

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
An individual’s heart rate variability (HRV) reflects their physical health state, including autonomic nervous system stability.1 HRV also reflects one’s psychological state, as people with high levels of depression, anxiety, or stress tend to have low HRV.23 Therefore, HRV has been widely used as an objective indicator to supplement subjective evaluation of psychological states.4 However, as HRV is affected by a variety of contributing factors, careful interpretation of HRV and its clinical implications is required.5 In particular, as the baseline level of HRV varies greatly from person to person, it is necessary to assess HRV changes through repeated measurements.
Although HRV is generally measured in a resting state for a short period of time (e.g., 5 minutes) in clinical settings, the reliability of HRV measured during a short period of time is controversial.6 As an alternative to a short resting period, previous studies examined whether measuring HRV during long periods of daily activity produce clinically meaningful results.7 In particular, as an electrocardiogram (ECG) signal is easy to acquire using a wearable device, the measurement of HRV has received increasing attention with the development of digital healthcare tools.8 However, sophisticated removal of confounding effects due to movement is required to extract HRV parameters from ECG signals acquired through a wearable device. In addition, to correctly interpret 24-hour ECG, circadian rhythm should be considered.
Despite accumulating evidence of a correlation between emotional state and HRV, the relationship between emotional indicators and HRV parameters extracted from long-term ECG has not been sufficiently explored. As long-term ECG contains information that is not contained in short-term ECG (e.g., changes in HRV due to circadian rhythm), it is expected to provide novel information about the relationship between emotional state and HRV. In this study, HRV parameters were extracted from Holter monitoring data for cardiac evaluation, and the participants’ degrees of depression and anxiety symptoms were assessed based on a self-reported questionnaire. Using this approach, we investigated the characteristics of HRV extracted from long-term ECG in participants with high levels of psychological distress.
METHODS
Participants
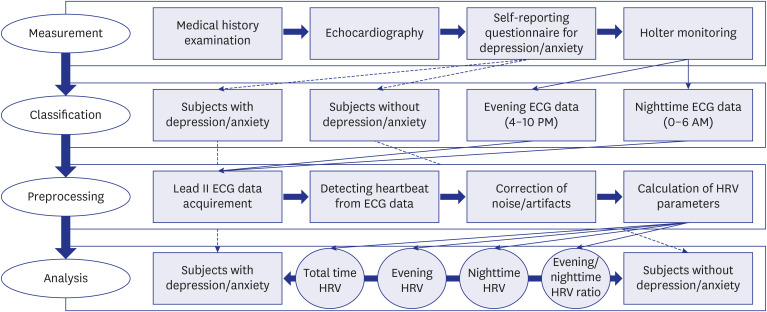
Data were collected from participants who underwent Holter monitoring for cardiac evaluation in a hospital. The overall protocol of this study is depicted in Fig. 1. The reasons for performing Holter monitoring included chest pain or discomfort, syncope or dizziness, palpitations, and suspected arrhythmias detected during health check-up. A total of 401 adults between the ages of 19 and 70 years who underwent Holter monitoring from March 2020 to April 2021 were included in this study. Participants’ medical and psychiatric histories were investigated, and participants were excluded from the analysis if they had a history of psychiatric illness or related psychopharmacology, paced rhythm, atrial fibrillation, incomplete information about medical history, or poor adherence to Holter monitoring.
Long-term ECG data were analyzed for 354 participants (224 women and 130 men; mean ± standard deviation age: 50.4 ± 13.5 years). Using a three-channel Holter device (SEER® Light Extend; GE Medical Systems, Seoul, Korea), seven electrodes were attached to the following positions: fifth intercostal space at the left axillary line, right clavicle just lateral to the sternum, fourth intercostal space at the right sternal edge, left clavicle just lateral to the sternum, sixth rib at the left mid-clavicle line, mid-sternum at the level of the clavicles, and the lower right chest wall. Only lead II data were used for HRV analysis.
Participants’ depression and anxiety levels were evaluated by the Hospital Anxiety Depression Scale (HADS).9 HADS consists of HADS-D, which measures depressive symptoms, and HADS-A, which measures anxiety symptoms. A score of 8 or higher on the HADS-D or HADS-A indicates significant symptoms. The HADS was administered to all participants so that their emotional state could be screened and, if necessary, they could consult with a psychiatrist. This study retrospectively analyzed clinical data.
HRV data processing
Either 24- or 48-hour ECG was recorded for each participant. For participants with 48-hour ECG, only the first 24 hours were analyzed. The ECG data of all subjects included a time zone from 4:00 PM to 6:00 AM the next day. To compare the most contrasting times possible, HRV analyses were performed on two different time intervals: evening (4–10 PM) and nighttime (midnight–6 AM). The middle time period from 10 PM to midnight was excluded from the analysis in consideration of the large difference of being asleep or not for each subject.
Extracted lead II ECG data were imported into the Kubios HRV Premium software (Kubios Oy, Kuopio, Finland) for data processing. Kubios HRV Premium has a built-in accurate QRS detector based on the Pan-Tompkins algorithm for detecting heartbeats from ECG.10 This detector consists of bandpass filtering of the ECG signal (to reduce noise components), squaring of the data samples (to highlight peaks), moving average filtering (to smooth close-by peaks), and decision rules including amplitude threshold and comparison to expected value between adjacent R-waves.
HRV analysis is highly sensitive to noise segments and artifacts in the ECG signal.11 Therefore, correction of artifacts before HRV analysis is crucial for the accurate determination of HRV parameters. Noise in the ECG signal typically includes baseline wander, motion artifacts, electromyographic noise, and powerline interference, and may also include missing, extra, or misaligned beat detections as well as ectopic beats, such as premature ventricular contractions or other arrhythmias.12 This study included the automatic noise detection and removal, which automatically identifies and removes noise segments in raw ECG data using “None,” “Very low,” “Low,” “Medium,” or “Strong” noise detection levels. The “Medium” level was selected in this study. Two methods for correcting artifacts in ECG data were applied: threshold-based correction, in which artifacts are simply corrected by comparing every RR interval value against a local average interval; and automatic correction, in which artifacts are detected from a time series consisting of differences between successive RR intervals.13
Various HRV parameters were calculated from the beat-detected and noise/artifact-removed ECG data. We calculated commonly used HRV parameters in the time and frequency domains. In the time domain, we used the standard deviation of all R-R intervals (standard deviation of normal-to-normal interval) and the squared root of the mean of the sum of squares of successive R-R interval differences (root mean square of successive differences). In the frequency domain, applying the fast Fourier transformation algorithm, we used power in the high frequency (HF: 0.15–0.4 Hz), power in the low frequency (LF: 0.04–0.15 Hz), power in the very low frequency (VLF: 0–0.04 Hz), and LF/HF ratio. The natural logarithm was applied to the values of VLF, LF, and HF.
Statistical analysis
Statistical analysis was conducted using the Statistical Package for the Social Sciences (SPSS) version 24.0 (IBM Corp., Armonk, NY, USA), and statistical significance was determined based on a P value < 0.05. Participants were classified based on cut-off values of 8 points for the HADS-D and HADS-A. Independent samples t-tests were used to compare the absolute values and ratios of nighttime-to-evening HRV parameters between groups. Paired samples t-tests were used to compare the nighttime and evening HRV parameters within groups.
Ethics statement
The study was conducted according to the guidelines of the Declaration of Helsinki. The current study’s protocols were approved by the Institutional Review Boards of Yongin Severance Hospital (9-2021-0082). Informed consent was waived by the board due to retrospective analysis of anonymized data obtained from routine evaluations of patients undergoing Holter monitoring.
RESULTS
Demographic and clinical characteristics
When classified based on a cut-off of 8 points on the HADS-D, there were 127 participants with depressive symptoms and 227 participants without depressive symptoms (Table 1). Compared with participants without depressive symptoms, participants with depressive symptoms had similar age but a higher proportion of females. When classified based on a cut-off of 8 points on the HADS-A, there were 95 participants with anxiety symptoms and 259 participants without anxiety symptoms (Supplementary Table 1). Compared with participants without anxiety symptoms, participants with anxiety symptoms had similar age but a higher proportion of females.
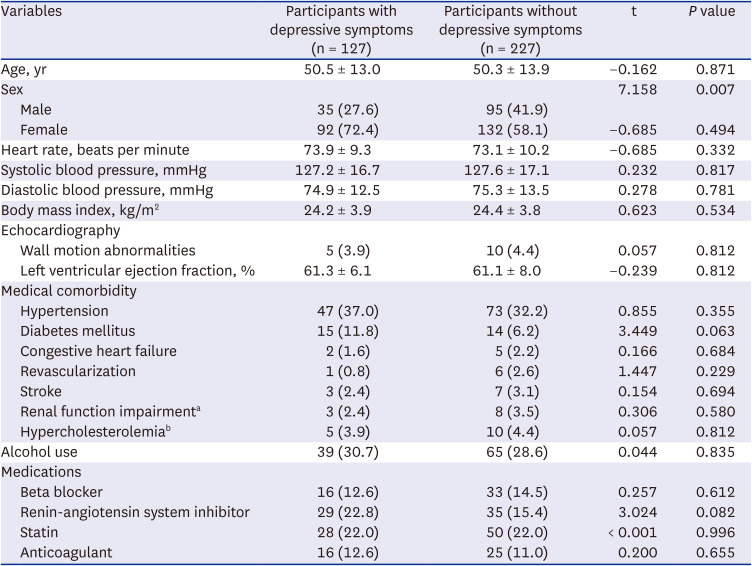
Table 1
Demographic and clinical characteristics of study subjects
Values are presented as mean ± standard deviation or number (%). Comparisons between groups were based on a cut-off of 8 points on the HADS-D.
HADS-D = Hospital Anxiety Depression Scale-Depression Subscale.
aGlomerular filtration rate < 60 mL/min.
bTotal cholesterol > 240 mg/dL.
![]()
HRV analysis
There were no significant differences in the absolute values of HRV parameters between participants with and without depressive symptoms (Table 2) or with and without anxiety symptoms (Supplementary Table 2).
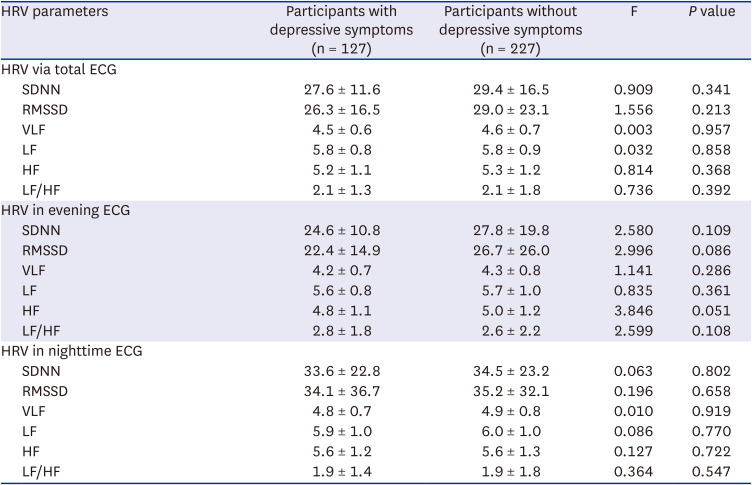
Table 2
HRV parameters
Values are presented as mean ± standard deviation. Comparisons between groups were based on a cut-off of 8 points on the HADS-D (differences in the gender ratio between groups were controlled).
HRV = heart rate variability, ECG = electrocardiogram, SDNN = standard deviation of normal-to-normal interval, RMSSD = root mean square of successive differences, VLF = very low frequency, LF = low frequency, HF = high frequency, HADS-D = Hospital Anxiety Depression Scale-Depression Subscale.
![]()
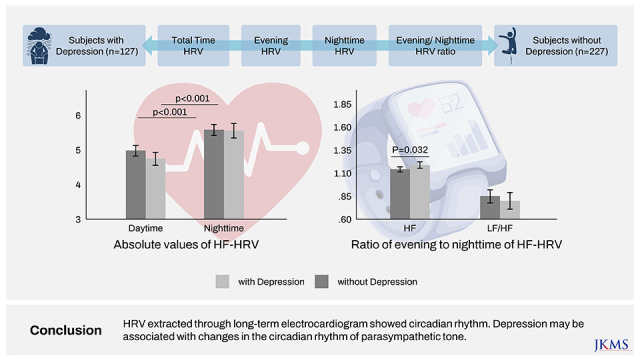
Comparison of evening and nighttime HRV in patients with and without depressive symptoms showed that nighttime HRV was significantly higher than evening HRV in both groups (Fig. 2, Table 3). Also, comparison of evening and nighttime HRV in patients with and without anxiety symptoms showed that nighttime HRV was significantly higher than evening HRV in both groups (Supplementary Table 3).

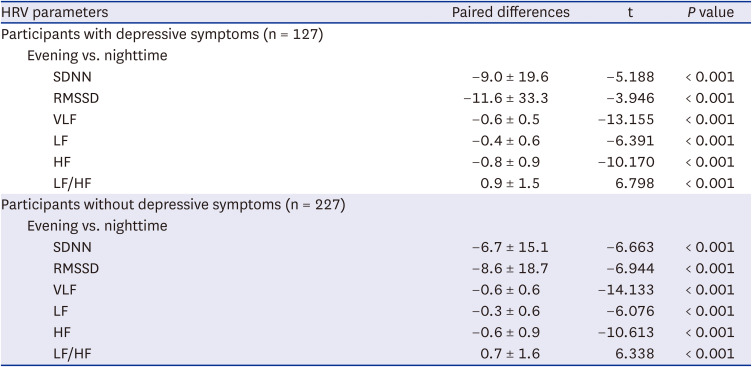
Fig. 2
Comparison of HRV parameters of evening (4–10 PM) and nighttime (midnight–6 AM) between subjects with depression (n = 127) and subjects without depression (n = 227). The 95% confidence interval is depicted.
HRV = heart rate variability, SDNN = standard deviation of normal-to-normal interval, RMSSD = root mean square of successive differences, VLF = very low frequency, LF = low frequency, HF = high frequency.
![]()
Table 3
Comparison of evening and nighttime HRV
Values are presented as mean ± standard deviation. Comparisons between groups were based on a cut-off of 8 points on the HADS-D.
HRV = heart rate variability, SDNN = standard deviation of normal-to-normal interval, RMSSD = root mean square of successive differences, VLF = very low frequency, LF = low frequency, HF = high frequency, HADS-D = Hospital Anxiety Depression Scale-Depression Subscale.
![]()
Participants with depressive symptoms showed higher ratios of nighttime-to-evening HF compared to participants without depressive symptoms (Fig. 3, Table 4). There were no significant differences in the ratios of nighttime-to-evening HRV parameters between participants with and without anxiety symptoms (Supplementary Table 4).
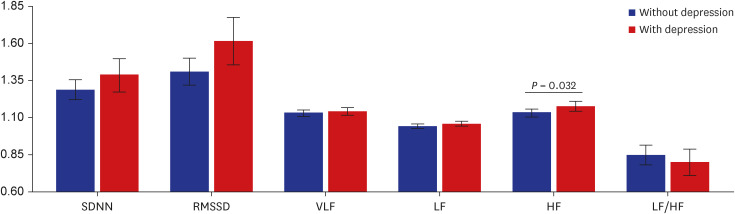
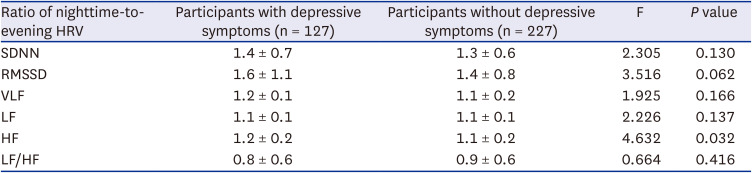
Fig. 3
Comparison of ratio of evening to nighttime in HRV parameters between subjects with depression (n = 127) and subjects without depression (n = 227). 95% confidence interval is depicted.
HRV = heart rate variability, SDNN = standard deviation of normal-to-normal interval, RMSSD = root mean square of successive differences, VLF = very low frequency, LF = low frequency, HF = high frequency.
![]()
Table 4
Ratio of nighttime-to-evening HRV
Values are presented as mean ± standard deviation. Comparisons between groups were based on a cut-off of 8 points on the HADS-D (differences in the gender ratio between groups were controlled).
HRV = heart rate variability, SDNN = standard deviation of normal-to-normal interval, RMSSD = root mean square of successive differences, VLF = very low frequency, LF = low frequency, HF = high frequency, HADS-D = Hospital Anxiety Depression Scale-Depression Subscale.
![]()
DISCUSSION
In this study, we analyzed the long-term ECG data of participants undergoing Holter monitoring and extracted HRV parameters. We also assessed the psychological distress of participants without major psychiatric history using a self-reported questionnaire, and divided participants into groups based on their degrees of depressive and anxiety symptoms. Contrary to our prediction that HRV would differ depending on the level of psychological distress, HRV parameters in long-term ECG did not differ between groups. Since this study included people without psychiatric histories, differences in HRV would not have been as noticeable as in studies comparing individuals with psychiatric disorders to healthy controls. Furthermore, HRV is affected by several intrinsic and extrinsic factors, and may be significantly influenced by medical comorbidities and medication history.14 Although we excluded participants with ECG-affecting conditions, many participants had medical comorbidities and medication histories, which could have masked potential differences between groups. Also, we did not use resting-state ECG but rather acquired long-term ECG during daily activity, which is greatly affected by physical activity.15
When we divided long-term ECG data into evening and nighttime, we found significant increases in HRV parameters at nighttime compared to evening in both high and low psychological distress groups. This was consistent with the findings of previous studies, and showed that HRV indicators exhibit circadian rhythm.16 Considering that HRV indicators are mainly influenced by parasympathetic tone,17 our results were consistent with previous studies which showed that the parasympathetic nervous system dominates at night. Based on previous findings, this increase in parasympathetic tone at nighttime is thought to be mainly due to the effect of non-rapid eye movement (NREM) sleep.18 Our results suggest that the time of day should be taken into account when interpreting HRV indicators. In addition, our results also suggest that ECG measured serially or long-term can provide useful information, such as HRV circadian rhythm, which is not included in ECG measured for a short duration at one time-point.
Participants with and without depressive symptoms differed in the degree of change in HF between evening and nighttime, with participants with depressive symptoms showing a greater change between evening and nighttime compared to participants without depressive symptoms. This result was unexpected, as it seems to conflict with previous studies showing that the circadian rhythm of HRV is more pronounced in participants with psychiatric illnesses, such as depression or anxiety.19 HF mainly reflects parasympathetic tone.20 Therefore, our results suggest that the increase in parasympathetic tone at night may be more pronounced in the presence of depressive symptoms. There are several possibilities that can explain these results. First, considering that parasympathetically modulated HRV reflects psychological stability,21 participants with depressive symptoms may show greater fluctuations in psychological factors between evening and nighttime. As another possibility, considering the characteristics of the ECG data used in this study, the differences in physical activity levels between participants with and without depressive symptoms may have influenced the results.22 The difference in sleep quality of the subjects may also have had a strong influence on the change in HRV at nighttime.2324 Future research, including a study design that considers individual differences in lifestyle factors, may provide a more appropriate framework for further investigating the relationship between psychological distress and HRV.
This study had several important limitations. First, the classification of the time zone used in this study had no prior evidence, and was based on the time range available to all subjects who received Holter monitoring. In addition, there was a limitation in evaluating the overall circadian rhythm since it did not include crucial time zones, such as morning or early afternoon. Second, in this study, the group with high psychological distress had a higher proportion of female subjects. Gender is one of the major confounders that can influence HRV.2526 Although gender was included as a covariate in the comparison between groups in this study, the effect of gender could not be sufficiently excluded. Therefore, further research on subjects matched by major demographic variables, such as age and gender, are required. Third, although we included participants with a wide age range and various physical conditions, the number of participants was too small to fully consider the influence of demographic characteristics and comorbid physical conditions. Fourth, we extracted HRV from ECG data acquired during the daily life of participants. Although we attempted to remove noise in the signal caused by physical activity, it may have still had a large presence and influence on the results. In addition, the participants’ internal and external stresses, life events, and living environment during Holter device monitoring could have influenced HRV. If HRV based on ECG measured in a resting state would have also been included, this would have provided useful reference information. Fifth, this retrospective study evaluated the psychological distress of participants based on a self-reported questionnaire assessing depression and anxiety symptoms, and did not thoroughly evaluate their emotional state through a structured clinical interview.
Despite these limitations, the results of this study have important implications for the use of HRV indicators to reflect emotional states. HRV has shown prominent circadian rhythm, with different patterns of changes between evening and nighttime depending on the degree of depressive symptoms. Our investigation of the relationship between HRV based on long-term ECG data and psychological state suggests the clinical applicability of HRV parameters extracted from ECG acquired with a wearable device. Moreover, HRV parameters extracted through long-term ECG during daily life may contain different psychometric information than those extracted through short-term ECG in a resting state.
 XML Download
XML Download