

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic, which has led to 2,610,925 deaths globally since its emergence at the end of 2019, has a reported mortality of 2.2% [1]. As of March 2021, COVID-19 has been responsible for 213,020 deaths, with a mortality of 9.9%, in Mexico, which is among the top 10 countries with high COVID-19 mortality rates [12]. On the other hand, COVID-19 mortality is between 6% and 10% in patients with cardiovascular and chronic respiratory tract diseases, diabetes mellitus (DM), and hypertension [3].
Serum vitamin D level has been identified as a poor prognostic factor in COVID-19. An observational study from Europe which analyzed the vitamin D status in older adults with COVID-19 reported that countries with greater exposure to sunlight such as Spain and Italy, which have the highest rates of COVID-19 and mortality, had high rates of vitamin D deficiency [4]. In contrast, high-latitude countries of Norway, Finland, and Sweden, which receive less ultraviolet-B sunlight than southern Europe, had low rates of vitamin D deficiency and, specifically in Norway and Finland, lower rates of COVID-19 and associated mortality. The study also showed a significant correlation between 25-hydroxyvitamin D (25[OH]D) and mortality rate (P = 0.046) [4]. This counterintuitive finding, i.e., the higher vitamin D deficiency in European countries with greater sun exposure compared with the lower vitamin D deficiency in high-latitude European countries with less sun exposure, may be explained by the consistently higher consumption of fatty fish, vitamin D fortification of food, and vitamin D supplementation in countries with low sun exposure [5]. In the Americas, high rates (up to 77%) of vitamin D deficiency have been reported [6], and, specifically in Mexico, as a country, the prevalence of vitamin D low levels has been reported to be 30%, being higher in Mexico City (43.1%) [7].
It is known that vitamin D is involved in innate and adaptive immunity; one mechanism is by boosting the defenses of the mucous membranes and attenuating excessive inflammation, which may explain the role of vitamin D in acute infections [8]. Vitamin D induces the gene encoding the antimicrobial peptide LL-37 [9]; this peptide has antiviral capacity against a number of viruses, including influenza-virus [10].
Several studies reported that between 59% and 74% of patients hospitalized with COVID-19 had vitamin D deficiency and that the rate of vitamin D deficiency was higher in those with torpid evolution [111213]. Considering the high mortality rates of COVID-19 in Latin American countries, together with multiple factors that increase the prevalence of vitamin D deficiency, it is critical to determine the role of vitamin D deficiency in the prognosis of patients with COVID-19. Therefore, the present study aimed to determine the vitamin D status and evaluate the association of 25(OH)D levels with mortality in patients with critical COVID-19.
SUBJECTS AND METHODS
Study design
This prospective, observational study included adult patients treated for critical COVID-19 between May 1, 2020 to November 30, 2020 in Hospital #48 of the Instituto Mexicano del Seguro Social in Mexico City. Critical COVID-19 was defined as the presence of respiratory failure and the need for mechanical ventilation, shock, or other organ failure requiring admission to intensive care unit (ICU). Patients without available 25(OH)D or albumin values and those with a clinical presentation compatible with COVID-19 who did not have a positive real-time polymerase chain reaction (RT-PCR)-based test for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) were excluded from the study. All patients were followed until hospital discharge or in-hospital death.
For all patients, data on the following clinical characteristics and risk factors were obtained from the clinical records: body mass index (BMI), obesity (BMI ≥ 30), hypertension, diabetes mellitus type 2 (DM2), chronic obstructive pulmonary disease, chronic kidney disease, congestive heart failure, peripheral venous insufficiency, and smoking.
In all patients, blood samples were collected at the time of ICU admission to measure 25(OH)D and albumin levels. Serum albumin levels < 3.5 g/dL were defined as hypoalbuminemia. Serum 25(OH)D levels of < 20 and 20–29.99 ng/mL were defined as vitamin D deficiency and vitamin D insufficiency, respectively, whereas a serum 25(OH)D level > 30 ng/mL was defined as normal vitamin D status [14].
Laboratory assays
In the present study, 25(OH)D levels were determined using chemiluminescence on the Architect i1000 platform (Abbott Diagnostics, Abbott Park, IL, USA) and albumin levels were determined by colorimetric enzymatic methods (Dimension Integrated Chemistry System, Erlangen, Germany) in the clinical laboratory of the Hospital Infantil de México Federico Gómez.
The presence of SARS-CoV2 was determined by RT-PCR in accordance with the standardized guidelines for Laboratory Epidemiological Surveillance of COVID-19 (Supplementary Material 1) (Dirección General de Epidemiología, 2020).
Statistical analysis
For quantitative variables, the Kolmogorov-Smirnov test was performed to evaluate the normality of the distribution of data, and data with non-normal distribution were presented as medians with 95% confidence intervals (CIs). Qualitative variables were presented as proportions and frequencies. The patients were divided into surviving and deceased patient groups. Comparisons between the 2 groups were performed using the Mann-Whitney U test for quantitative variables and the χ2 or Fisher's exact test for qualitative variables. Multiple logistic regression analysis was performed to assess the association between 25(OH)D levels, albumin levels and death after adjustment for age, sex and BMI. It should be noted that chronic obstructive pulmonary disease, chronic kidney disease, congestive heart failure, peripheral venous insufficiency, and smoking were grouped into “risk factors,” given the low frequency of cases with these conditions. STATA v.12.0 (Stata Corp., College Station, TX, USA) was used for all statistical analyses.
Ethical consideration
According to the Declaration of Helsinki, the protocol was evaluated and approved by the National Research and Health Ethics Committee of the Mexican Social Security Institute (registry number, R-2020-785-090) and the Research and Health Ethics Committee of the Hospital Infantil de Mexico Federico Gómez (registry number, HIM-2020-045). Written informed consent was obtained from all patients or their legal guardians.
RESULTS
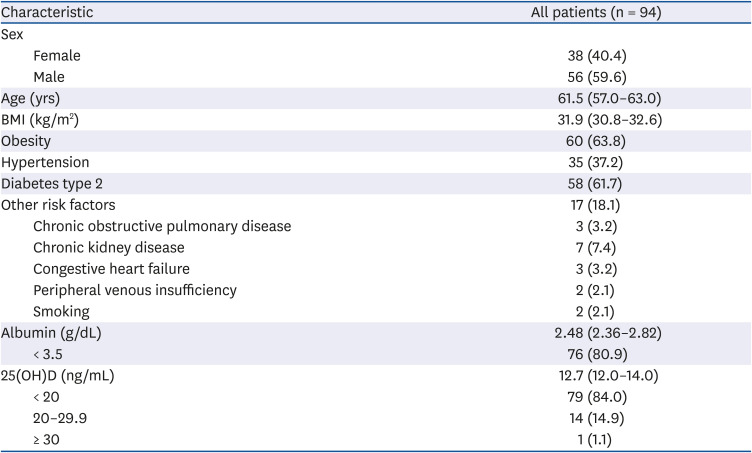
Among a total of 104 patients with critical COVID-19 who were admitted during the study period, serum 25(OH)D levels were not determined at the time of admission in 10 patients; therefore, the study cohort comprised 94 patients (Table 1). The median age was 61.5 years, with a male predominance (59.6%). There was a high frequency of obesity (63.8%), DM2 (61.7%) and hypertension (37.2%). Only 8 patients (8.5%) did not have any risk factors.
Table 1
Demographic and clinical characteristics and serum 25(OH)D levels of all patients
In total, 63 patients (67%) died during the study period. The deceased patients were significantly older than the surviving patients (65 vs. 53 years, P > 0.001). The deceased patients with critical COVID-19 had significantly higher BMI compared to the surviving patients with critical COVID-19 (33.4 vs. 30.8 kg/m2, P > 0.001; Fig. 1, Table 2).
Fig. 1
Comparison of age, BMI, and 25(OH)D level between the deceased and surviving patients with coronavirus disease 2019. (A) Age, (B) BMI, and (C) 25(OH)D.
Values are presented as median (95% confidence interval).
BMI, body mass index; 25(OH)D, 25-hydroxyvitamin D.
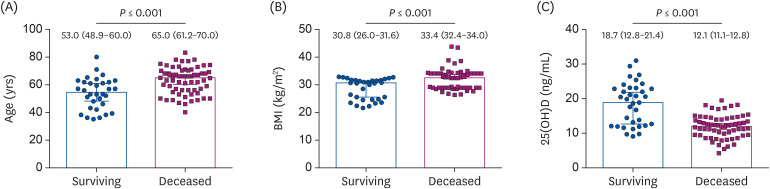
Table 2
Demographic and clinical characteristics between the deceased and surviving patients with COVID-19
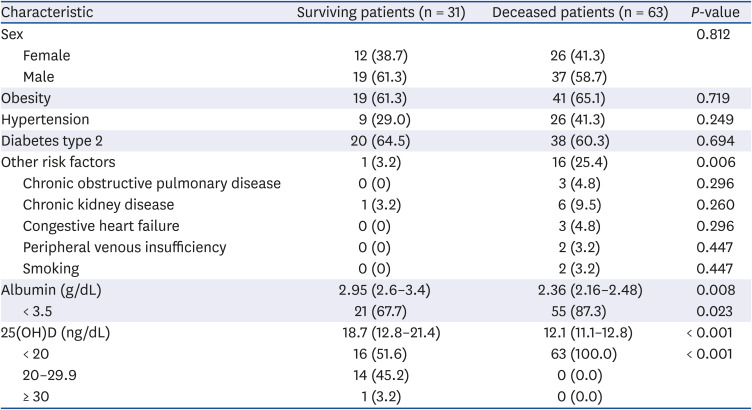
Values are presented as number of patients (%) or median (95% confidence interval). Comparisons between the 2 groups were performed using the Mann-Whitney U test for quantitative variables and the χ2 or Fisher's exact test for qualitative variables.
COVID-19, coronavirus disease 2019; 25(OH)D, 25-hydroxyvitamin D.
The median 25(OH)D level was 12.7 ng/mL in the overall cohort. There were 15 (16%) and 79 (84%) patients with vitamin D insufficiency and vitamin D deficiency, respectively, and none of the patients in the entire study cohort had serum 25(OH)D levels within the normal limits (Table 1).
The median serum 25(OH)D and albumin level were significantly lower in the deceased patients than in the surviving patients (median 25[OH]D, 12.1 vs. 18.7 ng/mL, P < 0.001 and median albumin, 2.36 vs 2.95 g/dL, P = 0.008, respectively; Fig. 1, Table 2). Additionally, the rate of vitamin D deficiency was significantly higher in the deceased patients than in the surviving patients (100% vs. 51.6%, P < 0.001; Table 2).
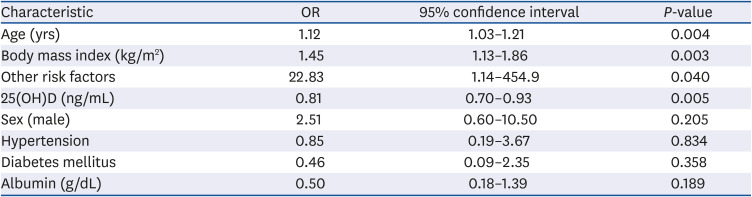
The multivariate logistic regression analysis revealed that older age, higher BMI and the presence of other risk factors were associated with mortality, while higher levels of 25(OH)D were a protective factor for mortality in patients with critical COVID-19 (Table 3). As also shown in Table 3, hypertension, diabetes, and albumin levels were not identified as prognostic factors.
Table 3
Multivariate logistic regression analysis for independent predictors of in-hospital mortality (n = 94)
DISCUSSION
In this prospective study conducted in a single institution in Mexico City, we found that the rate of vitamin D deficiency was high in patients with critical COVID-19 and that none of the 94 patients included in the study had normal vitamin D levels. Importantly, we found that a significantly higher rate of the deceased patients had vitamin D deficiency compared with the surviving patients (100% vs. 51.6%).
Vitamin D is associated with reduced risk of respiratory tract infections through several pathways. First, vitamin D plays a role in the maintenance of tight cell junctions by acting as a physical barrier. In addition, vitamin D is involved in innate cellular response by eliminating viruses through the production of β2-defensin and cathelicidin by macrophages, monocyte and keratinocytes, which increases their antimicrobial activity [15]. Furthermore, in the respiratory tract, CYP27B1 (via 1-alpha hydroxylase, the final activation of vitamin D) [16] is expressed in bronchial epithelial cells and induced by inflammatory stimuli, producing the LL37 peptide. This antimicrobial peptide may be activated locally upon infection, which further suggests a role for vitamin D in host defense [17]. Thus, it is not surprising that vitamin D insufficiency, not necessarily deficiency, increases susceptibility to bacterial and viral infections [181920].
Importantly, the present study also revealed that none of the patients had vitamin D levels within the normal limits. Studies have previously reported high prevalence rates of vitamin D deficiency in Latin American countries [21], including Mexico [22]. Additionally, studies have suggested additional factors other than high-latitude might predispose individuals in tropical countries to vitamin D deficiency despite sufficient sunlight [23]. For example, dark skin, use of sunscreen, and pollution affect the synthesis of vitamin D3 in the skin [2425] whereas low vitamin D intake, obesity, and advanced age reduce the bioavailability of 25(OH)D [2627]. A recent study in Mexico City demonstrated a positive relationship between pollution and COVID-19 mortality, which was significantly increased with age and appeared to be primarily driven by long- rather than short-term exposure [28]. This finding might be related to the high frequency of vitamin D deficiency observed in the present study, in addition to the chronic diseases, such as DM, obesity and hypertension, which are closely related to vitamin D deficiency, also observed in the present study [29]. Likewise, we also found that the COVID-19 mortality rate increased with increasing patient age. This finding, consistent with previous studies [3031], might be related to the increasing incidence of chronic diseases with age, which can worsen COVID-19 complications. Additionally, chronic diseases and advanced age both contribute to reduced 25(OH)D bioavailability [32].
It has already been described that hypoalbuminemia is a risk factor for mortality in patients with critical COVID-19 [33], which was also observed in this study (Table 2) (67.7% vs. 87.3% P = 0.023); however, in the multivariate analysis it was not demonstrated, this may be due to the sample size.
In addition to clinical evidence showing the potential detrimental effect of vitamin D deficiency on upper respiratory tract viral infections, experimental evidence supports the antiviral and immunity-boosting roles of vitamin D, with studies evaluating the association of vitamin D with mortality in patients with COVID-19 [34]. In the present study, vitamin D deficiency was present in 84% of all patients and 100% of deceased patients, consistent with previous studies [123536]. For example, in their study of 30 patients with COVID-19 who required ICU admission, Vassiliou et al. [35] reported that 80% of the patients had vitamin D deficiency and that none of the cohort patients had normal vitamin D levels, in agreement with our findings; the authors found that the rate of deceased patients was higher among those with vitamin D levels < 15.2 ng/mL. De Smet et al. [12] analyzed 186 patients hospitalized for COVID-19 with unknown disease severity and found that 59% of the patients had vitamin D deficiency at the time of admission; the authors also reported that vitamin D deficiency at the time of admission was associated with increased COVID-19 mortality (odds ratio, 3.87). Finally, in a retrospective study of 149 patients hospitalized for COVID-19, including 102 patients with severe COVID-19, Karahan and Katkat [11] found that 93.1% of the patients had vitamin D deficiency and that serum 25(OH)D levels were independently associated with increased mortality.
Vitamin D interacts with the renin-angiotensin system, a route utilized for entry by SARS-CoV-2, which interacts with angiotensin converting enzyme receptors [37]. Likewise, increased renin activity, higher angiotensin II concentrations, and higher renin-angiotensin system activity has been shown to result from low vitamin D concentrations [38].
There is not enough evidence to show that vitamin D supplementation improves the evolution of respiratory tract viral infections; however, several studies have shown that vitamin D supplementation prevents respiratory tract viral infections in populations with vitamin D deficiency [39]. Therefore, randomized controlled clinical trials should be considered to evaluate whether vitamin D supplementation in populations at risk for vitamin D deficiency prevents the development of severe disease and death in patients with COVID-19.
In the present study, one major limitation was the inclusion of only patients with critical COVID-19, which might explain the higher mortality and greater vitamin D deficiency rates observed in the study, compared to other studies. In addition, the sample size was relatively small.
In conclusion, vitamin D deficiency was present in 84% of patients with critical COVID-19 and 100% of deceased patients with COVID-19 and vitamin D deficiency. Older age, high BMI, presence of other risk factors were associated with increased mortality and, higher 25(OH)D level were associated with decreased mortality in patients with critical COVID-19.
 XML Download
XML Download