% (Supplementary Table 1). The cost-effectiveness was compared between the two groups: a control group treated with the conventional regimens including injectables without new oral drugs and an oral regimen group treated with all-oral longer-course regimes containing bedaquiline without injectables. (Supplementary Table 2).
Analysis method and settings
Since the progression of TB significantly impacts patients’ physical and mental health-related quality of life, a cost-utility analysis was performed by selecting quality-adjusted life years (QALYs) as an evaluation index. Analysis was conducted from the perspective of the healthcare system in Korea over 20 years of time horizon. The future effectiveness and cost were discounted at 4.5% per year.
Analysis model and health status definition
A combined analysis model using a decision tree model during the initial two years and two Markov models during the remaining period was used to assume QALY and cost in each treatment group (Fig. 1). The cycle length for the Markov models was set as six months.
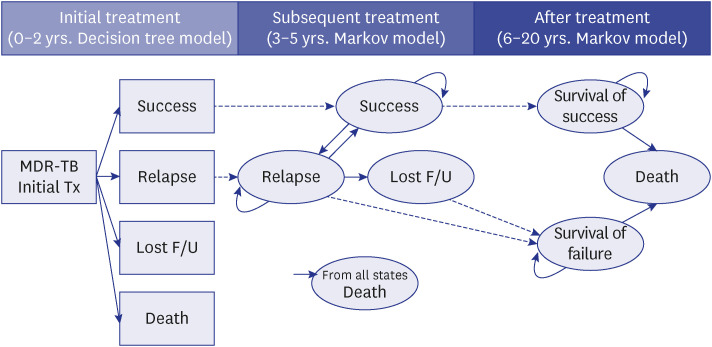
The model contains the following health statuses: 1) Success, the duration of drug discontinuation is shorter than two months after the onset of MDR-TB treatment or 24 months of treatment has been completed. The patient will remain in the state if MDR-TB does not recur; 2) Lost follow-up (F/U), treatment drug discontinuation period is longer than two months, and treatment was not followed after; 3) Relapse, treatment drug discontinuation period is longer than two months, and secondary treatment was followed after the discontinuation; 4) Survival of success, survival of treatment success patients after five years; 5) Survival of failure, survival of relapse or lost F/U patients after five years; and 6) Death.
Transition probability
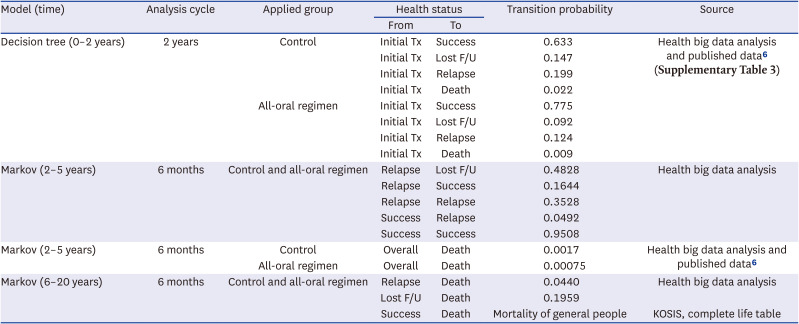
Based on Korean health big data analysis results, the transition probabilities to success, lost F/U, relapse, and death status were assumed to be 63.3%, 14.7%, 19.9%, and 2.2%, respectively, at the end of two years in the control group. The probabilities in the oral regimen group were assumed to be 77.5%, 9.2%, 12.4%, and 0.9% for the success status, lost F/U, relapse, and death using the control group’s results and the adjusted odds ratio (OR) of literature results. The adjusted OR for treatment success and death in the bedaquiline used group versus un-used groups were 2.0 (95% confidence interval [CI], 1.4–2.9) and 0.4 (95% CI, 0.3–0.5) (Table 1, Supplementary Table 3).6 We adopted adjusted ORs for bedaquiline used and un-used groups from the literature6 which were estimated by using generalized logistic mixed effects model with resistance to fluoroquinolones or second-line injectable drugs as covariates after propensity score matching based on individual-level covariates such as sex, age, acid-fast bacilli smear results, human immunodeficiency virus co-infection, cavitation on chest radiographs, history of tuberculosis treatment with first-line or second-line tuberculosis drugs, and number of possibly effective drugs in the initial phase.
Table 1
Transition probabilities
| Model (time) | Analysis cycle | Applied group | Health status | Transition probability | Source | |
|---|---|---|---|---|---|---|
| From | To | |||||
| Decision tree (0–2 years) | 2 years | Control | Initial Tx | Success | 0.633 | Health big data analysis and published data6 (Supplementary Table 3) |
| Initial Tx | Lost F/U | 0.147 | ||||
| Initial Tx | Relapse | 0.199 | ||||
| Initial Tx | Death | 0.022 | ||||
| All-oral regimen | Initial Tx | Success | 0.775 | |||
| Initial Tx | Lost F/U | 0.092 | ||||
| Initial Tx | Relapse | 0.124 | ||||
| Initial Tx | Death | 0.009 | ||||
| Markov (2–5 years) | 6 months | Control and all-oral regimen | Relapse | Lost F/U | 0.4828 | Health big data analysis |
| Relapse | Success | 0.1644 | ||||
| Relapse | Relapse | 0.3528 | ||||
| Success | Relapse | 0.0492 | ||||
| Success | Success | 0.9508 | ||||
| Markov (2–5 years) | 6 months | Control | Overall | Death | 0.0017 | Health big data analysis and published data6 |
| All-oral regimen | Overall | Death | 0.00075 | |||
| Markov (6–20 years) | 6 months | Control and all-oral regimen | Relapse | Death | 0.0440 | Health big data analysis |
| Lost F/U | Death | 0.1959 | ||||
| Success | Death | Mortality of general people | KOSIS, complete life table | |||
The probabilities for the Markov model were assumed, as shown in Table 1, based on data from health big data analysis, literature, and Korean statistical information service. The same transition probabilities were applied to both groups except for the probability of overall death, which applied the OR of 0.4 to the oral regimen group during 3–5 years. The mortality after 5-year survival was assumed based on general population mortality for success status and health big data analysis for lost F/U and relapse status.
Cost and utilities
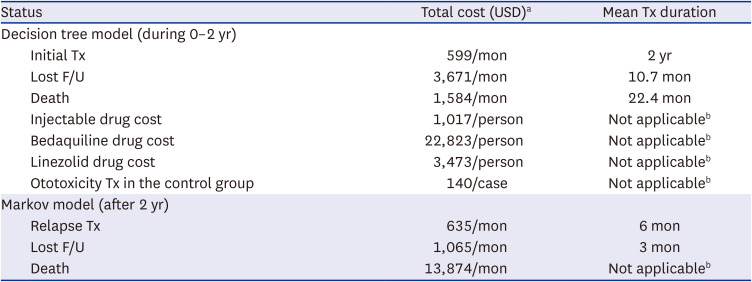
The cost for each health status was assumed based on the health big data analysis. The cost included all direct medical expenses incurred within the healthcare system (such as medication cost, preparation and administration cost, follow-up treatment, patient monitoring, adverse reaction treatment, end-of-life costs, and etc.), and transportation costs, time costs, home-nursing costs and productivity loss costs were not included. All the costs were converted to 2021 price and USD using the consumer price index in the health sector and the exchange rate of 1,200 Korean Won per 1 USD. The initial treatment cost in the oral regimen group included the cost of bedaquiline (22,823 USD per person), which was assumed to administer 400 mg daily for the initial two weeks and 200 mg daily three times a week for 22 weeks, with the unit price of 121.4 USD/100 mg. The cost of linezolid was included in the sensitivity analysis and assumed to be 3,473 USD per person with the administration of 450 mg daily for 180 days. The costs of injectables and administration of drugs were analysed as 1,017 USD per person based on health big data analysis, and the costs were excluded from the initial treatment cost in the all-oral regimen group (Table 2). The utilities for health-related quality of life were assumed as 0.51 for MDR-TB status (on treatment, lost follow-up, relapse) and 0.88 for success status after treatment completion based on literature data.17
Table 2
Cost assumptions
Sensitivity analysis
Deterministic sensitivity analyses were performed on major variables of effect, cost, and settings. A total of 1,000 iterations were performed for probabilistic sensitivity analysis by applying beta distribution for variables of transition probabilities and utility weights, normal distribution for outcome OR, and gamma distribution for cost variables.
RESULTS
Cost-effectiveness of base case results
The effectiveness outcomes were 1.093 life years (LYs) and 1.056 QALY longer, and total treatment costs were 20,778 USD more in the all-oral regimen group compared with the control group. Thus, the incremental cost-effectiveness ratio (ICER) was calculated as 19,007 USD/LY and 19,674 USD/QALY (Table 3, Supplementary Table 4).
Table 3
Results of base case analysis and deterministic sensitivity analysis
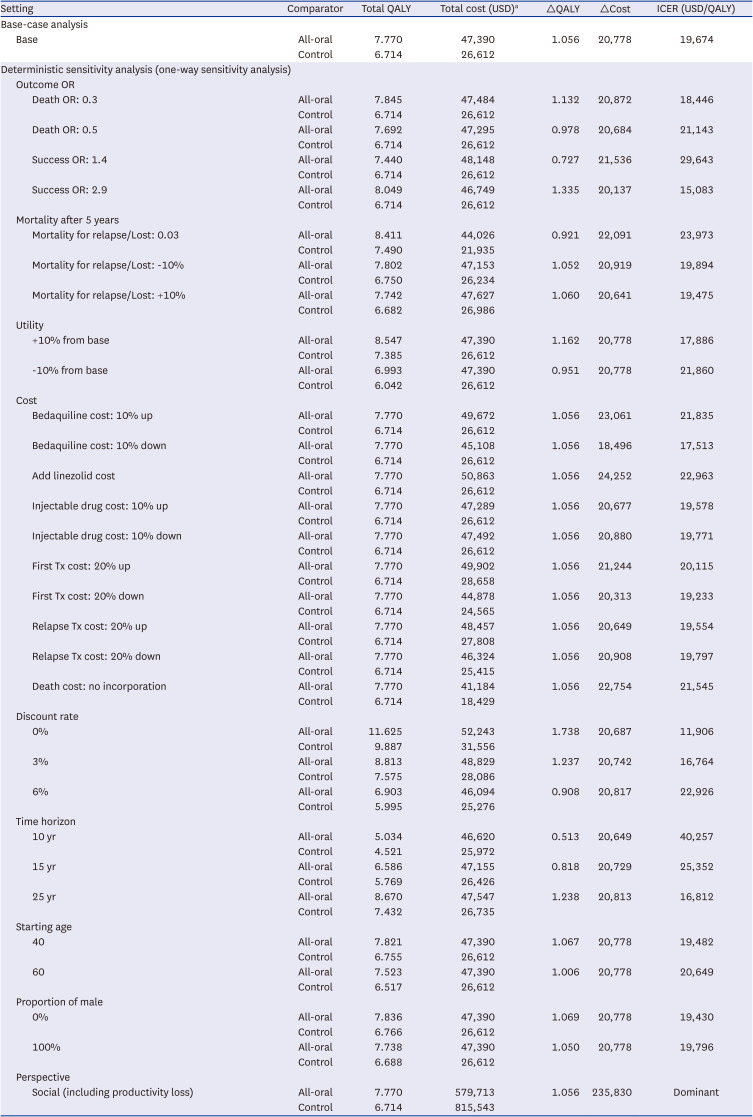
Deterministic sensitivity analysis results
The assumption for success OR between the groups affected ICER results mostly among the variables for effectiveness. The ICER increased to 29,643 USD/QALY when the OR was changed to 1.4 from 2.0. Overall, the change in cost variables had little effect on the ICERs. For the analysis of setting variables, the lower the discount rate, the lower the ICER, and the shorter the time horizon, the higher the ICER. In the sensitivity analysis with a social perspective which included productivity loss, the cost of the oral regimen group was 235,830 USD lower than that of the control group, indicating that the oral regimen group dominated the control group (Table 3, Supplementary Fig. 2).
Probabilistic sensitivity analysis results
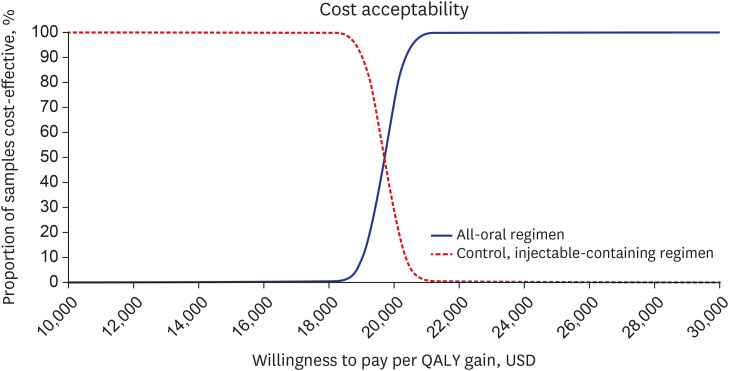
The mean ICER of 1,000 iterations of probabilistic analysis was 19,697 USD/QALY (standard deviation, 515) and the cost and QALY differences of all-oral regimens compared with injectable-containing regimens were shown in the cost-effectiveness plane (Supplementary Fig. 3). The cost-effectiveness of the oral regimen showed a 100% probability when the willingness to pay was above 21,250 USD/QALY (Fig. 2).
DISCUSSION
This study compared the cost-effectiveness of the oral regimen group and the control group (conventional injectable-containing regimens) for the treatment of MDR-TB. The results of this study showed that the ICER of the oral regimen group was 19,697 USD/QALY on average under the setting of Korean healthcare system and a 100% probability of being cost-effective if the willingness to pay threshold is above 21,250 USD.
In the base analysis, the treatment outcome of target patients was better in the oral regimen group than in the control group, as previous cost-effectiveness studies showed.13141518 The oral regimen group was analysed to live about one QALY or one year longer than the control group. The difference in the effectiveness of both groups was most affected by the treatment success rate of the initial two years. Therefore, assuming the probability of treatment success properly in the decision model is critical to estimate the effectiveness outcomes. The probability of treatment success during the initial two years in the control group was 63.3%, which was analysed based on the population-based health big data in Korea between 2013 and 2018, so the result can be considered very valid. The probability was also similar to the published study results. In a study by Lee et al.19 involving 5,192 MDR patients diagnosed in 2011–2014, the treatment success rate was reported as 65.7%, which was consistent with this study. However, the definition of treatment success in a clinical sense may differ from this study. While this study’s definition was the completion of treatment medications for 24 months, including discontinuation of medications less than two months, the WHO defined it as follows; Cured: at least three consecutive culture tests negative every 30 days after the intensive care period. Treatment completed: the sputum smear or culture results do not meet the definition of a cure, but the treatment is completed without evidence of failure.20 However, since treatment success includes cured and treatment completed, this study’s definition of treatment success was assumed to be highly consistent with clinical treatment success.
The treatment outcomes of the control were assumed based on the analysis of real-world data, but the outcomes of the oral regimen group were assumed based on literature data on top of the results of the control group. Using the OR of treatment success according to bedaquiline administration based on a published study,6 the probability of treatment success during the initial two years was derived as 77.5% in the oral regimen group. The probability was consistent with a previously published study’s results on Korean MDR-TB patients. The treatment success rate was reported to be 79.2% if newly diagnosed MDR-TB patients in 2016–2018 were treated with new oral drugs-containing regimens.21 Meanwhile, the treatment effect and cost of delamanid were not considered in the base case. This is because bedaquiline is selected first in most patients in Korea, and if bedaquiline is not used, a delamanid prescription is allowed only if it is used to replace bedaquiline under the health insurance benefit criteria. Including bedaquiline replacement by delamanid, the base case analysis results will not change significantly considering that delamanid is not expected to affect the overall treatment outcomes, and the drug cost of delamanid (assumed 23,880 USD for the 6-month course) is similar to the cost of bedaquiline.2122
The treatment outcomes of the oral regimen group were assumed to be slightly conservative in the following two points; First, the treatment success rate seems to be further improving recently as the use of bedaquiline has been expanded to all MDR-TB patients from limited MDR-TB patients after the change in the 2020 Korean TB treatment guidelines and health insurance benefit criteria. Individualized treatment therapy has been implemented according to the recommendations of the National TB expert review committee. Second, the patient’s treatment compliance is expected to increase further if the all-oral regimens are used. As the patient’s compliance increases, the treatment success rate will increase further, and the rate of treatment failure due to lost F/U and death will decrease relatively.23
In addition to the OR of treatment success, the effectiveness variables affecting ICER results were the mortality rates of relapse and lost F/U. The ICER increased by about 20% more than the base case when applying the mortality rates based on the results of the literature data.24 However, the literature mainly dealt with TB patients rather than MDR-TB patients, and this study’s source data were updated compared with the published literature. Hence, the analysis results based on the literature data were presented only as sensitivity analysis. All other variables on effectiveness have an effect within 10% on the ICER of the base case, and the range of incremental QALY in the probabilistic analysis results was not wide; therefore, the validity of estimating the overall treatment outcomes is evaluated as high.
The control group’s cost estimation meant that all the treatment costs applied in the health insurance system were captured based on real-world data analysis. Considering that the national health insurance scheme covers most of the costs associated with MDR-TB treatment, it is estimated that the treatment cost assumed in this study will be very close to the actual cost of treatment. In contrast, the cost assumption of the oral regimen group was approached quite conservatively. Although there were cost-savings in the bedaquiline group by reducing the hospitalization days due to advancing sputum conversion days in the previous economic evaluation study on bedaquiline,1218 cost-savings due to reduced hospitalization were not included in this study. The length of the treatment regimen was assumed as a long course for all the patients in the cost assumptions, and the treatment period significantly affected the overall treatment costs.25 Currently, some patients are treated with shorter course regimen, so reflecting these clinical realities, the actual cost-effectiveness will be further improved. In the previous economic evaluation studies,12131415 some studies showed cost-saving results in the oral regimen group containing bedaquiline. However, this study estimated that the total cost was higher in the oral regimen group. The difference seems to be due to the differences in the healthcare system and medical service costs in each country and the analytic perspective of each study. The base case analysis did not reflect transportation costs, time cost, and productivity loss. When all of them were reflected, the cost-saving results were derived in the same way as other studies.13 Ultimately, the main difference in cost estimation in both groups was the cost of treatment for the first two years. The cost of bedaquiline accounted for most of the difference, and the lower death cost in the bedaquiline group reduced the cost difference between the two groups.
The limitations of this study were as follows. First, the effectiveness outcomes and cost of each health status were assumed using Korean health big data, which might differ from the definition of clinical health status. However, the definition of health status was consistently applied in both comparator groups, and the costs of the oral regimen group were estimated conservatively. The effect of these limitations on ICER is not expected to be critical. Second, the effectiveness outcome of the oral regimen group was not directly measured but assumed based on published data. Therefore, there will be a difference in the real effectiveness outcomes of current all-oral regimens. The concomitant use of linezolid in the oral regimen group has increased compared with the control group,26 but the effect of linezolid was not reflected in the estimation of effectiveness outcomes. We performed a sensitivity analysis on the concomitant use of linezolid with bedaquiline. The ICER was calculated by reflecting only the increased cost of linezolid without adjusting effectiveness outcomes from the base case because no appropriate reference was available to assume the effect of concomitant use of linezolid with bedaquiline. The ICER increase in the sensitivity analysis was not significant; thus, it is estimated that the concomitant use of bedaquiline and linezolid would also be cost-effective. However, after adopting a strategy to use all-oral drugs to treat MDR-TB, the treatment outcomes have not yet been evaluated, and a more accurate evaluation will be needed through future research. Third, the utility values of quality of life by health status will be different from the value of Koreans. The only study on the utility value of MDR-TB patients was published in Thailand. Since the quality of life of TB patients showed very variable results depending on the country of measurement and the measurement tools,1727 further studies on the quality of life of MDR-TB patients need to be conducted in the future.
In conclusion, an all-oral regimen is a cost-effective option in treating MDR-TB patients compared with injectable-containing regimens. It will contribute to patients’ return to society in a shorter time, and it is expected to be a cost-saving choice by compensating for productivity losses. Therefore, implementing WHO’s new guidelines on all-oral regimens needs to be further promoted to end TB.
 XML Download
XML Download