

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Severe acute brain injuries (SABI) are characterized by a sudden and critical neurological crisis leading to disorders of consciousness, ranging from a vegetative state (VS) to a minimally conscious state.1 VS involves a lack of awareness and purposeful behavior, while a minimally conscious state signifies intermittent purposeful behaviors. In the US, approximately 4,200 persons annually enter VS,2 but epidemiological information is lacking in Korea. Patients in VS experience diminished quality of life, dependence on caregivers, and reliance on long-term care facilities, causing a significant socioeconomic burden.3456
The legalization of withdrawal of treatment in VS varies significantly between East and West, as well as among different countries, both in terms of whether it is legalized and the timing of such legalization. The intense debates leading up to the legalization of withdrawal of treatment in VS can be attributed to several factors. Firstly, within disorders of consciousness, including VS, there is clinical uncertainty regarding functional recovery, the accuracy of diagnostic tests, and the challenges in establishing consistent treatment strategies.17 Secondly, as shown in iconic cases from Quinlan and Cruzan over Terri Schiavo in the United States,8 there has been fierce debate from a bioethical perspective on whether accepting the withdrawal of treatment is morally justified. This debate includes considerations such as the importance of preserving life, respecting patient autonomy by following the patient's prior wishes, evaluating the quality of life, and the appropriateness of surrogate decision-making to support the patient's self-determination. Legal and procedural advancements in patient autonomy have emerged in some countries amidst these debates.9
In South Korea, the 2009 Severance Hospital case, in which the Supreme Court allowed a patient in a VS patient to forgo her ventilator treatment, reversed the medical community’s conservative stance of prohibiting patients in the VS from withdrawing treatment, which had been upheld since the 1998 Boramae Hospital case.10 During the debate in South Korea, healthcare professionals often used the concept of futility to justify withdrawal, but this concept has been challenged in medical ethics literature. Before enacting relevant legislation, following the Severance Hospital case, established guidelines based on academic societies, and the government formed a social consultation body to create grounds for respecting patient autonomy and legitimizing the process of surrogate decision-making.11 However, during the discussion, VS was ultimately excluded from candidates for the implementation of life-sustaining treatment (LST) decisions. Under the Act on hospice and palliative care and decisions on LST for patients at the end of life (hereafter, the LST Decisions Act) implemented in 2018,12 the provision for forgoing LST has been confined to patients nearing death.
Patient self-determination rights to refuse unwanted treatment has been expanded legally to some degree through the Act; however, subsequent legalization discussions on VS have essentially disappeared as well as various ethical and legal guidelines, creating a gap between legal requirements and treatment decisions in clinical settings, creating ethical concern,101314 Understanding the attitudes of clinicians and the general population (GP), apart from the legal permissible scope, regarding treatment decisions in such situations is essential to gather fundamental data for future societal discussions. Herein, we aimed to determine, via a case vignette, the attitudes of the GP and clinicians toward decisions regarding mechanical ventilator withdrawal in patients in the VS after SABI.
METHODS
Study design and participants
In 2022, we conducted an online survey in South Korea among GP and clinicians to assess their perspectives on treatment decisions. GP members aged 20 to 69 were reached out to between March 24 and March 30, 2022, via phone or text. We aimed for 500 participants, with a minimum of 420 for regression analysis, using quota sampling for sex and age categories. Clinicians from a university hospital participated between August 24 and September 23, 2022, with an anticipated 200 participants based on a 15% response rate from historical data. The final questionnaire was distributed to 1,576 clinicians, resulting in a response rate of 12.7%.
Questionnaires
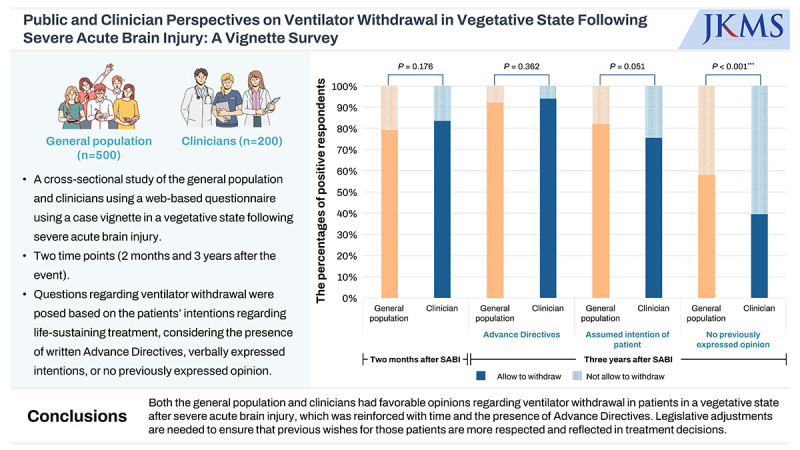
The authors developed scenarios and questionnaire items by drawing from a review of existing literature and engaging in discussions. One of the scenarios depicted a 75-year-old patient experiencing SABI and subsequently transitioning to a VS (Supplementary Method 1). The initial situation unfolded 2 months post-operation for cerebral hemorrhage in the intensive care unit, where participants were asked about allowing to withdraw the mechanical ventilator and the reason(s) for their responses. The second situation, 3 years later, depicted a patient using a home ventilator in a nursing hospital, and participants were asked about withdrawal again. The prognosis by attending doctor was given as follows; although it is difficult to expect recovery of consciousness or spontaneous breathing capacity, the patient could survive for several years if ventilator support were continued. Questions were posed based on the patients’ intentions regarding LST, considering the presence of written advance directives (AD), verbally expressed intentions, or no expressed opinions.
To investigate factors influencing attitudes, we gathered demographic data, health and LST decision-making experiences, and spirituality information from both the GP and clinicians. Specifically, questions on spirituality devised by the authors,15 covered transcendence beyond self and the present life, connection, the ultimate meaning of life, and engagement in spiritual practices. Responses were rated on a 5-point Likert scale. Additionally, social characteristics and clinical experiences were queried for the GP and clinicians, respectively.
Statistical analysis
Descriptive data summarized participant characteristics and responses. Categorical variables between groups were compared using Fisher’s exact test or Pearson’s χ2 test. Responses on a 5-point Likert scale were categorized as positive (4–5) or negative/neutral (1–3) attitudes. Variation in responses between the GP and clinicians based on the patient’s intention for LST at different time points was assessed. McNemar’s tests compared ventilator withdrawal responses between the 2-month and 3-year periods assuming the presence of an AD at 2 months post-SABI. These tests also compared each group’s attitude toward ventilator withdrawal at 3 years, considering the patient's intention for LST. Factors influencing attitudes toward ventilator withdrawal 2 months after SABI and their changes between two time points were separately analyzed for the GP and clinicians. All statistical analyses were two-sided (statistical significance at P < 0.05, 95% confidence interval). All the analyses were performed using STATA version 16.0 (StataCorp LP, College Station, TX, USA).
RESULTS
Characteristics of the participants
The characteristics of the 500 members of the GP and 200 clinicians are outlined in Table 1. Males represented 50.8% and 54.5% in each group, respectively, with distinct age distributions. Christians accounted for 33.6% of the GP and 41.0% of the clinicians. Clinician specialties included internal medicine (18.5%), pediatrics (17%), family medicine (9%), anesthesia and pain medicine (7.5%), emergency medicine (6.5%), general surgery (5.5%), neurology (3.5%), neurosurgery (2%), and other (30.5%).
Table 1
Characteristics of the GP and clinicians participating in this study
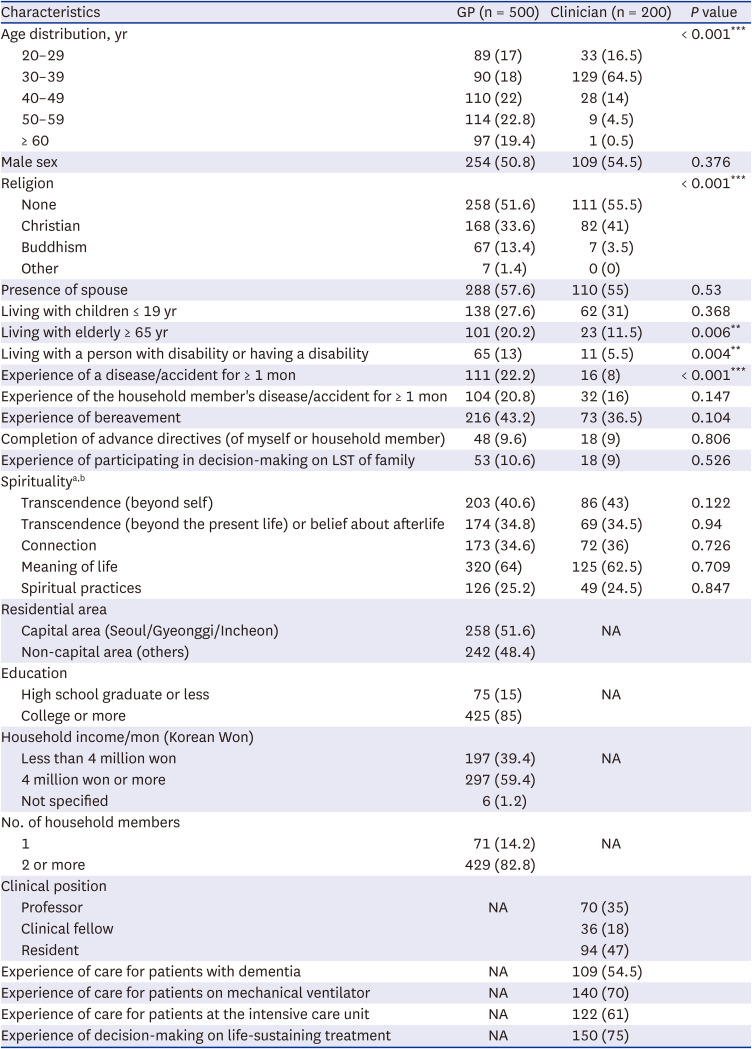
Values are presented as number (%).
GP = general population, LST = life-sustaining treatment, NA = not applicable.
aProportion agreeing (agree or strongly agree) with statements.
bQuestions regarding spirituality developed for this study were as follows: 1) transcendence (beyond self) by the question (“I believe that there is God or sacred in the world”), 2) transcendence (beyond the present life) or belief about afterlife by the question (“I believe that the existence of afterlife and it is as crucial as the present life), 3) connection by the question (“I closely connect to others, other life, God, sacred or nature”), 4) meaning the life by the question (“Life has the ultimate meaning”), and 5) spiritual practices by the question (“I try to participate in religious or spiritual practices or rituals”).
**P < 0.01, ***P < 0.001.
Attitudes toward mechanical ventilator withdrawal 2 months after SABI and reasons for the responses
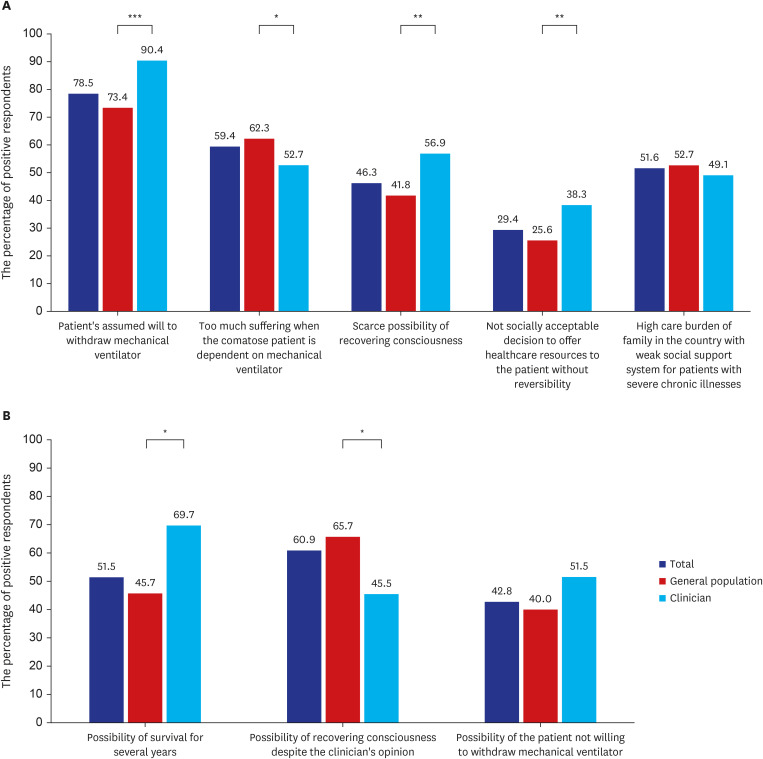
Two months post-SABI event, 79% of GP and 83.5% of clinicians responded that they allow to withdraw mechanical ventilator, with no significant difference between the groups (P = 0.176). Fig. 1A illustrates the reasons for allowance for ventilator withdrawal and the differences between GP and clinicians. While 90.4% of clinicians and 73.4% of the GP cited the patient’s presumed will as the main reason, its prevalence was significantly lower among the GP (P < 0.001). Conversely, the GP showed higher response rates for suffering (62.3%) compared to clinicians (P = 0.034) and had lower response rates for scarce chances of recovery (P = 0.001) and resource distribution concerns (P = 0.002) than clinicians. In Fig. 1B, clinicians were more concerned about the possibility of long-term survival (69.7% vs. 45.5% in GP, P = 0.016), whereas the GP more frequently cited the chance of recovery than clinicians (65.7% vs. 45.5% in clinicians, P = 0.038) as reasons for not allowing ventilator withdrawal.
Factors related to the negative attitudes toward mechanical ventilator withdrawal 2 months after SABI
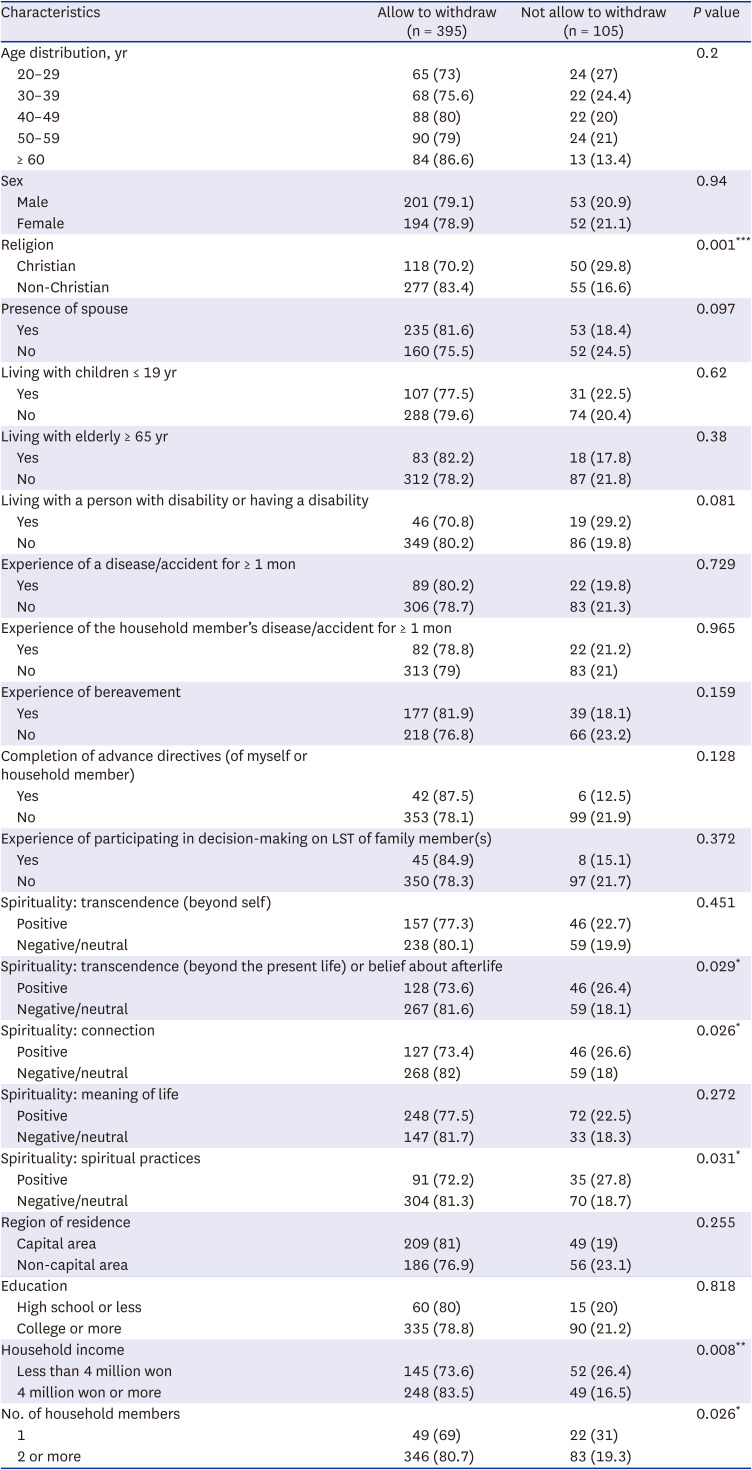
Table 2 and Supplementary Table 1 outline factors influencing GP and physician responses regarding the acceptability of mechanical ventilator withdrawal 2 months post-SABI. Among the GP, Non-Christians had a significantly higher rate (83.4% vs. 70.2%, P < 0.001) of allowing ventilator withdrawal. Positive attitudes toward “transcendence or belief about afterlife,” “connection,” and “spiritual practices” correlated with not allowing withdrawal (26.4% vs. 18.1%, P = 0.029; 26.6% vs. 18%, P = 0.026; 27.8% vs. 18.7%, P = 0.031, respectively). Lower household income and single-person households were associated with not allowing ventilator withdrawal. Age, sex, education level, family characteristics, and experiences related to illness and LST were not significantly associated with attitudes toward ventilator withdrawal in the GP.
Table 2
Related factors with attitudes toward withdrawal of mechanical ventilator at 2 months after severe acute brain injury in the general population (N = 500)
Contrarily, religion did not significantly influence clinicians' attitudes. Among clinicians, positive attitudes toward "meaning of life" correlated with not allowing withdrawal (20.8% vs. 9.3%, P = 0.034). Those independently completing the AD or having family members do so reported that they could allow ventilator withdrawal, while 18.1% without a completed AD considered it unacceptable (P = 0.048). Clinicians without prior LST discussion experience were more likely to see ventilator withdrawal as unacceptable compared to those with such experience (12% vs. 30%, P = 0.003). Among clinicians, demographic factors, family characteristics, illness experience, and experience in treating specific diseases were all not significantly associated.
Comparisons of attitudes toward ventilator withdrawal 3 years after SABI between the GP and clinician group by the patient’s intention on LST
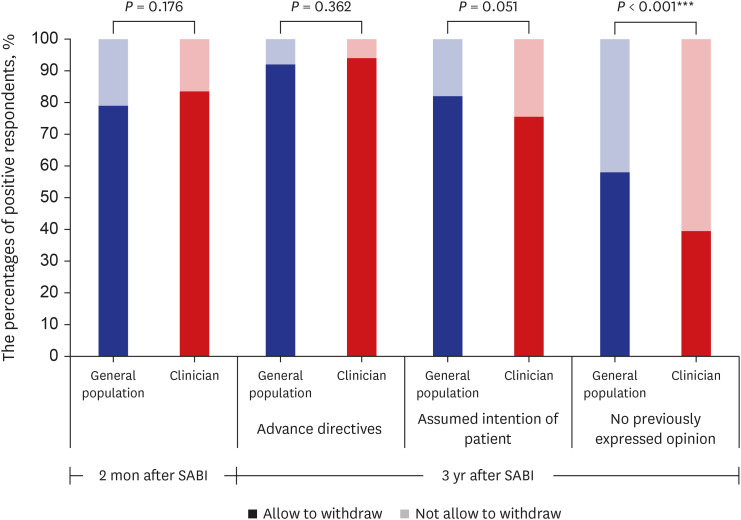
Fig. 2 shows the variation in ventilator withdrawal responses based on the patients’ LST intentions in the two groups. Among both GP and clinicians, the percentages of respondents allowing ventilator withdrawal were 92% and 94% with AD (P = 0.362), 82% and 75.5% with the patient's verbal intention (P = 0.051), and 58% and 39.5%, when the patient had not previously expressed an opinion regarding LST (P < 0.001), respectively.
Changes in attitudes toward ventilator withdrawal between 2 months and 3 years after SABI in the case with AD
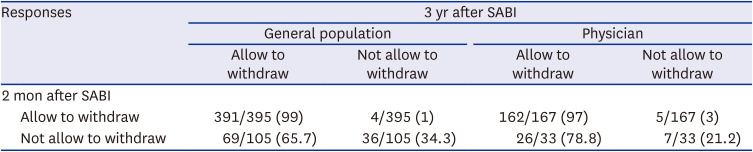
Assuming that AD is in place, Table 3 compares the GP and clinician attitudes toward ventilator withdrawal at 3 years and 2 months after SABI, respectively. Among the GP, 65.7% of those who initially deemed withdrawal unacceptable changed their stance to acceptable after 3 years, with 99% maintaining it as acceptable (McNemar’s chi-square = 57.8, P < 0.001). Also, 78.8% of the clinicians who initially regarded withdrawal as unacceptable changed to acceptable after 3 years, and 97% who initially deemed it acceptable maintained that stance (McNemar’s χ2 = 14.2, P < 0.001). Among the GP, shifts from negative to positive attitudes were associated with having a spouse (P = 0.011), children (P = 0.037), and neither having a disability nor having a disabled family member (P = 0.017). No factors were associated with changes in the clinicians’ attitudes (Supplementary Table 2).
Table 3
Changes in attitudes toward ventilator withdrawal between 2 months and 3 years with advance directives
Changes in attitudes toward mechanical ventilator withdrawal 3 years after SABI according to the patient’s intention on LST
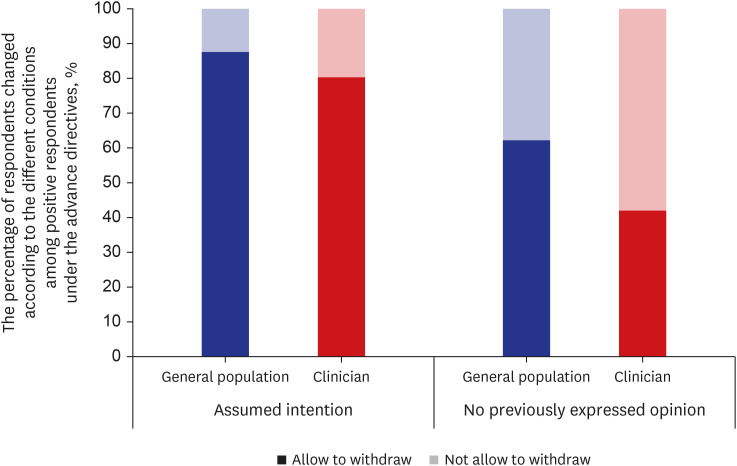
Fig. 3 shows a shift in attitudes toward ventilator withdrawal 3 years post-SABI based on patients’ expressions of intention on LST. Among 460 GP members with positive attitudes, 12.4% changed responses with the patient’s verbal intention (McNemar’s χ2 = 39.1, P < 0.001), and 37.8% changed with no previously expressed opinion of LST (McNemar’s χ2 = 162.4, P < 0.001). For 188 clinicians, 19.7% changed with verbal intention (McNemar’s χ2 = 37.0, P < 0.001), and 58% changed with no previously expressed opinion of LST (McNemar’s χ2 = 109.0, P < 0.001). Clinicians had notably higher response change rates than the GP.
DISCUSSION
To our knowledge, this is the first study to explore GP and clinicians’ attitudes toward ventilator withdrawal in VS cases after the LST Decision Act in Korea. The LST Decision Act in Korea permits the implementation of a decision to withhold or withdraw LST exclusively for patients who are in the process of dying, not clearly covering those in the VS and making them legally ineligible for LST decisions. Despite this, our study revealed a substantial number of both the GP and clinicians favoring withdrawal of mechanical ventilator 2 months after SABI, with increased support at 3 years.
Our study aligns with prior research in western countries, indicating a high acceptance of mechanical ventilator withdrawal after acute treatment among GP and clinicians. In a Norwegian survey, 66% of citizens supported treatment withdrawal based on patient preferences in a VS.16 While our rates were slightly higher, a global online study17 and a survey of US residents18 reported 40–50% support for withdrawal in VS cases. European surveys revealed that 66% of healthcare professionals accepted treatment withdrawal for VS, with 82% expressing a personal preference against being kept alive.19 In a Pan-Asia study regarding the perception of LST decisions in the intensive care unit, Korean clinicians were notably more conservative about withdrawal compared to other nations.20 Despite this, the notably high acceptance rate for ventilator withdrawal observed in our study, even more than in western studies, suggests the need for more open conversations about treatment decisions for patients in the VS.
Despite widespread support for ventilator withdrawal for patients in the VS, clinical decision-making may be difficult due to the diagnostic and prognostic uncertainties linked to decreased consciousness. The American Academy of Neurology1 recommends early identification of patient and family preferences. In the absence of AD, surrogate decision-making should consider predicted patient preferences and expected quality of life.7 Then, how are treatment decisions made for patients in the VS in clinical practice in other countries? In over 25% of the 67 European hospitals surveyed for end-of-life care for patients with traumatic brain injury,21 the decision to withhold or withdraw LST occurred 4–7 days after the SABI event in patients with poor prognoses but without brain death. Approximately 63% of these hospitals opted to withdraw mechanical ventilation. Similar trends were noted in Canada and the United States,222324 with 70–97% of SABI-related deaths resulting from LST withdrawal. In western countries, it is legally permissible for a patient to terminate the use of a ventilator, particularly in cases involving AD.925 Discussions on discontinuing treatment for patients in VS primarily focus on hydration and artificial nutrition rather than ventilators.2627 Among Asian countries, Taiwan’s Patient Self-determination Act in 2019 explicitly acknowledges the VS as an indication for determining LST decisions.28 A Japanese retrospective study revealed that withholding LST was common approach for patients with SABI showing poor neurological prognosis; however, an increasing trend toward treatment withdrawal was observed.29 In contrast, Korea's LST Decision Acts restrict the possibility of making LST decisions to the dying process, excluding patients in the VS from the legal decision-making framework. This restriction does not consider the prognostic uncertainty in patients in VS, which prohibits both withdrawing LST and withholding additional invasive treatments, which is not in line with the patient’s prior intentions. We suggest that a significant disparity in Korea’s legislative framework compared to other global practices is shown. However, there has been insufficient debate in Korea on LST decisions based on patient intentions for those in the VS since the enactment of the LST Decision Act, hindering future progress.
This study’s attempt to identify changes and differences in decision-making attitudes in response to various situations is notable. First, favorable attitudes toward ventilator withdrawal increased from 2 months to 3 years post-SABI, reflecting the impact of chronicity. The implementation of time-limited trials,30 which is a temporary treatment period to evaluate its effectiveness and decide on further steps on the stakeholder responses, is a recommended strategy in the field of neuropalliative care to enhance decision-related outcomes and alleviate a decision-maker’s anxiety when confronted with challenging choices in high-uncertainty situations, such as acute VS. However, the existing LST Decision Act does not permit such trials without assessing the dying process. Second, the study underscores the significant influence of AD on treatment decisions in patients in a VS,16 emphasizing clinicians’ reliance on AD despite practical challenges in extrapolating patient wishes. In Korea, the LST Decisions Act incorporates AD verification; however, legal assurance is limited to decisions deemed part of the dying process. This presents a challenge for patients in a VS, in whom determining the progression of the dying process is difficult. Improvements are required in the legal procedures for upholding decisions based on AD.
In this study, GP members’ inclination toward treatment withdrawal was significantly linked to religious and spiritual considerations, consistent with previous research.16171831 Specifically, Christian respondents were less accepting of ventilator withdrawal, possibly indicating a preference for more extensive treatment. However, unlike previous studies showing the association between clinicians’ religiosity and treatment decisions,32 our results did not show such an association. Limited data exist on the factors influencing clinicians’ attitudes; however, those with experience in AD or discussions on LST decisions were more favorable toward ventilator withdrawal. With recent legislation in Korea, clinicians lacking practical experience or adhering rigidly to a dichotomous approach to decision-making in which full treatment or “do-not-resuscitate” is considered, may make more conservative decisions.
Our study emphasizes the importance of data for shaping future policies on LST decisions for patients in the VS. Notably, there was significant agreement among the GP and clinicians, especially regarding ventilator withdrawal in patients with AD. This highlights the need for existing legislation to allow such decisions for patients in the VS, while respecting their autonomy. While legal regulations may not universally guide VS treatment decisions, Korean clinicians typically prioritize legal permissibility in end-of-life care.33 Therefore, expanding the areas approved by the current Act, including the VS, could be the next step to facilitate surrogate decision-making. This would be based on the values and preferences of individuals who do not wish to be kept alive by artificial means, rather than solely on medical judgment.
The differences in reasons for decision-making regarding ventilator withdrawal in this study also have clinical significance in understanding the different perspectives during decision-making discussions between clinicians and the patient’s family. Clinicians often express clinical nihilism due to uncertainty,7 while families may hold optimistic views.34 Reframing hope35 is crucial in neuropalliative care communication. While clinicians should offer sufficient prognostic information, guiding families toward shared decision-making and prioritizing the patient’s values over fixating on medical recovery possibilities, is also essential.25
This study has several limitations. First, the findings from clinicians were based on a specific sample from a tertiary hospital, limiting generalization to other settings. Although we attempted to recruit clinicians with diverse specialties and varying lengths of clinical experience, the responses may have been influenced by the culture and organizational hierarchy of the institution, as well as the clinicians’ experiences in resolving similar cases within the institution. Second, distinguishing VS from other consciousness disorders may be challenging for both GP and clinicians. Despite presenting detailed case vignettes to minimize bias, an insufficient understanding of the clinical situations may have influenced the responses. Third, as we did not ask for detailed reasons regarding responses about ventilator withdrawal at the 3-year mark, difficulty in understanding the reasons behind changes in opinion from the 2-month mark to the 3-year mark may limit the interpretation. Fourth, the spirituality assessment tool lacks validation from established psychometric assessments or widely recognized standards, raising concerns about its reliability. Finally, we only used a simple comparative analysis to evaluate factors associated with attitudes toward decision-making in patients in VS.
In summary, although there are some limitations to generalizing the study, the high acceptance rates for withdrawing ventilators observed in both the GP and clinicians in this study, which were strengthened over time with the existence of AD, suggest the need to facilitate the currently stagnant discussions on this issue. Legislative adjustments are needed to ensure that previous wishes for those patients in a VS are more respected and reflected in treatment decisions.
 XML Download
XML Download