

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 outbreak began in Wuhan, China, in December 2019, and was declared a pandemic on March 11, 2020, by the World Health Organization.1 Due to its rapid dissemination and lack of effective treatment, the importance of vaccination has been highlighted. Several vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have been developed and approved after phase III randomized trials that have demonstrated each vaccine’s efficacy and safety.2345 However, as the vaccines are being widely used, some unexpected adverse events have been reported in real-world practice.6
Neuralgic amyotrophy is a rare inflammatory and idiopathic neuropathy occasionally associated with vaccination.78 Although the classic phenotype is brachial plexopathy, neuralgic amyotrophy can also manifest in the involvement of other nerves, such as the lumbosacral plexus or phrenic nerve.9 To our knowledge, there has been only one previous report on phrenic neuropathy following SARS-CoV-2 vaccination.10 The diaphragm is the principal respiratory muscle, and its weakness can disrupt vital respiratory function. Diaphragmatic dysfunction can be unilateral or bilateral, with the latter being associated with more severe respiratory symptoms. Here, we present a patient who developed unilateral diaphragmatic dysfunction as a manifestation of neuralgic amyotrophy after SARS-CoV-2 vaccination.
CASE DESCRIPTION
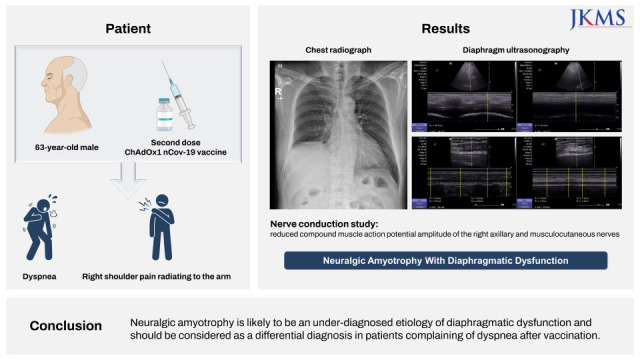
A 63-year-old man presented to our hospital with dyspnea and an abnormal chest radiograph. He reported prior vaccination with two doses of ChAdOx1 nCoV-19 (Oxford/AstraZeneca, Cambridge, UK). After receiving the first dose, he developed dyspnea which improved over subsequent weeks. Within a week following receipt of the second dose which was one month before visiting the hospital, he re-developed dyspnea at a degree worse than what he had experienced after the first dose. Simultaneously, he developed right shoulder pain radiating to the right arm. Chest radiography revealed right hemidiaphragm elevation which was absent on a chest radiograph taken one month before the second dose of vaccination (Fig. 1).
Fig. 1
Chest radiograph images of the case patient (A) one month before vaccination and (B) one month after vaccination. Elevation of the right hemidiaphragm is noted after vaccination.

The patient had been prescribed aspirin, fimasartan, amlodipine, and rosuvastatin for hypertension and hyperlipidemia. He denied recent chest trauma, cardiothoracic procedures, or surgery. He was a former smoker with a smoking history of 20 pack-years. His body mass index was 26 kg/m2. Neurological examination did not reveal any motor or sensory deficits. Spirometry performed at the time of the first visit showed a restrictive pattern with a forced vital capacity (FVC) of 2.64 L (72% of the predicted value [%pred.]) and a forced expiratory volume in 1 second (FEV1) of 1.90 L (72%pred.). He underwent a chest computed tomography scan, and no abnormal findings were observed, except for an elevated right hemidiaphragm.
After four months, the dyspnea and shoulder pain did not improve. Repeated pulmonary function tests in the supine position showed an FVC of 1.44 L (41%pred.) and FEV1 of 1.12 L (40%pred.), with a decrease of 42% and 40% respectively, compared to an FVC of 2.47 L (69%pred.) and FEV1 of 1.88 L (67%pred.) in the upright position. Diaphragm ultrasonography revealed left and right diaphragmatic excursions of 38.7 and 15.3 mm, respectively, during forceful breathing (Supplementary Fig. 1). The right diaphragmatic thickness was 1.5 mm at end-inspiration and 1.3 mm at end-expiration (thickening fraction 15%), while that of the left diaphragm was 3.2 mm at end-inspiration and 2.0 mm at end-expiration (thickening fraction 60%), as shown in Supplementary Fig. 2. Based on these findings, his condition was diagnosed as diaphragmatic dysfunction, and causality with prior vaccination could not be excluded given no other apparent cause except for the temporal relationship with vaccination.
Owing to the presence of shoulder pain and documented diaphragm dysfunction, neuralgic amyotrophy was suspected. Electrophysiological studies demonstrated reduced compound muscle action potential amplitude of the right axillary and musculocutaneous nerves, with normal medial, ulnar, and radial nerves. These findings suggested right upper brachial plexopathy. Therefore, diaphragmatic dysfunction in the current patient was considered secondary to neuralgic amyotrophy following SARS-CoV-2 vaccination. Analgesics were given to manage the shoulder pain. As there was no evidence of hypoventilation or sleep disturbance that may require noninvasive ventilation, the patient was followed with conservative treatment. At follow-up 8 months after symptom onset, the patient reported a significant reduction in shoulder pain and slight improvement in dyspnea. Regular follow-up is planned until recovery of the diaphragmatic dysfunction.
DISCUSSION
Diaphragmatic dysfunction following SARS-CoV-2 vaccination has rarely been reported. In this report, the patient was diagnosed with unilateral diaphragm dysfunction through pulmonary function tests, chest imaging, and diaphragm ultrasonography. Plausible causes of the diaphragmatic dysfunction, other than vaccination, were not identified. Considering the ipsilateral brachial plexopathy, which also occurred following vaccination, we diagnosed the patient with neuralgic amyotrophy with prominent unilateral diaphragmatic dysfunction.
Neuralgic amyotrophy, also known as Parsonage–Turner syndrome, is an idiopathic neuropathy that commonly affects the brachial plexus. This syndrome is typically characterized by acute-onset neuropathic pain in the shoulder or upper extremities, followed by varying degrees of weakness and atrophy of the associated muscles. Although recognized, phrenic nerve involvement is rare in neuralgic amyotrophy.111213 According to an observational study by van Alfen et al.,14 the incidence of phrenic neuropathy in patients with neuralgic amyotrophy was 7.6%.
The pathophysiology of neuralgic amyotrophy is not well understood; however, interactions between environmental factors and individual susceptibility are important. Infections and immune-related factors including vaccinations have been reported to trigger neuralgic amyotrophy. SARS-CoV-2 infection and vaccination have been reported as antecedent events to neuralgic amyotrophy.1516 However, cases involving diaphragmatic dysfunction are rare, and to our knowledge, only one other case has been reported in literature.10 In that report, the patient developed intense shoulder pain four days after Vaxzevria vaccine (AstraZeneca) administration, which led to the diagnosis of neuralgic amyotrophy. The patient received corticosteroid treatment but subsequently developed ipsilateral diaphragm dysfunction approximately 40 days following vaccination.
As most patients with neuralgic amyotrophy develop severe neuropathic pain, adequate analgesic treatment is usually required. Although no randomized controlled trials to date have examined this issue, immunomodulatory treatment with corticosteroid or intravenous immunoglobulin has been attempted in several case reports and case series due to the possible immune-mediated nature of the disease. The administration of high-dose corticosteroid within the first month of onset may reduce the pain duration and improve functional recovery.1 However, treatment started beyond 2 weeks after symptom onset is not expected to be effective and chronic treatment is not warranted. In our patient, the diagnosis was made several months after the disease onset; thus, corticosteroid treatment was not given.
Treatment of diaphragmatic dysfunction is primarily supportive. Noninvasive ventilation is indicated for severe orthopnea, hypoventilation, or sleep disturbances. The prognosis of neuralgic amyotrophy without diaphragmatic involvement is favorable, with a recovery rate of nearly 90% within 3 years.17 In cases of diaphragmatic dysfunction, a moderate degree of spontaneous recovery is expected in most patients,1314 but the duration of phrenic nerve recovery in neuralgic amyotrophy is typically much longer than in other involved nerves.1118 Hughes et al.18 assessed diaphragm strength in patients who had previously been diagnosed with neuralgic amyotrophy and bilateral diaphragmatic dysfunction. Among the 14 study patients, 10 showed some evidence of improvement and the recovery took more than 3 years. It is not well understood why the recovery rate of diaphragmatic dysfunction is slow, but it may be due to a greater severity of immune-mediated attacks on phrenic nerves compared to other nerves, or the low intrinsic ability of phrenic nerves to recover.19 Since recovery is prolonged, waiting for a sufficient period is recommended before considering invasive interventions such as surgical plication.
The present case is a rare incidence of diaphragmatic dysfunction secondary to neuralgic amyotrophy following the SARS-CoV-2 vaccination and is thought to be the first such case report in South Korea. Although rare, neuralgic amyotrophy may be encountered more frequently when an entire population is encouraged to get vaccinated. Neuralgic amyotrophy is an under-diagnosed etiology of diaphragmatic dysfunction and should be considered as a differential diagnosis in patients complaining of dyspnea following vaccination.
 XML Download
XML Download