

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Dietary education is a component of the “Nutrition Care Process,” an integral standard process in dietetic services [1]. Effective dietary education reduces the risk of diseases by making nutrition knowledge accessible and practical in everyday situations [2]. Utilising educational tools for nutrition instruction during counselling, particularly with patients who receive individualised counselling, has been demonstrated to improve adherence to dietary recommendations [345]. In addition, it also helps patients understand dietary advice better [678]. Having adequate nutrition knowledge and understanding are necessary components for preventing and managing non-communicable diseases that are linked to unhealthy diets, such as obesity [9].
The effectiveness of nutritional counselling depends on various factors, such as offering personalised dietary advice, receiving feedback and support from dietitians and using educational tools during counselling sessions [10]. Nonetheless, a local study indicated that healthcare professionals were facing obstacles in providing effective dietary education due to unappealing and unlocalised pamphlets, and limited nutrition education materials at the primary healthcare clinic [11]. To accommodate the literacy level of the target population, nutrition education tools need to be adjusted accordingly. A study that employed a visual educational tool among individuals with lower literacy individuals demonstrated that they could formulate healthier eating plans with a higher Healthy Eating Index compared to another group taught using a standard system [12].
It has been reported that the public frequently misinterprets specific terms found in nutritional guidelines, such as “serving size” [13]. Consequently, it is important to provide educational tools that can help patients accurately estimate food portions [1415]. Traditionally, dietitians have used physical-based nutrition education tools during counselling sessions, such as pamphlets, flip charts, healthy plate models, food pyramids, food models, and meal planning sheets. However, these tools may lose their effectiveness as technology advances. Dietitians who fail to embrace or understand the digital dietary landscape are at risk of falling behind [16]. There is a lack of local research on how dietitians utilise nutrition educational tools in their practice. Therefore, this study aimed to investigate the existing types and limitations of the nutrition education tools that are being used and to seek dietitians’ perspectives on digital nutrition educational tools. Data from this study can be utilised to create nutrition educational tools that accommodate dietitians’ preferences and patients’ needs.
SUBJECTS AND METHODS
Study design and population
Fifteen dietitians were recruited using a convenience sampling method from selected healthcare facilities in central Malaysia, i.e., the Klang Valley, including 7 public hospitals, 5 teaching hospitals, and 3 primary care clinics. In this study, “health clinics” refer to government facilities that provide fundamental healthcare services such as preventive care and treatment for common illnesses. “Public hospitals” are tertiary hospitals with specialised medical facilities managed by the government. Finally, “university hospitals” are institutions affiliated with universities or medical schools that provide medical care to patients while also serving as training grounds for healthcare professionals.
The subjects were invited to participate in this study through social media such as WhatsApp Messenger and email. Klang Valley is the most populated city in Malaysia with the greatest number of public hospitals and experienced servicing dietitians [17]. Only dietitians with a minimum of 5 years of experience in both outpatient and inpatient settings were eligible for the study. Those who worked in the food service department were excluded as they usually do not provide dietary counselling to patients.
A research dietitian with initial training in qualitative study methods used semi-structured face-to-face interviews to conduct this qualitative study. The study was conducted following the ethical standards of the Medical Research Ethics Committee of Universiti Kebangsaan Malaysia (reference code: UKM PPI/111/8/JEP-2020-219). All participants were briefed on the purpose and procedures of the study, and they signed a written informed consent form before participating in this study.
The Interviews
To gain a comprehensive understanding of the subject matter, this study utilised a qualitative approach that allowed for an in-depth analysis of the interviewees’ responses [18]. The interview guide was developed using research questions and The Design and Development Research Model [19]. A pilot study was conducted among 5 dietitians to pre-test the questions, leading to necessary amendments before the actual interviews. The participants of this study were dietitians from 5 selected public hospitals and primary care clinics in the Klang Valley, all of whom met the study criteria. The participants were asked 4 key questions: (i) the nutrition education tools they used during dietary counselling sessions, (ii) the importance of using nutrition education tools during dietary counselling sessions, (iii) the limitations of existing educational tools, and (iv) their preferences for nutrition education tools during dietary counselling. Individual interviews were carried out at the participants’ workplaces between January and February 2020, using a Xiaomi Redmi Note 4 mobile phone to record the sessions. On average, each interview session lasted 30 min. The interview questions are listed below:
1. What nutrition education tool do you currently use in your dietary counselling?
2. In your opinion, what is the importance of using nutrition education tools during dietary counselling?
3. Are there any limitations in the current nutrition education tools you use?
4. What is your preference for nutrition education tools to be used during dietary counselling?
Data coding and analysis
The interview data was transcribed verbatim and input into the NVIVO 12 Plus software program for qualitative analysis. An inductive thematic analysis of the data was used, whereby the data was coded through an open coding process based on the research questions. Subsequently, 2 other researchers conducted a second round of coding to consolidate codes and identify the main themes relevant to the research questions. This was further reviewed and independently checked by another researcher.
Trustworthiness
Several methods were used to ensure the reliability and quality of the data in this investigation. To begin with, the participants’ trust and rapport were maintained throughout the research process, beginning with the initial contact to the completion of the interviews. Secondly, after performing 5 preliminary interviews, the primary researcher engaged in discussions with pertinent supervisors to consider the potential modifications to probing and interview questions. The transcripts texts and audio recordings were re-examined to fully understand the interactions. The final step involved ongoing peer debriefing among co-researchers to ensure consensus in data interpretation and data analysis.
RESULTS
Study participants’ general characteristics
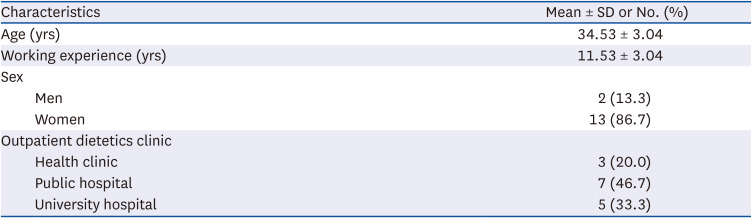
In this study, data saturation was attained following the interviews of 15 participants. These participants were based on the concept of data saturation, which is the point at which no additional pertinent information surfaced during the interviews [20]. Table 1 shows the socio-demographic profiles of participants in this study. Most of the participants were women (87%) and held at least a bachelor’s degree qualification. Their ages ranged between 32 and 44 yrs, and they had an average of 11 yrs of experience working in an outpatient dietetic clinic.
Nutrition educational tools currently used in dietary counselling
Table 2 shows descriptions of several types of nutrition education tools, as well as their uses and representativeness. Among the study participants, the Malaysian Healthy Plate model and pamphlets were the most widely used nutrition education tools (100%), followed by household measurement tools (67%), flip charts (60%), menu planning sheets (47%), and food models (33%). The least used resources were digital tools (20%). All the participants believed that the Malaysian Health Plate Model can improve awareness of food portion size, making it the most frequently used nutrition education tool.
Table 2
Types of nutrition education tools and participants’ quotes illustrating their use of these tools
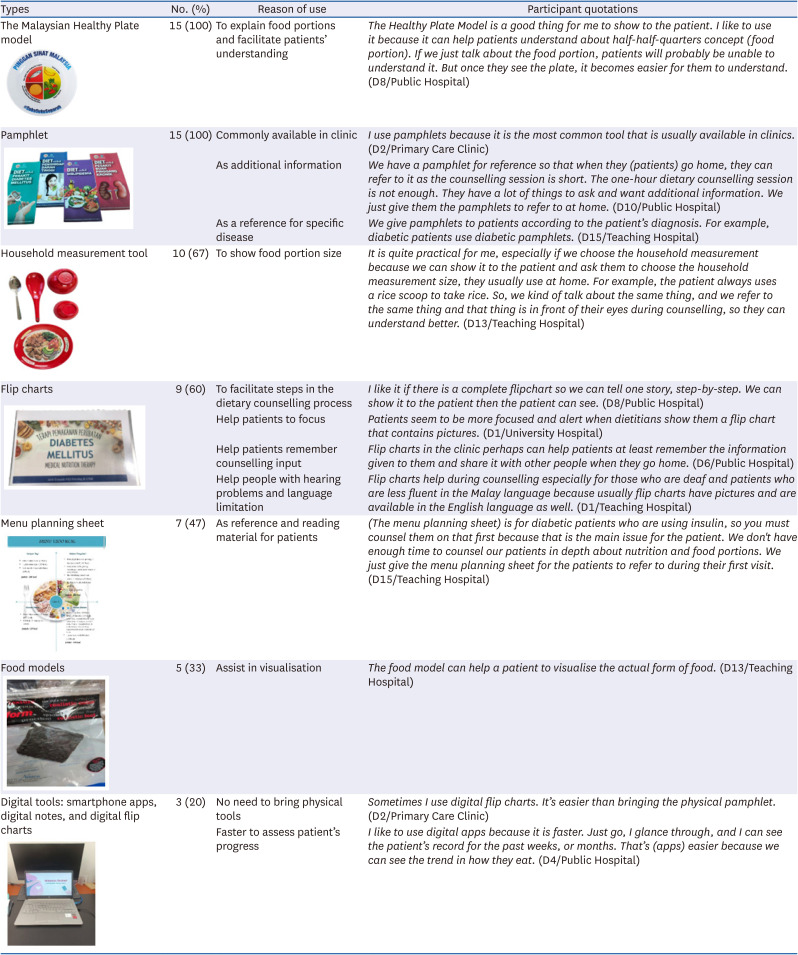






The participants in this study indicated that practical nutrition education tools, such as household measurement tools, were important since they could help patients comprehend food portions better if they also used the same tool at home. Furthermore, pamphlets were frequently used because they are typically given out to patients at dietetic clinics and customised to specific medical diagnoses such as diabetes. Flip charts were used by more than half of the participants as they found it helped to stage the flow of dietary counselling and increase patients’ concentration and memory retention of information gained from the sessions. Participants also mentioned that it helped deliver dietary interventions to patients who had language barriers. Menu planning sheets were reported as another tool that is frequently utilised and provided to patients as reference materials after the counselling session. As for food models, participants described that they assist patients in visualising actual food portion sizes.
Findings from this study indicate that digital tools are the least used nutrition education tools by the participants. However, one of the participants said that she preferred to use digital flip charts because they are more portable than physical flip charts. Another participant described the convenience of using digital nutrition apps to track patients’ progress. However, according to one of the participants, she doubted the invalidated existing nutrition smartphone application content.
Importance of nutrition education tools during dietary counselling
Table 3 shows the input from participants that supports the sub-themes that emerged regarding the importance of nutrition education tools. The first sub-theme identified is timesaving in which participants expressed that the shortage of dietitians especially in primary care health clinics resulted in time constraints in giving full dietary advice to the patient. Furthermore, one primary health care clinic dietitian is reported to oversee many clinics in each district thus, strengthening the need for using nutrition education tools that can expedite the dietary counselling process and help save time.
Table 3
Illustrative participants’ quotes regarding their perceptions of the importance of nutrition education tools
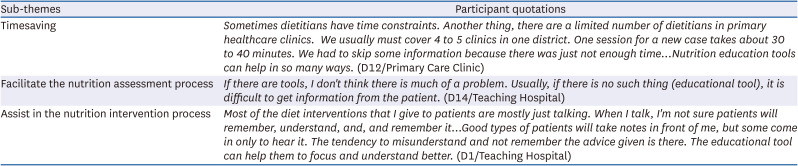
Another sub-theme that emerged from the analysis was nutrition education tools facilitating nutrition assessment and intervention during dietary counselling. Participants described that nutrition education tools are essential for collecting information to evaluate patients’ nutritional status. Participants also felt that the usage of the tools is crucial in dietary counselling as they increase patients’ attentiveness as well as understanding.
Limitations of the existing nutrition educational tools
Five sub-themes were found within the existing nutrition education tools theme (Table 4). The first sub-theme highlighted is the difficulty in visualisation of portion size. According to the participants, the Malaysian Healthy Plate Model that emphasises the concept of quarter-quarter-half serving is unclear for some patients. For example, patients feel unsure of the actual food portion to fill in a quarter-quarter-half space as it is commonly assumed that one portion is only for one type of food such as rice. This is despite that the first quarter section portion is also applied to all cereals and starchy vegetables. In addition, participants cited that some patients were unable to estimate the portion of food as the printed food photos on the Malaysian Healthy Plate Model did not represent the actual size of the food. Moreover, the size of the Malaysian Healthy Plate Model used by dietitians was different from the size of the plate patients used at home. Thus, it is difficult for patients to visualise the message delivered by dietitians during dietary counselling sessions. In the Malaysian Healthy Plate Model, “quarter-quarter half” represents a recommended division of a meal plate, where one-quarter is allocated to protein sources, another quarter to carbohydrates or grains, and half the plate to fruits and vegetables, promoting a balanced and healthy diet [21].
Table 4
Illustrative participants’ quotes regarding their experience with the limitation of existing nutrition education tools
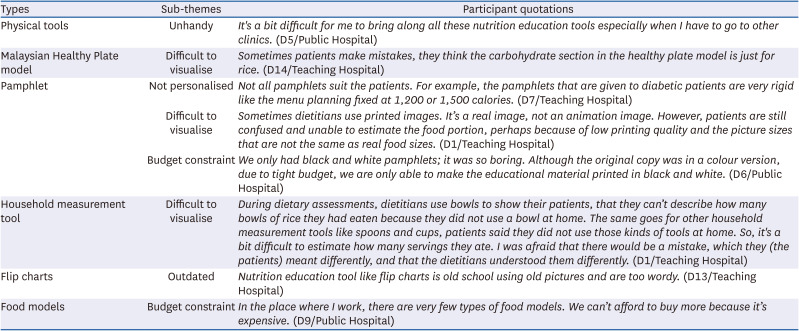
The second sub-theme is the cost of educational tools currently used in dietetic clinics. Participants in this study stated that the types of food models available in dietetics clinics are limited because food models are generally expensive, and most clinics have limited budgets. The same situation applies to pamphlets, which were first produced in colour and distributed in dietetics clinics. However, due to financial limitations, they were only printed in black and white. Consequently, participants felt that it would make the pamphlets less attractive to their patients.
The next sub-theme identified in this study is that participants reported it was challenging to use physical nutrition education tools during numerous trips to health clinics. They acknowledged that even though the pamphlet was customed to various medical diagnoses, it can be unsuitable for some patients as it is not personalised based on their actual energy needs. On the contrary, the menu planning pamphlet is prepared based on a general range of calorie needs (i.e., 1,200 kcal, 1,500 kcal and 1,800 kcal).
Additionally, participants cited that the existing flip charts in their clinics were outdated as they were based on old pictures and references. Moreover, it was felt that the existing materials were wordy and that their patients would not be interested to read them.
Preferred nutrition education tools during dietary counselling
All participants stated that they preferred digital tools and suggested that more digital tools should be developed in Malaysia. Smartphone apps were described not only to simplify dietitians’ tasks but also to ease the overall experience for patients.
“Nowadays everyone uses a smartphone. Many people like to snap food pictures before eating. Meaning that we (dietitians) can ask the patient to log in their daily food intake in the apps. When they come to see us, they don’t need to recall anything, we can review directly from the apps.” (D1/Teaching Hospital)
Another participant recommended using a digital flip chart, perceiving that it would make dietary counselling sessions more engaging and enjoyable compared to using old-fashioned flip charts.
Features of digital nutrition education tools desired by study participants
Six sub-themes were identified in the discussion on the features that should be included in a digital tool for nutrition education (Table 5). Firstly, the participants described that digital tools could serve to provide instant monitoring and feedback from dietitians to patients. It is believed that the delivery of current dietary interventions should be more prompt rather than delayed until a physical clinic appointment.
Table 5
Illustrative participants’ quotes regarding their preferred feature of the digital nutrition education tool
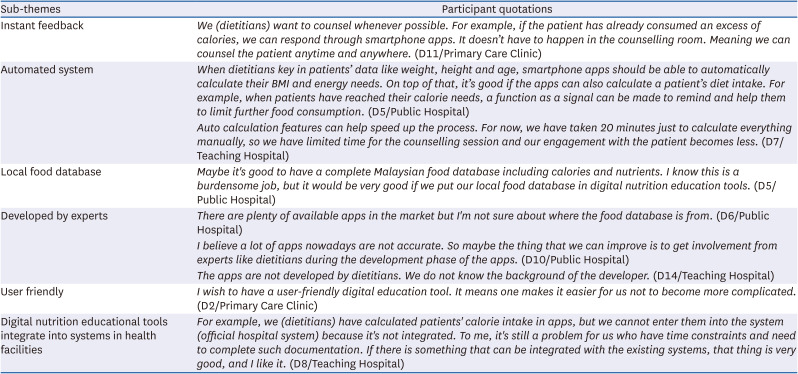
The second suggested digital feature was an automated calculator that could obtain important nutritional information. Participants expressed that mobile apps should have the capability to automatically calculate patients’ body mass index (BMI) and energy requirements, thereby allowing more time for dietitians to focus on giving counselling to the patient. In addition, the participants prompted that digital nutrition education tools be embedded with the local food database.
The next sub-theme involves the development of digital nutrition education tools by experts in the field such as dietitians and nutritionists. Participants claimed that available apps in the market are often misleading, and this might be due to the lack of legitimate experts included in the development process.
Finally, participants added that the ability of a nutrition education tool to be able to integrate with healthcare databases was crucial. Dietitians have already started to use digital apps to determine patient’s energy requirements. However, they need to manually document the information retrieved from the apps into their respective hospital databases which can be time-consuming. Thus, participants would prefer that future apps be connected to hospital databases.
Advantages of digital nutrition education tools
Table 6 summarises the perceived advantages of digital nutrition education tools mentioned by the participants. It has been perceived that the functions of digital nutrition education tools available in mobile apps help dietitians obtain initial information about their patients before the dietary counselling session begins. Secondly, participants cited that the availability of digital nutrition education tools may improve communication between dietitians and patients. Thirdly, digital nutrition education tools are believed to be able to accelerate the dietary counselling process and simultaneously save time. Furthermore, patients can complete food diaries via digital apps to meet their dietitian and thus, expedite the nutrition assessment process.
Table 6
Illustrative participants’ quotes regarding their perceptions of the advantages of digital nutrition educational tools
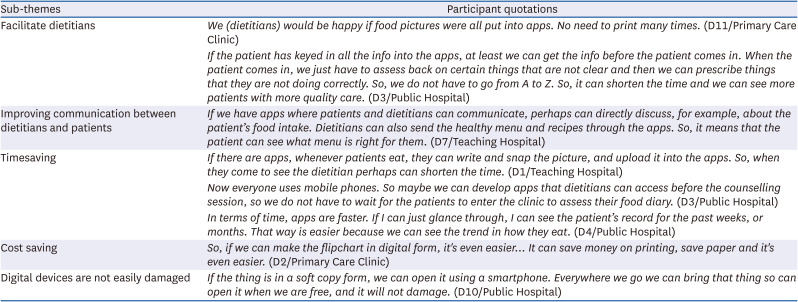
Concomitantly, participants narrated that digital nutrition education tools would be more cost-effective by reducing paper and printing costs that were previously used to develop flip charts and other education tools. Lastly, digital nutrition education tools are believed to be easily accessible and not vulnerable to damage as compared to physical nutrition education tools.
DISCUSSION
This qualitative study provides a comprehensive exploration of dietitians’ perspectives on nutrition education tools, considering the types of tools that they use as well as their importance and limitations. In addition, we explored in depth the participants’ recommended features in digital nutrition education tools.
Most of our participants favoured printed pamphlets as they perceived it was the most convenient option and was readily available at their clinics. Moreover, the pamphlet was given to patients as take-home messages. Similarly, another qualitative study among multidisciplinary clinicians on challenges in implementing Mediterranean dietary patterns found that participants also agreed that handouts could be supporting materials, especially during short consultation sessions due to time and resource constraints [22]. Thus, printed education materials can benefit healthcare providers by expediting the consultation process as well as allowing them to review the information at their convenience and improve their understanding.
In this study, the participants believed that The Healthy Plate Model, household measurements, food models, pictorial pamphlets, and flip charts to be able to increase patients’ concentration during dietary counselling sessions. The inclusion of visual elements in teaching aids is encouraged because it can increase audience engagement, attract attention, and simplify complex knowledge [23]. Furthermore, it was demonstrated that colourful education pamphlets reduced patients’ absenteeism rates for dietary intervention [24]. The Kiel Obesity Prevention Study that was conducted in Germany found that pictorial foods and visual food models used in dietary counselling sessions had improved the nutrition knowledge of their study participants [25]. Pictorial-type education tools can serve as a guide to patients in determining the appropriate food portion and the type of diet to comply with [262728].
Our study participants revealed their uncertainty about the available apps in the market. Issues related to their accuracy, reliability, and trustworthiness become the main concern. It was reported that app users preferred expert-developed apps as they believed it could affect the accuracy and reliability of nutrition advice provided [29]. The healthcare professional mentioned that the important criteria for selecting an app were ease of use, apps being free of charge and validation [30]. Significant barriers to using the nutrition apps reported in the previous study include inaccurate database nutrition output and a lack of local food composition database [31]. In addition, our study found that the digital nutrition education tool needs to be user-friendly for dietitians to utilise and to conduct their work more efficiently compared to the traditional method. It was reported that perceived accessibility, usefulness, price value, and trust affect the adoption of the app in dietetic practice [32]. Findings from our study suggest that it is crucial to involve dietitians during the development process of apps as well as test their usability with local end users including both dietitians and patients.
In this study, although most of the participants had not initiated the use of digital nutrition education tools in their dietary counselling sessions, they highly recommended the development of these tools for future use. Text messaging programs delivered by dietitians have been reported to be effective in improving eating behaviours among people with cardiovascular diseases [3334], and web-based nutritional interventions have helped in improving eating behaviours in patients with obesity [35] and type 2 diabetes mellitus [36]. Moreover, dietary interventions using community-based technologies such as mHealth and eHealth have shown the ability to improve nutritional behaviours among people with type 2 diabetes mellitus [37], hypertension [38], and chronic kidney disease [39]. A quasi-experimental study examining the effectiveness between graphic persuasive games and non-graphic persuasive games towards changes in healthy food choice attitudes among second-year students found that the treatment group scores were significantly higher than the control group [40]. A randomised controlled trial among older adults found that web-based health education tools are more cost-effective compared to pamphlets [41].
In this study, participants thought that the audio and visual features of digital communication used in digital nutrition education tools could improve communication between dietitians and patients. A study assessing an automated and interactive telephone program developed by dietitians to enhance dietary compliance with the Dietary Approach to Stop Hypertension among American patients with hypertension demonstrated notable enhancements in dietary quality, increased fibre intake, reduced daily energy consumption, improved medication adherence, and a decrease in blood pressure [42].
Our participants also thought that digital education tools could provide instant intervention feedback to patients rather than delaying it until a physical clinic appointment. The innovation of natural language processing, artificial intelligence, and machine learning have led to the increased use of information technology in healthcare such as chatbots which can provide lifestyle and medical advice through real-time feedback [43]. For instance, the Academy of Nutrition and Dietetics Health Informatics Infrastructure is an electronic web-based tool that allows dietitians to monitor and evaluate nutritional care outcomes remotely [44]. Digital nutrition education tools also have the advantage of being time-efficient, which may save time during dietary counselling sessions [45]. Time efficiency was reported as one of the key user requirements during the development of the TreC-Lifestyle mobile app nutrition education [46].
In this study, the participants felt that the current local population is prepared for digital nutrition education tools due to the increasing use of mobile phones. The Malaysian Communication and Multimedia Commission 2021 report shows that nearly all Malaysians use smartphones (94.8%) [47]. A study in Malaysia shows that 53.6% of smartphone users have downloaded health-related apps for lifestyle management [48].
This study is subject to a limitation in participant selection. Specifically, participants were exclusively recruited from government hospitals, teaching hospitals, and health clinics within the main city of the country. As a result, our findings only reflect the perspectives of dietitians from these settings which may limit our insights into the experiences of dietitians working in rural areas. This limitation highlights the necessity for further investigation among dietitians in rural settings, where internet access and usage are likely to be less prevalent. Nevertheless, the findings of our study on the perspectives of dietitians regarding digital nutrition educational tools in Malaysia present significant implications for dietitians in diverse geographical regions. These implications encompass cross-cultural insights, the adaptation of educational tools, professional development, and policymaking. Through comparative analysis of their local contexts, dietitians can identify common challenges or opportunities in implementing similar tools.
In conclusion, dietitians in this study believed that nutrition education tools are crucial in assisting dietary counselling, facilitating the nutrition assessment process, and saving time. Most dietitians in this study are using physical nutrition education tools due to their availability and ease of use. Nonetheless, some of the physical nutrition education tools were perceived as immobile, impersonalised, outdated, and modified to lower quality due to budget constraints which could limit the efficacy in delivering the nutrition care process. Dietitians in this study thought that digital nutrition educational tools could overcome these limitations. To ensure the trustworthiness of these digital applications, dietitians perceived that the digital nutrition education tools must involve the end users in the development process which includes dietitians and patients. The findings of the current study serve as a reference for the development of up-to-date nutrition education tools for dietitians in Malaysia. Furthermore, these findings can serve as a valuable resource for dietitians worldwide seeking to enhance their practice with the latest educational tools and methodologies.
 XML Download
XML Download