

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
A novel coronavirus outbreak occurred in December 2019 in Wuhan in Hubei province in China.1 The virus was named severe acute respiratory syndrome corona virus-2, and the disease was named coronavirus disease 2019 (COVID-19).2 What started as a local epidemic became a pandemic, as declared by the World Health Organization (WHO) on March 11, 2020.3 As of April 29, 3,024,059 cases were confirmed as COVID-19 and 208,112 people had died from the disease in 213 countries, areas, or territories around the world according to a COVID-19 outbreak situation report provided by the WHO.4
It is important to estimate the impact of disease for appropriate health policy decision-making. Traditionally, classical epidemiological indicators such as incidence, prevalence, mortality, and case fatality rate have been used for measures of disease impact. Mortality and case fatality rate, in particular, can show the significance of diseases, and thus these measures are often reported. Therefore, WHO and each country have been reporting their COVID-19 situations using these indicators.4 However, case fatality rate and mortality have the limitation that they do not reflect the years of life lost (YLLs) so they do not portray the true impact of a disease. Therefore, the Global Burden of Disease (GBD) study has used the YLLs to calculate disability-adjusted life years (DALYs).5 This study aimed to estimate the YLLs due to COVID-19 in 30 high-incidence countries.
METHODS
In this study, YLLs is used to measure the burden of the COVID-19 in the 30 countries with the highest incidence of COVID-19. These 30 countries were selected from the data provided by the WHO on April 13, 2020 when the study was planned.6 The countries included were: Netherlands, Norway, Germany, Russia, Romania, United States of America (USA), Belgium, Brazil, Sweden, Switzerland, Spain, Ireland, Ecuador, United Kingdom (UK), Austria, Iran, Israel, Italy, India, Japan, China, Chile, Canada, Turkey, Peru, Portugal, France, Australia, and the Korea.
The age- and sex-specific cases and deaths were determined using publicly available data. First, the country-specific new and deceased cases of COVID-19 as of April 22 and July 14, 2020 were determined using from publicly open sources (Supplementary Tables 1 and 2). Second, the sex-specific number of confirmed cases and deaths were determined according to country. When the sex-specific numbers were reported for a country, the data were used. If the number of cases was not reported by sex, the distribution of the sex ratio by Global Health 50/50 was used.7 Third, the age- and sex-specific confirmed and deceased cases were recorded for each country, if these figures were available. If the age-specific number of cases were available, but the age- and sex-specific estimates could not be found, the age distribution of COVID-19 related figures in each country was used to calculate the number of COVID-19 cases by age- and sex. If the age-specific values were not available, they were calculated by applying the proportions for the aggregate of the number of the age- and sex-specific confirmed and deceased cases from the countries where the data were available for each of the reference dates in April (Spain, Italy, France, Portugal, Switzerland, Chile, Belgium, and Peru) and July (Spain, Italy, Germany, France, Portugal, Switzerland, the UK, Chile, and Belgium). Age was divided into 10-year age groups in individuals under 80 years, and 80 years and older.
The life expectancy of Japanese females at one-year age intervals, which is the longest life expectancy globally, was used to estimate the YLLs.8 Demography data from the United Nations were used to calculate the incidence and YLLs per 100,000 population.9 The results of YLLs were compared by country, sex, age group. The correlations between YLLs due to COVID-19 and the incidence or mortality were calculated. Finally, the portions of the YLLs were estimated using the results from the GBD 2017 study.10
RESULTS
Comparing YLLs due to COVID-19 by country
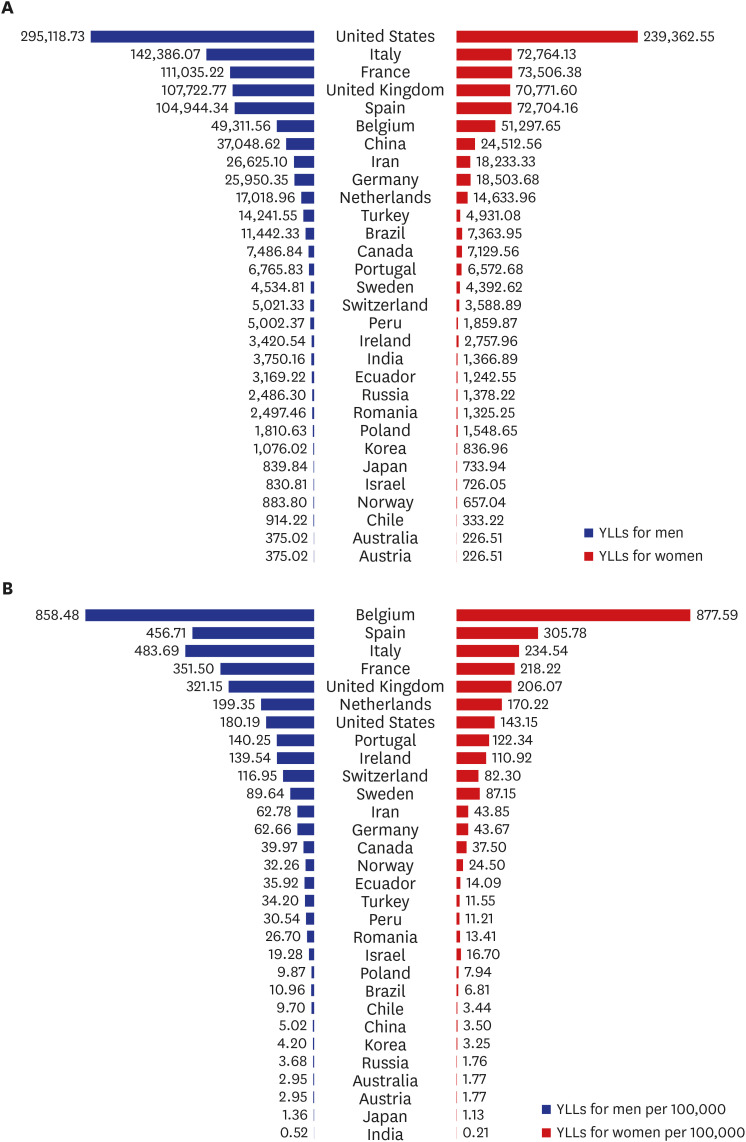
Overall results of YLLs due to COVID-19 by sex and country as of April 22 and July 14, 2020 are presented in Supplementary Tables 3 and 4. As of April 22, 2020, YLLs due to COVID-19 in the 30 targeted countries were 1,699,574. When the YLLs due to COVID-19 was compared between 30 countries, the USA had the highest total value of 534,481 YLLs among the countries considered (Fig. 1A), followed by Italy (215,150), France (184,542), Spain (177,649), and Belgium (100,609). In Italy, the YLLs due to COVID-19 among males (142,386) were about twice of that among females (72,764). Belgium was the only country in which the YLLs due to COVID-19 was higher in females than in males. Belgium had the highest YLLs due to COVID-19 when estimated per 100,000 population (868.12), followed by Spain (379.96), Italy (355.84), France (282.72), and the Netherlands (184.73) (Fig. 1B).
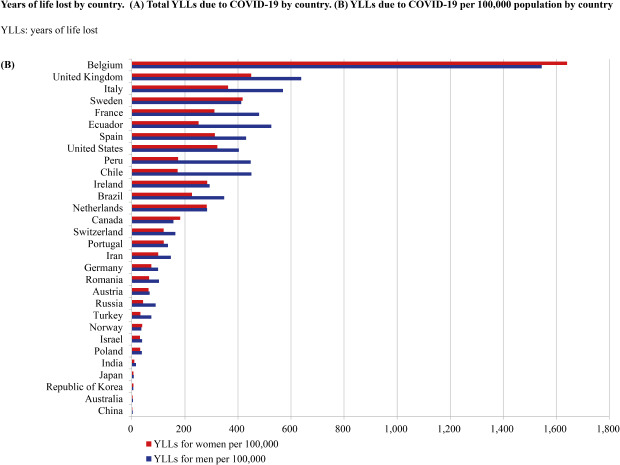
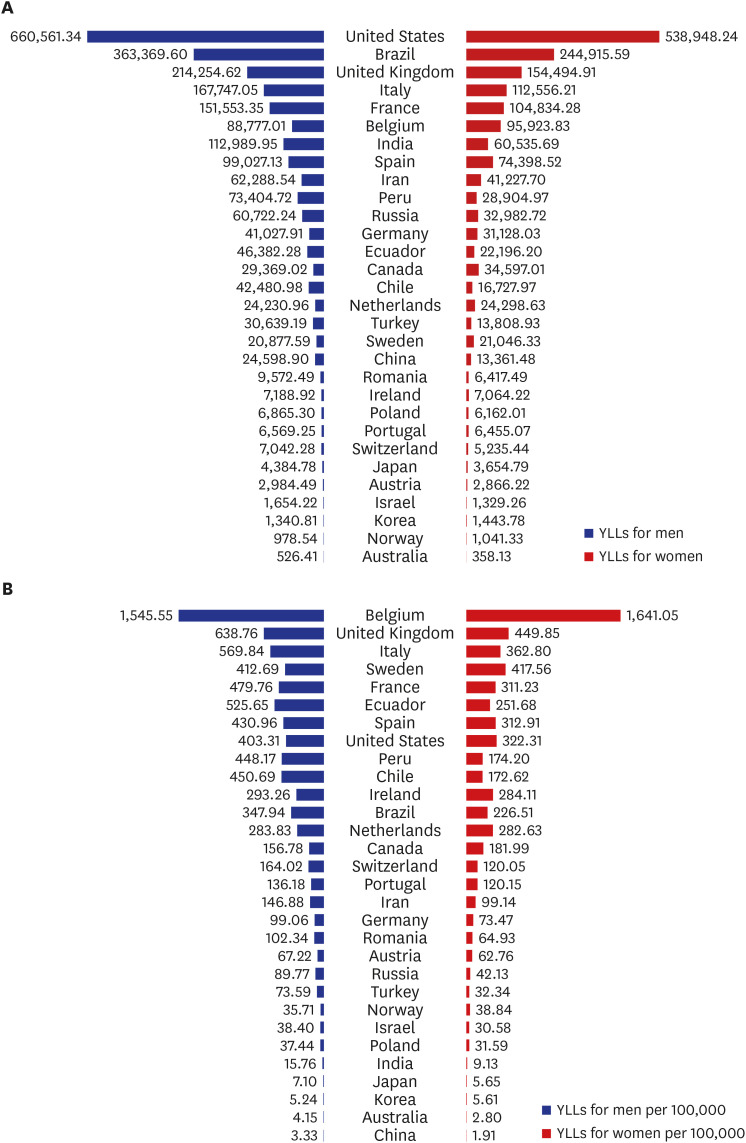
As of July 14, 2020, a total of 4,072,325 YLLs were caused by COVID-19. Similar to the results from April, the USA had the highest total value of 1,199,510 YLLs among the countries considered (Fig. 2A), followed by Brazil (608,285), UK (368,737), Italy (280,303), and France (256,388). The USA was also the country with the largest difference in YLLs between men (660,561) and women (538,948). In Belgium, conversely, women (95,924) had greater YLLs than men (88,777). Belgium had the highest YLLs due to COVID-19 when estimated per 100,000 population (1,593.72), followed by United Kingdom (543.17), Italy (463.60), Sweden (415.12), and France (392.79) (Fig. 2B).
Comparing YLLs due to COVID-19 by age group
Combined results of YLLs due to COVID-19 in 30 countries as of July 14, 2020 were analyzed in detail (Table 1). Total YLLs due to COVID-19 were higher in men (2,363,410) than in women (1,708,915). In the case of YLLs due to COVID-19 per 100,000 population, the rate was also higher in men (104.68) than in women (77.78). In men, the total YLLs due to COVID-19 was highest in the 70–79-year age group (752,599), while in women, the total YLLs due to COVID-19 was highest in the 80 years and older age group (664,502). In both men and women, the YLLs due to COVID-19 per 100,000 were the highest among those aged 80 years and older (1,205.66 and 981.05, respectively). The total YLLs due to COVID-19 among individuals aged 70 years and older accounted for more than 50% of the total YLLs (58.8%) in all age groups, while the total YLLs due to COVID-19 among individuals aged 60 years and older accounted for about three-quarters of the total YLLs (79.5%) in all age groups.
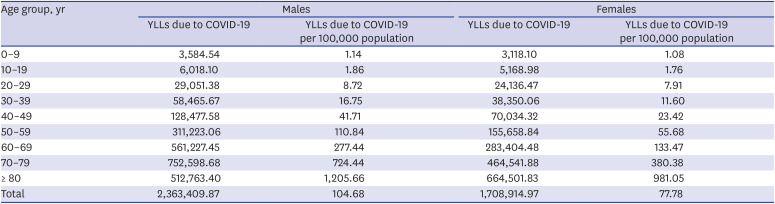
Table 1
Years of life lost due to COVID-19 according to sex and age group in the 30 target countries as of July 14, 2020
![]()
Association between YLLs due to COVID-19 and other parameters
The YLLs due to COVID-19 was related to other epidemiological parameters, such as the number of cases and number of deaths due to COVID-19. The Pearson correlation coefficients between the YLLs due to COVID-19 and the incidence of COVID-19 (Fig. 3A) and the YLLs due to COVID-19 and number of deaths due to COVID-19 (Fig. 3B) were 0.933 (high-case fatality countries, 0.760; low-case fatality countries, 0.988) and 0.989, respectively, which were both statistically significant (P < 0.001). Among 29 countries excluding results from the USA, the Pearson correlation coefficients between the YLLs and the number of confirmed COVID-19 cases (Fig. 3C) and between the YLLs and the number of deaths due to COVID-19 (Fig. 3D) were 0.783 (P < 0.001; high-case fatality countries, 0.760; low-case fatality countries, 0.972) and 0.989 (P < 0.001), respectively.
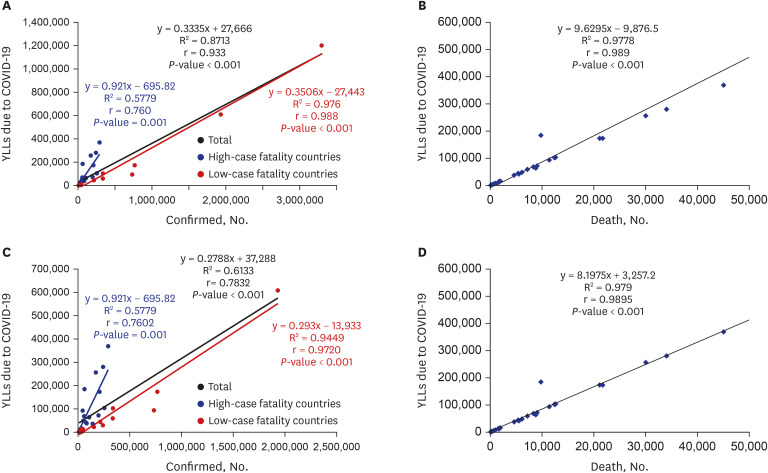
Fig. 3
Correlation between COVID-19 parameters and YLLs. (A) Correlation between the COVID-19 incidence and the total YLLs due to COVID-19 in 30 countries, (B) Correlation between number of deaths due to COVID-19 and the total YLLs due to COVID-19 in 30 countries, (C) Correlation between the COVID-19 incidence and the total YLLs due to COVID-19 in 29 countries excluding the USA, (D) Correlation between number of deaths due to COVID-19 and the total YLLs due to COVID-19 in 29 countries excluding the USA.
YLL = years of life lost, COVID-19 = coronavirus disease 2019.
![]()
Percentage of YLL due to COVID-19 in total YLLs and DALYs by country
Table 2 shows the proportions of YLLs due to COVID-19 per 100,000 population and the total value of YLLs and DALYs per 100,000 population by country. Belgium was the country with the largest proportion of the YLLs due to COVID-19 in the total YLLs per 100,000 (11.3%), followed by the UK (4.0%), Italy (3.5%), Sweden (3.3%), France (3.13%), and Spain (3.05%), which also accounted a high proportion of YLLs due to COVID-19 per 100,000. Similarly, in Belgium (5.7%), UK (2.0%), Italy (1.7%), and Ecuador (1.6%), YLLs due to COVID-19 accounted for a high proportion of the total value of DALYs per 100,000 population in the country.
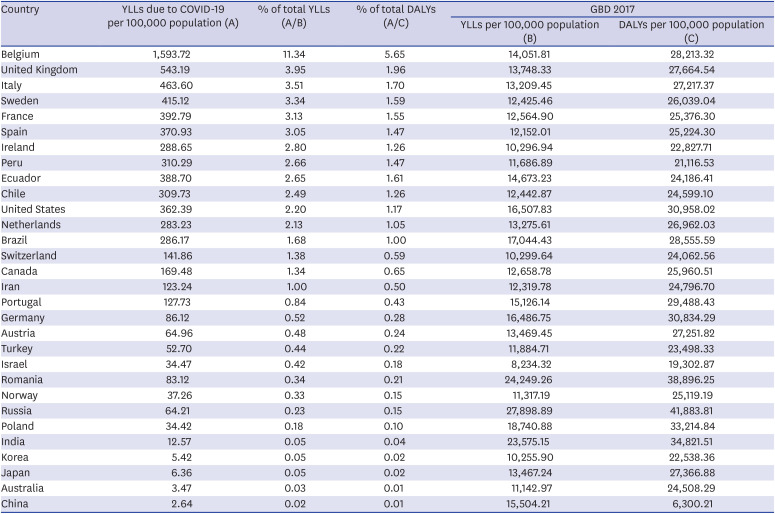
Table 2
Percentage of YLLs due to COVID-19 in relation to total YLLs and by country
YLL = years of life lost, COVID-19 = coronavirus disease 2019, DALYs = disability-adjusted life years, GBD = global burden of disease.
![]()
DISCUSSION
This study estimated the YLL due to COVID-19 by country, sex, and age group in 30 countries with a high incidence. As of July 14, 2020, a total of 4,072,325 YLLs due to COVID-19 had occurred in 30 countries, which increased from a total of 1,699,574 YLLs in April. When observed by country, the total YLLs due to COVID-19 was highest in the USA, followed by Brazil, UK, Italy, and France. However, Belgium had the highest YLLs due to COVID-19 per 100,000 population, followed by the UK, Italy, Sweden, and France. The YLLs due to COVID-19 were higher in men than in women, and the YLLs due to COVID-19 in individuals aged 60 years or older accounted for more than three-quarters of the total. Belgium also accounted for the largest YLLs due to COVID-19 as a proportion of the total disease burden, while COVID-19 also accounted for a large portion of the total disease burden in the UK, Italy, and Ecuador.
The results of this study could be used as a basis for estimating the global burden of COVID-19. The results also reveal which countries each should take more active measures to lower the disease burden of COVID-19. By country, the USA had the largest number of YLLs due to COVID-19 as of July 14, 2020, which is likely to have been affected by the case fatality, population size, the number of incident cases, the medical system, and the frequency of contact between people. Most of all, the case fatality is the most important factor leading to the increase in the burden of COVID-19, which has been related to the rapid outbreak that exceeds the facility capacity in several previous experience from regions like Wuhan, New York, and Deagu. Especially, the R0 of COVID-19 is considerably high,11 implying the necessity to implement a incidence control policy such as social distancing, mask-wearing, and hand-washing.
Furthermore, our results showed that there was a strong correlation between the total YLLs due to COVID-19 and its epidemiologic indicators: Pearson correlation coefficient between the incidence and the YLLs due to COVID-19 was 0.933; the correlation coefficient between the mortality and the YLLs due to the disease was 0.989. From the results, the burden of COVID-19 in context of YLLs were not only highly associated with the number of deaths, which contributes directly to YLLs as included in the calculation, but also with the number of confirmed cases, especially among the countries with a lower case fatality rate. As the number of confirmed cases increases, it may result in the overloaded healthcare system, failing to care for all those have been infected. Particularly, at the beginning of the pandemic, unpreparedness as well as the lack of capacity to screen and accommodate all COVID-19 related patients led to a step-behind detection of cases. Corroborating, results on the correlation between the incidence, mortality, and YLLs from the current study emphasize the importance of the early detection of infections, which could minimize the burden of COVID-19.12
The YLLs due to COVID-19 were mostly concentrated in the older population, who were the most vulnerable group. Older people are more likely to have underlying diseases such as diabetes and chronic obstructive pulmonary disease, and may be more vulnerable to COVID-19, due to lower lung capacity.13 In addition, the COVID-19 pandemic has resulted in a large number of patients in a short period of time, resulting in a shortage of hospital beds, particularly intensive care unit beds. It is necessary to classify the severity of the disease and establish appropriate treatment strategies, and to increase treatment resources for the vulnerable, including the elderly.1415
It is difficult to predict the extent to which COVID-19 will increase the disease burden by country as the spread has not been curbed. In Belgium, the COVID-19 YLLs has already exceeded 10 percent of the YLLs for the whole of 2017, while in India, Korea, Japan, Australia, and China, COVID-19 accounts for less than 0.1 percent of the 2017 YLLs. In Belgium as well, YLLs account for a high proportion of deaths, but further data collection and review is required to determine whether COVID-19 will replace other causes of death or will increase the total number of deaths. However, considering not only the medical burden caused by COVID-19 but also the socioeconomic burden caused by this pandemic, the burden of COVID-19 cannot be underestimated. Establishing a system to cope with this new infectious disease is a key public health challenge.16 In addition, a long-term strategy needs to be considered until the vaccine or anti-viral agent for COVID-19 is developed.
One of the notable characteristics of the study is the variability in the level of data available in different countries. In some countries such as United States, Korea, Italy, and Portugal, data on age- and sex-specific incidence and mortality were available. In addition, data were available on the number of negative test results in one country (Korea). In other countries such as Brazil, Peru and Ecuador, the age-specific mortality figures were available, but not the age-specific incidence. In some countries (Turkey and Iran), only the total number of cases was available. Because the age- and sex-specific incidence and mortality are the basis of epidemiology and the basis for efficient preventive intervention and international comparisons, the availability of data should be improved.
There were some limitations to this study. First, as the pandemic is ongoing, the results from this study are provisional and the YLL will be increased. However, there is a need to estimate the YLLs attributable to COVID-19 even though the figures are likely to change over time, because it could support the decision-making process regarding the allocation of resources. Second, in some countries we estimated the number of deaths by sex and age group using the demographic distributions from known data. Sex- and age- specific confirmed cases were unavailable in 14 out of 30 countries (78.1% of the total cases), while the number of deaths were unavailable in 18 out of 30 countries (55.8% of the total deaths) for the estimation of YLLs due to COVID-19 as of July 14, 2020. Third, the total number of the deceased by country could be inaccurate. While in some countries the number of deaths among those who were not diagnosed before their death was not reported, other countries tried to identify deaths due to undiagnosed COVID-19 by mean of posthumous testing. When the detailed demographic information on deaths due to COVID-19 is reported, the YLLs will be able to be calculated more accurately. Lastly, we only included the top 30 countries with the highest incidence. However, the 30 countries included in the study occupied 91.1% of the total number of confirmed cases as of April 22, 2020, and 75.6% of the total confirmed case as of July 14, 2020.6 Therefore, it could be said that we measured almost the entire YLLs due to COVID-19 in the current situation.
In conclusion, the burden of COVID-19 due to premature death is currently highest in USA, Italy, and France, while the YLLs per 100,000 are currently highest in Belgium, Spain, and Italy. In the highest burden countries such as Belgium and Spain, the burden of COVID-19 already exceeds 3% of the total YLLs. Incidence as well as mortality is very closely related to YLLs which highlights the importance of prevention of infection. Therefore, control measures should focus on preventing the spread of infection.
 XML Download
XML Download