

 ePub
ePub Citation
Citation Print
Print


| Korean J Gastroenterol. 2015 Dec;66(6):340-344. English. Published online December 22, 2015. https://doi.org/10.4166/kjg.2015.66.6.340 | |
| Copyright © 2015 The Korean Society of Gastroenterology | |
|
Eun Soo Jeong,
Su Jin Hong, | |
| Digestive Disease Center and Research Institute, Department of Internal Medicine, Soonchunhyang University College of Medicine, Bucheon, Korea. | |
|
1Department of Pathology, Soonchunhyang University College of Medicine, Bucheon, Korea. | |
| Received May 01, 2015; Revised August 03, 2015; Accepted August 10, 2015. | |
|
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by- | |
|
Abstract
| |
|
While endoscopic submucosal dissection (ESD) is widely used to treat gastrointestinal tumors, it is rarely used for subepithelial tumors (SETs) originating from the muscularis propria of the esophagus and gastric cardia because of the risk of perforation and problems with inadequate space and field of view during procedures. Submucosal tunneling endoscopic resection (STER) is a new therapeutic method for treating SETs in specific locations in the esophagus and stomach. This technique is highly skill-dependent, using a mucosal flap that covers a deeper part of the gut wall, but is safe and minimally invasive compared with conventional endoscopic approaches such as ESD in SETs originating from the muscularis propria.We report a patient who underwent STER to remove a SET located at the gastric cardia. The patient recovered without any complications. We believe that our case shows the efficacy and safety of the STER technique for patients with a SET originating from the muscularis propria. |
|
Keywords: Cardia; Muscle; Subepithelial tumor; Submucosal tunneling endoscopic resection |
|
|
INTRODUCTION
|
Gastrointestinal subepithelial tumors (SETs) are usually found incidentally during routine endoscopic examination. Surgical resection is the standard treatment for gastrointestinal SETs.1 However, with recent developments in endoscopic procedures, endoscopic resection is now commonly performed to remove gastrointestinal SETs.2
While standard endoscopic submucosal dissection (ESD) is widely used to treat gastrointestinal tumors, it is rarely used for tumors of the esophagus or gastric cardia, because of the risk of perforation and problems with inadequate space and narrow vision during the procedures. In addition, ESD is difficult when treating subepithelial lesions originating from the muscularis propria layer.
The submucosal tunneling technique was first described for transesophageal mediastinoscopy via submucosal endoscopy with a mucosal flap.3, 4 During the procedure, a submucosal tunnel, which provides working space, is created for endoscope insertion into the mediastinum or peritoneal cavity. Submucosal tunneling endoscopic resection (STER) is a modification of the submucosal tunneling and ESD techniques for gastrointestinal SETs resection.
This report presents a case in which STER was used to remove a SET originating from the muscularis propria of the gastric cardia.
|
CASE REPORT
|
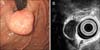
A 50-year-old man was diagnosed with a growing gastric SET at a private clinic. He was referred to Soonchunhyang University Bucheon Hospital (Bucheon, Korea) for management of the lesion, as it was enlarged compared to a previous examination. He had a history of hypertension and diabetes mellitus controlled with oral medications. The physical examination was unremarkable. Esophago-gastro-duodenoscopy (EGD) showed a 2 cm diameter SET located in the gastric cardia (Fig. 1A). EUS showed a homogenous, hypoechoic tumor originating from the muscularis propria layer (Fig. 1B).
|
We performed STER under standard general anesthesia with endotracheal intubation using a dual-channel endoscope (GIF-Q260J; Olympus, Tokyo, Japan) with a plastic fitted cap (MH-583; Olympus). Carbon dioxide insufflation was used during the procedure. Other equipment included a high-frequency generator (VIO 300D; ERBE, Tübingen, Germany), hook knife (KD-620LR; Olympus), insulated-tip knife 2 (IT2; KD-611L; Olympus), hemostatic clips (HX-610-090L; Olympus), and injection needle (NM-200L-0423; Olympus).
The STER procedure is shown in Fig. 2 and the video file (Supplementary data). From 5 cm proximal to the SET, a saline solution with indigo carmine and diluted epinephrine (1:100,000) was injected into the esophageal wall until the mucosa was lifted fully. To create mucosal entry into the submucosal space, a 2 cm longitudinal incision was made on the esophageal mucosa. ESD technique created a submucosal tunnel downward until the SET was visualized in the endoscopic field. After the SET was exposed, the margin was dissected using endoscopic knives, including a hook knife and IT2 knife (Fig. 2A). We mainly used the hook knife during dissection of the tumor base from the muscularis propria layer for cutting the muscle fibers. The tumor was dissected into two pieces because the tumor shape narrowed the working space in the submucosal tunnel. After removing the SET through the tunnel, we performed precise hemostasis using hemostatic forceps for several minutes to prevent a hematoma in the submucosal tunnel. The mucosal entry was closed with several hemostatic clips (Fig. 2B). The patient had no complications during or after the procedure. The size of the dissected tumor was 25 mm. The total procedure time was 90 min, and the rate-limiting step was the tumor dissection from the muscle layer. After the procedure, the patient complained of mild pain and soreness in the epigastric area (numeric rating scale score of 3), but this symptom improved after intravenous infusion of a proton pump inhibitor. After no oral intake for one day, oral intake progressed from water to a soft diet. The patient was discharged without any complications three days after the procedure. Histopathologically, the tumor cells had abundant eosinophilic cytoplasm and elongated nuclei (Fig. 3A). Immunohistochemistry revealed diffuse strong positivity for SMA (Fig. 3B) and negativity for C-kit (CD117). Two months later, EGD showed complete healing and replacement of the scar at the previous tunnel entry (Fig. 4A) and no definite defect in the cardia (Fig. 4B).
|

|

|

|
DISCUSSION
|
Most gastrointestinal SETs are asymptomatic, and were considered benign when small. In general, a pre-surgical histological diagnosis might not be necessary for large (diameter less than 3 cm) or symptomatic lesions that require resection of the lesion because of their malignant potential.5 Our patient was treated with STER because the tumor had grown compared to a previous examination, although still less than 3 cm in size. EUS is very useful in the diagnosis of an SET. If the SET is large and shows low echogenicity on EUS, a biopsy is required to determine if it is malignant.6 ESD is sometimes performed for diagnosis or treatment because a SET is difficult to diagnose with a conventional biopsy. Many approaches are used to remove a SET originating from the muscularis propria, including open and laparoscopic surgery and endoscopic procedures such as snare polypectomy, band ligation, ESD, endoscopic mucosal resection (EMR), and endoscopic full-thickness resection.1 However, these approaches have weaknesses. Surgery has a higher complication rate because it is more invasive and involves a longer hospital stay and more expense than endoscopic approaches. Conventional endoscopic therapy might not be suitable for treating esophageal and gastric cardia SETs originating from the muscularis propria due to technical difficulties related to the narrow submucosal space and endoscopic visual field.7 In addition, resection by EMR is often incomplete, and ESD has a higher risk of perforation when treating SETs originating from the muscularis propria.
Inspired by peroral endoscopic myotomy (POEM),8 recent studies have reported on the STER technique for resecting upper gastrointestinal SETs. STER combines ESD and POEM. STER procedural technique differs from the other approaches to SET treatment. To maintain the mucosa covering the tumor, a longitudinal mucosal incision is performed to create a mucosal entry into the submucosal space 5 cm proximal to the tumor during STER. After dissection of the tumor in the submucosal space, the mucosal entry is closed using hemostatic clips. However, a circumferential incision is made around the tumor during ESD, and the tumor is dissected from the submucosal and muscular layers. After ESD, a mucosal defect remains because the overlying mucosa is removed with the dissected tumor.
STER offers advantages of a very good view of the dissection through the submucosal tunnel, which can be easily insufflated with air,7 and submucosal tunneling maintains the integrity of the mucosal layer over the tumor. Even when perforation occurs, it is easier to close with endoscopic clips, helping to stop gastrointestinal tract leakage or secondary abdominal infections.9
We have described a case of gastric cardia SET originating from the muscularis propria layer. We performed STER because of the increase in the lesion size and location. The patient had no complications such as pneumothorax, subcutaneous emphysema, pneumoperitoneum, bleeding, or infection during or after the procedure.
Nevertheless, STER has several limitations. Unlike other endoscopic approaches, STER requires general anesthesia. Therefore, STER cannot be performed in the conventional endoscopic intervention unit. Second, complications such as pneumothorax, subcutaneous emphysema, pneumoperitoneum, bleeding, and infection can occur during and after the procedure.7 Prophylactic antibiotics and precise hemostasis are required because of the risk of bleeding and secondary infections. Third, the maximum resectable tumor size is restricted because of the limited tunnel space.10 Fourth, STER might be impossible due to the location of the lesion, such as in the upper esophagus.11
In conclusion, STER is a safe, economic, less invasive method for providing histopathology information and treating esophageal or cardiac SETs originating from the muscularis propria layer. Further studies with long-term outcomes and complications are needed to fully address the efficacy of STER.
|
References
|
| 1. | Ponsaing LG, Hansen MB. Therapeutic procedures for submucosal tumors in the gastrointestinal tract. World J Gastroenterol 2007;13:3316–3322. 
|
| 2. | Lee IL, Lin PY, Tung SY, Shen CH, Wei KL, Wu CS. Endoscopic submucosal dissection for the treatment of intraluminal gastric subepithelial tumors originating from the muscularis propria layer. Endoscopy 2006;38:1024–1028.
|
| 3. | Sumiyama K, Gostout CJ, Rajan E, Bakken TA, Knipschield MA. Transesophageal mediastinoscopy by submucosal endoscopy with mucosal flap safety valve technique. Gastrointest Endosc 2007;65:679–683.
|
| 4. | Sumiyama K, Gostout CJ, Rajan E, Bakken TA, Knipschield MA, Marler RJ. Submucosal endoscopy with mucosal flap safety valve. Gastrointest Endosc 2007;65:688–694.
|
| 5. | Jeong ID, Jung SW, Bang SJ, Shin JW, Park NH, Kim do H. Endoscopic enucleation for gastric subepithelial tumors originating in the muscularis propria layer. Surg Endosc 2011;25:468–474.
|
| 6. | Seo SW, Hong SJ, Han JP, et al. Accuracy of a scoring system for the differential diagnosis of common gastric subepithelial tumors based on endoscopic ultrasonography. J Dig Dis 2013;14:647–653.
|
| 7. | Gong W, Xiong Y, Zhi F, Liu S, Wang A, Jiang B. Preliminary experience of endoscopic submucosal tunnel dissection for upper gastrointestinal submucosal tumors. Endoscopy 2012;44:231–235.
|
| 8. | Inoue H, Ikeda H, Hosoya T, et al. Submucosal endoscopic tumor resection for subepithelial tumors in the esophagus and cardia. Endoscopy 2012;44:225–230.
|
| 9. | Li QL, Yao LQ, Zhou PH, et al. Submucosal tumors of the esophagogastric junction originating from the muscularis propria layer: a large study of endoscopic submucosal dissection (with video). Gastrointest Endosc 2012;75:1153–1158.
|
| 10. | Ye LP, Zhang Y, Mao XL, Zhu LH, Zhou X, Chen JY. Submucosal tunneling endoscopic resection for small upper gastrointestinal subepithelial tumors originating from the muscularis propria layer. Surg Endosc 2014;28:524–530.
|
| 11. | Kang MS, Hong SJ, Han JP, et al. Endoscopic submucosal dissection of a leiomyoma originating from the muscularis propria of upper esophagus. Korean J Gastroenterol 2013;62:234–237.  
|