

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
As the population grows and ages, the burden of diseases and the demand for medical services are expected to gradually increase,12 which will also lead to an increased demand for healthcare professionals such as physicians and nurses. To respond to this need, the supply of health workers may need to be expanded, but it is also important to help existing health workers maintain their health and productivity.34 In particular, the health of medical professionals must be maintained for the sake of patient safety since the mental health of medical professionals is related to the safe provision of quality medical care.56
Prior studies have shown that physicians' burnout is associated with increased rates of substance abuse, suicide, and medical malpractice lawsuits.789 In addition, about 25% of physicians reported feeling depressed for two weeks and having a poor work-life balance.10 The impact of burnout also extends to nurses, who may complain of more physical pain, such as musculoskeletal pain, and work-related stress and depression than physicians.1112 In addition, nurses were reported to have a higher prevalence of migraines, cancer, gastrointestinal disease, and thyroid disease than other occupational groups.13 Therefore, the health problems of medical professionals should be considered by occupational type and medical institutional type since they vary greatly depending on the working conditions.1415
Reducing health problems for medical professionals starts with a proper assessment of their health-related quality of life. Various measurement tools have been developed and utilized to measure negative health conditions, such as depression and the second victim experience, as well as medical professionals’ burnout.16 In addition, several measurement tools related to positive health conditions such as well-being and quality of life, resilience, and mindfulness have been developed and used.17 However, the health-related quality of life of medical professionals is a complex issue, for which a standardized evaluation approach has yet to be established.17 In addition, since health professionals are often exposed to patients who are in poorer health than their own, they may perceive their health or health-related quality of life overly positively.11 Therefore, caution should be exercised when measuring the health level of medical professionals.
An in-depth study is needed to examine how medical professionals perceive their health-related quality of life, how they measure and evaluate health-related quality of life, and how to improve their health-related quality of life. Therefore, rather than administering simple surveys to identify medical professionals' health problems, this study utilized a qualitative research methodology to elicit the in-depth opinions of medical professionals regarding their health-related quality of life. Accordingly, this study attempted to provide evidence for measuring and improving the quality of health-related life for medical professionals. The focus group discussion (FGD) was conducted with physicians and nurses in Korea to identify their perceptions of the health-related quality of life of medical professionals and explore ways to measure their quality of life accurately.
METHODS
This study aimed to examine perceptions of subjective health and well-being and identify the opinions about health-related quality of life measurement tools by conducting FGDs with medical professionals. The research method for the FGD is described below in detail based on the “Consolidated criteria for reporting qualitative research”.18
Research team
The research team consisted of two researchers from the analysis team and five researchers from the audit team. The analysis team consisted of a preventive medicine specialist and a preventive medicine doctoral student, both of whom have experience in writing a thesis using qualitative research methodology, attending qualitative research seminars, and teaching qualitative research. Two researchers of the audit team have participated in qualitative research studies as lead authors, and three have considerable experience in the preventive medicine field related to this research topic.
Research participants
The researchers expected the theme of the study would be less likely to reflect their intentions since the purpose of the study was to provide participants' personal experiences and opinions on various survey tools. Accordingly, research participants were selected upon the recommendation of researchers and advisors. The criteria for selecting participants were: first, they did not have a deficit in communication skills; second, people who believed that their health-related quality of life experience as medical professionals could be fully revealed. The researchers tried to recruit various participants in terms of work experience and the size of their affiliated medical institutions. The final participants were 18 medical professionals (12 physicians and 6 nurses) who voluntarily agreed to participate after the research purpose was explained to them.
Conducting FGD
An FGD, in which several people talk on the same subject, has the advantage of revealing multiple experiences of participants due to the dynamic nature of the process, and at the same time has the disadvantage of not being able to richly capture the personal experiences of all participants.19 In order to supplement the shortcomings of FGD, this study divided medical professionals into three groups (large hospital physicians, self-employed physicians, and nurses), thereby limiting the variability in the occupational group and workplace so that the rich stories of all participants could be revealed. FGDs were conducted by a skilled moderator from a professional research firm. The preliminary guidelines for the FGDs were developed based on a review of previous studies and discussions among researchers on the analysis team. Afterward, the guidelines were reviewed by one researcher from the audit team and confirmed without modification.
The FGD guidelines consisted of three main topics: first, the perceptions of health and quality of life; second, the perceptions of health and quality of life by medical professionals; and third, opinions on health-related quality of life measurement tools (Supplementary Data 1). Specifically, for the perceptions of health and quality of life, we asked for participants' opinions on the concept of general health and the health definition of the World Health Organization (WHO). For the perceptions of health and quality of life by medical professionals, we asked participants for their opinions on factors affecting the quality of life for medical professionals, their perception of burnout, and the need to measure the quality of life for medical professionals. Finally, for opinions on health-related quality of life measurement tools, we gave participants a brief description for each of three tools and then asked for their input on the tool, including factors that would influence responses and dimensions and items in need of improvement.
The health-related quality of life surveys provided to participants included the Well-Being Index, 5-level EuroQol-5D (EQ-5D-5L) & EuroQol Visual Analogue Scale (EQ-VAS), and Health-related Quality of Life Instrument with 8 Items (HINT-8) (Supplementary Data 2). The Well-Being Index is a questionnaire developed for medical workers in the United States that consists of nine questions for both physicians and nurses.20 Since a Korean questionnaire tool does not yet exist, the US questionnaire development team approved the development of a Korean questionnaire tool and the researchers translated the questions into Korean under the supervision of the National Institute of Korean Language. The Korean-English translation company reverse translated the tool, which received final approval from the Mayo Clinic before it was shown to participants. The EQ-5D-5L is a questionnaire developed by the EuroQol Group that consists of five areas: mobility, self-management, daily activities, pain and discomfort, anxiety, and depression.21 The EQ-VAS provides a quantitative measure of subjective health outcomes through a vertical visual analog scale with consecutive numbers ranging from 0 to 100. Respondents check their own health status, with a score of 0 meaning ‘the worst imaginable health status’ and a score of 100 meaning ‘the best imaginable health status’.22 Finally, the Korean version of the HINT-8 is a health-related quality of life measurement tool developed by the Korea Centers for Disease Control & Prevention for use in the Korea National Health and Nutrition Examination Survey. Respondents' health status is measured for a week using eight items (stair climbing, pain level, strength level, degree of difficulty in performing the duties, depression level, degree of difficulty in remembering, degree of difficulty in sleeping, and happiness level), and four response scales are provided for each item.23
Analysis
Transcribed data were analyzed by content analysis, which extracts patterns from content by contrasting and comparing excerpts of the original data.24 Code analysis and consensus were conducted in three stages. Researcher A of the analysis team read the transcriptions of the FGDs more than three times and summarized words thought to be meaningful into brief sentences in order to extract the codes. Afterward, researcher B of the analysis team reviewed the codes derived by researcher A. When disagreement occurred or additional codes were created, the two researchers engaged in a discussion to reach an agreement. After the final codes were determined for the three FGDs, categorization was carried out. The categorization took place in three steps: 1) roughly classifying similar codes to execute subject grouping, 2) deriving detailed category names within subject groupings, 3) constructing upper categories through relevance and rearrangement of detailed category names derived for each subject. Subsequently, researcher B of the analysis team reviewed and revised the category table created from the third step of the categorization by researcher A. Finally, after confirming the audit team agreed with the decisions made by the analysis team, the category table was finalized.
Research validity assessment
The four evaluation criteria (truth value, applicability, consistency, and neutrality) proposed by Guba & Lincoln (1981) were used to ensure the rigor of the analysis and results.2526 First, the researchers repeatedly checked whether the transcribed data of the participants' meetings were consistent with the research results. When the participant's language was included in the results, peer review was continuously conducted to prevent the meaning from being altered and ensure the original meaning of the text was preserved. Second, we sought to ensure the “applicability” of the data by asking about the relevance of the FGDs data in contexts other than the research context. In order to ensure the applicability of the data, it is necessary to reach saturation of the data.19 The researchers conducted FGDs with three groups and continued the interview until no further information was elicited from each group. Third, in order to ensure the consistency of the responses, i.e., the responses would be similar if we asked the questions of different subjects working in similar conditions, additional medical professionals reviewed the results of analysis. Two nurses and one physician, who did not participate in the FGDs but met the selection criteria, ensure that the results of analysis were consistent with their experiences and knowledge. Fourth, “neutrality” indicates that the research findings were derived from the research participants, and not from the researcher's bias, motivation, or perspective. Neutrality can be guaranteed if the research methods and analytical procedures are specifically described, and the researchers work continuously to rule out their biases. The researchers made a conscious effort to share their prejudices and preconceptions of the study with each other and exclude prejudice and preconception in the analysis process.
RESULTS
Socio-demographic information
There were a total of 18 participants in the study. The nurse group comprised six participants with an average career length of 10 years, and all were employed in large hospitals except one. The group of specialists and residents of a university hospital included seven participants with an average career length of 13 years. The self-employed physician group included five participants with an average career length of 17 years. Participant characteristics are displayed in Table 1.
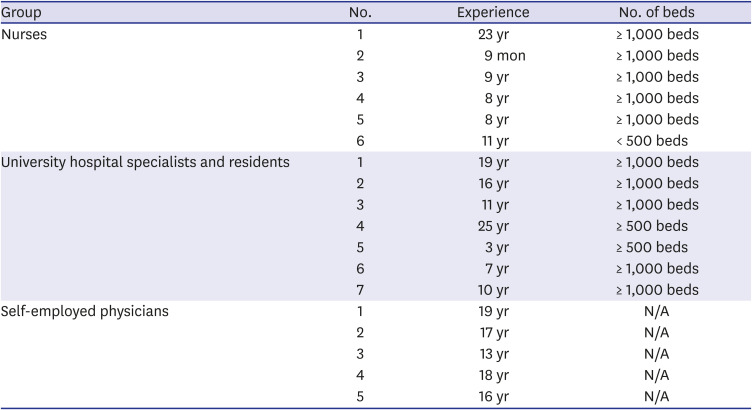
Table 1
Socio-demographic characteristics of participants
![]()
Analysis results
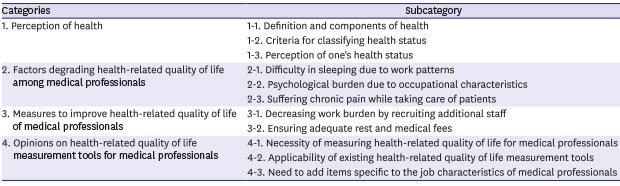
A total of 406 codes were derived as a result of analyzing the transcribed data of the three FGDs. As a result of the categorization, 11 sub-categories and 4 upper categories (perception of health, factors degrading the health-related quality of life among medical professionals, measures to improve health-related quality of life of medical professionals, opinions on health-related quality of life measurement tools for medical professionals) were derived. The details of each category are described in Table 2.
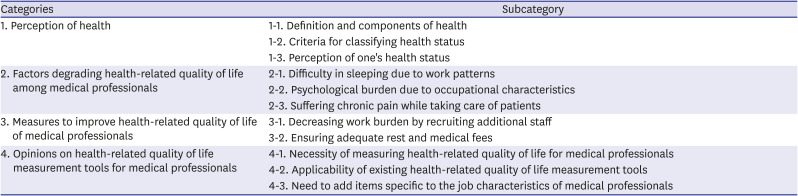
Table 2
Category table for health-related quality of life of medical professionals
![]()
Perception of health
Definition and components of health
While participants agreed on the definition and components of health of the WHO, they indicated that it represents an ideal rather than a realistic goal. In addition, some participants felt the definition of health was vague since it was difficult to distinguish between its physical, mental, and social aspects. Participants thought that this ambiguity leads to complications in measurement, by making it difficult to accurately judge someone's health status.
“I've heard about the definition [of WHO] roughly. I mean I agree with that, but it doesn't explain much in detail. Nobody knows what this really describes specifically. The whole thing is just vague.” (Participant 1 in group 3)
When asked about the definition of health from the perspective of the medical professional, participants ranked its “mental aspect” as the most important. One participant suggested that when it comes to thinking about health, the physical aspect comes first normally, while from the medical professional's point of view, mental health is the most important because they serve the health of others.
“Since we exist to improve other people's health, we may not be able to perform the proper surgery if the mental health of the treating person is not healthy, and if we are not mentally healthy in terms of ethics about people and life, it could harm the patient. In this respect, or in ethical terms, I think we will be able to provide medical care properly when we have no abnormal psychosis…” (Participant 7 in group 2)
Criteria for classifying health status
The participants considered a healthy person to be a person who can do what he/she wants, is energetic with positive energy, and does not harm others. “Negative energy” was mentioned the most frequently when participants were asked to explain unhealthy people. Specifically, participants suggested that unhealthy people have a distorted facial expression, and display a lot of irritation, anger, sighing, and helplessness, which has a negative psychological effect on the participants.
“The life you want to live can be a social life, or you can go to school if you are a student, or manage a household if you are a housewife. I consider the status of an average person that is not suffering from a health problem and not hindered in their desired emotional, physical, and social functions as healthy.” (Participant 4 in group 3)
“Unhealthy people are always frowning, while people who are healthy are smiling.” (Participant 4 in group 1)
When asked about the perception of the health status among medical professionals, one participant responded that medical professional tend to say that they are relatively healthy since they judge their health compared to their patients. Another participant noted that the physician group tended to have a higher quality of life, although their occupation is labor-intensive and stressful.
Perception of one's health status
Most participants said they were not healthy; they have experienced fatigue from irregular sleep schedule, discouragement in social relationships, and deterioration of physical functioning. On the other hand, some participants thought they were healthy due to a high level of resilience and satisfaction with life and acceptance of the subjectivity of life.
“I take a lot of medicines (That's why I'm not healthy). Hard to be flexible, and [I] always wake up at dawn.” (Participant 4 in group 2)
“I am mentally resilient, and I tend to shake things off well even if I get stressed because I am quick to overcome or rationalize stressful situations. In terms of health, I feel sick in some parts of my body, but it is not a disease that cannot be fixed or causes problems in my life. So I think... (I'm healthy)” (Participant 6 in group 1)
In addition, some participants mentioned they could not give an accurate answer to their health status, because they were unsure about the definition of health and their health state changed depending on the circumstances.
“That's a difficult question to answer. Because, as you know, there are patients who concern a bit much about their health status, and I am like them too. The concept of ‘being healthy’ feels quite complicated to me. …Well, I haven't started to take any medicines. But since I am getting old, my knees do hurt. Then I ask myself, ‘Am I healthy?’ and I can't clearly answer to that with certainty.” (Participant 1 in group 1)
Factors degrading health-related quality of life among medical professionals
Difficulty in sleeping due to work patterns
Cumulative fatigue was the most frequently cited factor that deteriorated the health-related quality of life of medical professionals. Participants working in general hospitals where they work three shifts or are on call responded that they suffer from sleep deprivation due to an irregular lifestyle. One participant had experienced falling asleep while reading the patient's test results, while another participant mentioned that he/she had difficulty in waking up due to lack of sleep.
“I am physically sleep-deprived… and I feel physical fatigue because I'm unfamiliar with the work pattern of three shifts.” (Participant 2 in group 1)
“Sometimes I doze off while reading the results. Cause I can't sleep at night...” (Participant 4 in group 2)
Likewise, a medical professional working in clinics also mentioned that he/she has treated patients while feeling fatigued or experienced dozing off in a chair. Although there was variability in responses depending on the work pattern, the results suggest that most medical professionals are hampered by accumulated fatigue when facing patients.
Psychological burden due to occupational characteristics
The professional nature of a medical practitioner as someone who helps others lead a healthy life was one factor that gave participants satisfaction with their work but was also a burden. One participant mentioned that he/she was always under pressure since his/her actions could determine a patient's life and death. Another participant had vague anxiety about the occurrence of an unexpected medical accident.
“Our department rotates every three months. Since departments of surgery keep changing, I have to keep learning new procedures. Even if I have nine years of experience [performing a surgical procedure], I have to start new again. That's too stressful. I’m scared.” (Participant 3 in group 1)
Participants also suffered from anxiety due to certain patients (respiratory diseases, Middle East respiratory syndrome [MERS], tuberculosis, infectious diseases such as human immunodeficiency virus) that they encountered as medical personnel. This has led to concerns not only about themselves, but also about their families, which caused participants to step away from their relationship with the family.
“The day I met a patient with MERS, I started to feel sick. Rather than worrying about myself getting MERS, I was worried that my family could get sick because of me and my work. Also, the day I met a scabies patient, I felt itchier. I have a baby less than 12 months old, and I wonder if I should or could hold my baby. On such a day, I felt sorrier for my family.” (Participant 3 in group 2)
Suffering chronic pain while taking care of patients
Many participants were found to experience chronic pain in their lives as medical professionals. One participant was having difficulties in his/her daily life after being diagnosed with plantar fasciitis while working as a nurse. Another participant said that many dentists or otolaryngologists have a problem with a neck disc. Participants also complained of chronic pain in the wrist, shoulder, and knee areas while caring for patients, although the type of pain they experienced differed depending on their work.
“I was diagnosed with plantar fasciitis because my foot hurt last year. It can be caused by obesity or excessive movement… I work in a general ward, so I have a lot of coming and going, and I often lift patients to change their positions. I think it's resulted from moving a lot.” (Participant 4 in Group 1)
“A lot of dentists and otolaryngologists have [pain in a] neck disc.” (Participant 3 in group 3)
Measures to improve health-related quality of life of medical professionals
Decreasing work burden by recruiting additional staff
Reinforcement of staff has been proposed as one of the ways to improve the quality of life of participants, especially for those in the nurse group. Excessive work has caused participants to feel anxiety and depression. Participants suggested that if the workforce was added, burnout of the medical professional would be reduced, and patients and caregivers could be provided with more friendly and high-quality medical services.
Ensuring adequate rest and medical fees
Most participants were found to have experienced burnout from work, which had a negative impact not only on their quality of life, but also on their family relationships and health care services. The workforce shortages and excessive work problems previously mentioned are related to insufficient rest for medical professionals. Participants mentioned that if they were able to get more rest through the recruitment of additional personnel in hospitals or the government was to guarantee rest for medical professionals, the health-related quality of life among medical professionals would be improved.
“I think it would be nice to have a lot of vacation provided [by the government]. Those who want a break can take a rest and those who have a relationship can get together.” (Participant 2 in group 2)
In addition, the group of physicians mentioned that the guarantee of higher medical fees than the present fees could also be a way to improve their quality of life.
“If raising medical fees is not available systematically, we should be able to take more breaks and get some compensation for the break time. I'd like the government to make sure that we don't work more than 52-hour to meet the working standard and that we are compensated for that so that we can earn income while resting. We work under state control, so I don't think it's reasonable to be treated the same as other self-employed people. (Participant 3 in group 3)
Opinions on health-related quality of life measurement tools for medical professionals
Necessity of measuring health-related quality of life for medical professionals
When asked whether it is necessary to measure the health-related quality of life for medical professionals, all participants except one said it is essential. The participant who did not agree on the necessity indicated that it was contradictory to regulating working hours for the medical professional differently from other occupations. Other participants thought it was necessary to regularly measure health-related quality of life for medical professionals and preferred it to be in the form of recommendations rather than obligations.
Applicability of existing health-related quality of life measurement tools
Participants indicated that the Mayo Well-Being Index, the EQ-5D-5L (including EQ-VAS), and the HINT-8 were generally ambiguous. In addition, they emphasized the necessity of providing details to accurately reflect the professional lives of medical staff.
1) Mayo Well-Being Index
Participants felt the Mayo Well-Being Index was specific but lacked details. The response scale of most items consisted of a dichotomy, which made it both simple but also gave it low discrimination. When a specific situation was presented, participants felt that the words used were likely to be subjectively interpreted and focused on the spiritual aspect. Participants reported that the item that asked about the impact of work schedules on leisure time or family time was the most important in terms of measuring the quality of life among medical professionals.
2) EQ-5D-5L & EQ-VAS
The EQ-5D-5L questionnaire consists of five response scales asking about the day's health status of following dimensions: mobility, self-care, daily activities, pain and discomfort, and anxiety and depression. EQ-VAS requires the day's health status to be marked on a 100-point scale. One participant said that he/she considers the questionnaire easy to respond to since the questionnaire focuses on “today.” Other participants said that the EQ-5D-5L and EQ-VAS surveys were simple and easy-to-understand, and not difficult to complete. However, some thought they were unsuitable for measuring the health-related quality of life of medical professionals since EQ-5D-5L consists of dimensions that would not be problematic for medical professionals. Still, some participants said that if the survey were to be completed before and after work or repeated measurements were accumulated, it would be worthwhile.
3) HINT-8
All three groups of participants mentioned that a measure needs to assess “difficulty in sleeping” in order to accurately measure the health-related quality of life among medical professionals. Although the HINT-8 questionnaire asked about the difficulty of sleeping, the participants expressed the most dissatisfaction with the questionnaire itself out of the three tools they reviewed. Some participants found the HINT-8 difficult to understand because the sentences in the questionnaire did not read well. In addition, since the questionnaire was generic, it was thought that the specific meaning was not conveyed and that there would be no discrimination amongst other occupation groups. Participants pointed out that when using the questionnaire to measure the health-related quality of life of medical professionals, the subdivision of the items and the subtle differences between the words within the items should be sufficiently considered and corrected.
Need to add items specific to the job characteristics of medical professionals
Overall, participants expressed considerable dissatisfaction with the existing health-related quality of life measurement tools. They pointed out that while the existing survey tools may be suitable for the general population or patients, they rarely reflected the characteristics of medical professionals and suggested that various items should be added to measure the health-related quality of life of medical professionals (Table 3). One participant commented that the questionnaire should be changed depending upon the occupational group and position in the medical institution.
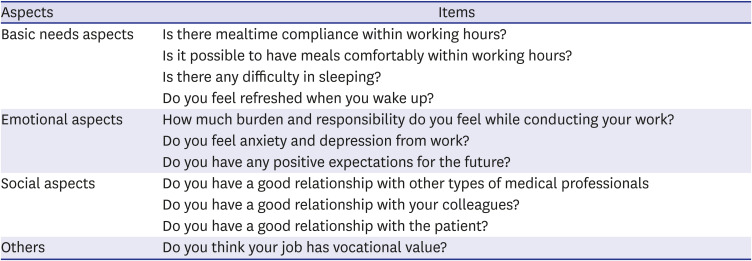
Table 3
Items that should be considered additionally crucial in the measurement of health-related quality of life for medical professionals
![]()
“I hope that stress will be assessed a little more as well as fatigue. Not only my current status, but also hope, vision, or positive thinking for the future should be assessed more. I think that is very important.” (Participant 1 in group 2)
“‘Have you ever skipped meals for work?’, ‘Have you ever refrained from going to the bathroom for more than an hour because of work?’” (Participant 2 in group 2)
DISCUSSION
This study conducted three FGDs with 18 healthcare professionals in Korea (6 nurses, 7 physicians in a hospital, and 5 physicians in a clinic) to examine their perceptions of health-related quality of life and their opinions on measuring, evaluating and improving the health-related quality of life of Korean medical professionals. This study is of great significance because it highlighted the need to more comprehensively measure the health-related quality of life of medical professionals, identified the limitations of existing health-related quality of life measurement tools, and provided implications for the development of new tools. There may be fundamental cultural and social differences regarding health-related quality of life issues. A limitation of most studies that address health-related quality-of-life issues for medical professionals is that they have been conducted in Western countries. This study adds a more diverse cultural interpretation of health-related quality of life for medical professionals. Unlike the existing studies, the current study also examined the in-depth perceptions of medical professionals using a qualitative research methodology.
Participants in this study provided multiple opinions on the definition and components of health, while also focusing on the ambiguity in the current definition of health. Some felt their health status was good, but most were not confident that they were in good health. Although we did not verify the actual health of participants, many of them mentioned that they considered the health definition of the WHO (which includes physical, mental, and social well-being) to be an ideal rather than an achievable goal. A previous study found that Koreans evaluated their health ideally and recognized good health only when certain criteria were met.27 Therefore, the health-related quality of life of medical professionals should be considered comprehensively rather than by only assessing specific dimensions or items such as its mental or physical aspects.
The participants in this study complained of various health problems covering multiple aspects of health. In addition to the various physical and psychological symptoms8101112132829 identified in previous studies, participants in this study complained of work-related burdens, anxieties, and fears along with physical burdens such as fatigue, lack of sleep and insomnia, and chronic pain due to their work burden. In other words, health-related quality of life issues related to medical environmental aspects, such as working hours and intensity, are likely to be more critical for Korean medical personnel. Vitality and sleep were suggested as important health-related quality of life items that need to be assessed in addition to the EQ-5D for the general population in Korea.30 Fatigue and the lack of sleep caused by the long hours of work prevalent in Korean society, including the medical field, have been raised as major social problems.31 Although efforts have been made in Korea to limit long hours of work, including recent efforts to restrict residents to no more than 80 hours of work per week, realistic measures need to be identified based on consensus within the medical community and by securing more personnel.32
It is also worth noting the mental difficulties identified in this study. In addition to the difficulties associated with their workload, participants in this study complained of anxiety, pressure, and fear of the complexity of the work and the possible negative consequences. The mental difficulties arising from the work of medical professionals have received little attention in previous studies. In particular, some participants complained of vague anxiety about medical malpractice. Medical professionals who have experienced actual cases of patient safety accidents complain of psychological difficulties,633 indicating that medical professionals would benefit from training on how to address patient safety incidents34 and provide support for the psychological difficulties of all affected.35
In order to improve the health-related quality of life of medical professionals, it is necessary to measure it properly and reliably. It is expected that there will be little resistance from physicians and nurses to participating in the measurement process, as most participants in this study acknowledged the need to measure the health-related quality of life for medical professionals. However, since the measurement and tool used will be of considerable importance, this study collected opinions from participants on three representative tools. The participants pointed out the shortcomings of each tool, and suggested the need for a measurement tool that reflects the occupational characteristics of health professionals. The opinions of participants regarding the advantages and disadvantages of the three tools are summarized in Table 4.
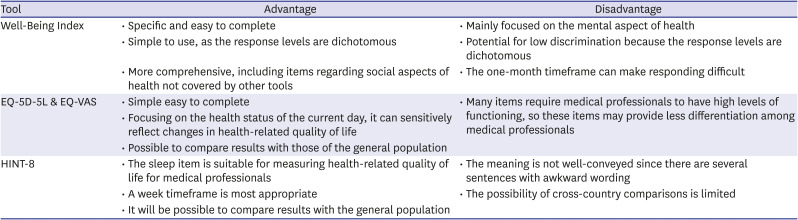
Table 4
Advantages and disadvantages of major existing tools in measuring health-related quality of life among medical professionals
EQ-5D-5L = 5-level EuroQol-5D, EQ-VAS = EuroQol Visual Analogue Scale, HINT-8 = Health-related Quality of Life Instrument with 8 Items.
![]()
Since there is currently no tool specific to medical professionals that comprehensively measures their health-related quality of life,16 and there is an overall lack of standardized approaches to systematically measuring health-related quality of life,17 multiple considerations need to be addressed in selecting a tool, including how frequently the measure is assessed, the comprehensiveness of items, the ease of use, and its comparability to existing tools. Although a tool should be simple when measuring the health-related quality of life for medical professionals who have little time,36 the various aspects of health-related quality of life should be comprehensively assessed to increase the acceptability of the tool among medical professionals.18 In addition, it is essential to regularly measure a specific health care group and monitor their changes over time, to identify how much the health-related quality of life for medical professionals compares across measurement tools and with other occupational groups or the general public.
To address the measurement issues, it may be necessary to consider using two or three tools together. In developing a new measurement tool of health-related quality of life specific to medical professionals, the additional items identified in this study should be considered. In particular, it is recommended that a tool used in Asian cultures such as Korea includes social dimensions or items that address relationships with colleagues or family. In addition, the inclusion of items that evaluate positive aspects of medical professions such as vocational value and degree of fulfillment may prevent a ceiling effect in the results.19
There were several limitations of this study. One limitation is that it did not explore the opinions of medical professionals regarding a more diverse array of survey tools. While this study identified the perceptions of participants on three representatives of health-related quality of life measurement tools, it would be useful in a future study to identify in-depth opinions regarding other measurement tools as well. Another limitation of this study is that it did not include participants from diverse healthcare occupations. While this study was conducted with physicians and nurses, it is necessary to expand our understanding of the views of medical professionals on health-related quality of life by conducting similar studies with pharmacists and emergency medical technicians.
In conclusion, this study conducted three FGDs with 18 physicians and nurses in Korea to identify their perceptions of health-related quality of life as well as their opinions on its measurement and evaluation. The study obtained basic data on how to improve health-related quality of life, and its results support the need for future studies to investigate health-related quality of life for medical professionals in Korea and also help determine the method of assessment. In addition, the dimensions or items related to health-related quality of life that were identified as important by medical professionals may be used as references for developing future health-related quality of life measurement tools for medical professionals.
 XML Download
XML Download