

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Aging is accelerating in many countries and is emerging as a significant social problem today. The baby boomer generation in Korea, representing approximately 15% of the population born between 1955 and 1963 after the Korean War, commenced their transition into the elderly population in 2020 [1]. Moreover, while life expectancy is gradually increasing, healthy life expectancy is showing a decreasing trend [2], raising the problem of increasing overall financial expenditure towards social security, taxes, and the burden of medical expenses and long-term care costs for the elderly. Accordingly, there is a need for various healthcare policies that could extend healthy lifespans at the national level. Previous studies have shown that health care in middle age affects the quality of life in old age and that maintaining certain health behavior patterns in middle age can lead to a satisfying life even after the seventh decade of life [3]. Since the majority of Korean baby boomers are still in middle age, it is important to raise awareness of their future health in old age and provide appropriate approaches to healthier lifestyles.
Healthcare for the elderly aims to not only prolong their lifespan but also to enable them to lead an independent life and be active in society. This necessitates the preservation of mental, social, and physical health starting from middle age. Given the established association between subjective health status and mortality [4], it should be emphasized that mental health plays a crucial role in determining the overall health status of the elderly population. Studies have shown that higher levels of perceived stress are associated with cognitive decline and an increased risk of cognitive impairment in later life [5]. Mental disorders, including depression and post-traumatic stress disorder, elevate the risk of cardiovascular disease [46]. A meta-analysis of studies assessing the link between perceived psychosocial stress and stroke risk in adults revealed that perceived psychosocial stress was independently associated with an elevated risk of stroke [7]. The compounding impact of life stress, together with restricted psychosocial support in middle age, correlates with detrimental consequences in the psychological, biological, and health-related quality of life domains [8]. Stress management is crucial for the health of middle-aged individuals, given their exposure to diverse stress factors [9].
The interaction between diet and mental health is bidirectional, wherein changes in the diet may affect mental disorders by affecting mood, and conversely, mental disorders may influence dietary habits over time [1011]. The Mediterranean diet is an eating pattern characterized by high consumption of fruits, vegetables, legumes, nuts, whole grains, olive oil, fish, and seafood, low consumption of high-fat dairy and red meat, and moderate consumption of alcohol [12]. Adherence to the Mediterranean diet has been reported to be favorably associated with a lower risk of overall mortality, cardiovascular diseases, cancer, and mental disorders, including Parkinson’s disease and Alzheimer’s disease. Adopting a Mediterranean diet peri-retirement age contributes to promoting healthy aging and has been associated with the prevention and alleviation of depression and improvement in cognitive abilities [131415]. Previous research in primates suggests that the Mediterranean diet may be an effective intervention for psychosocial stress [16]. Another study in humans found that a Mediterranean diet buffered the association between high-stress levels and poor executive function [17]. However, research on the relationship between the Mediterranean diet and psychosocial stress remains insufficient.
This study aimed to examine the dietary habits of Korean baby boomers by utilizing extensive national data and to analyze the association between adherence to the Mediterranean diet and levels of psychosocial stress. The goal was to offer evidence that could contribute to the development of strategies for mental health management in elderly life.
SUBJECTS AND METHODS
Subjects
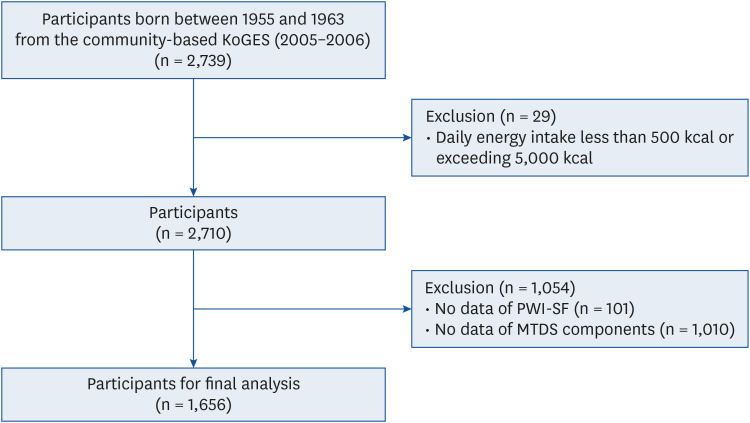
This was a cross-sectional study using 2005–2006 data from the community-based Korean Genome and Epidemiology Study (KoGES, 2005–2006). The KoGES is a cohort study of Korean men and women living in the Ansan (urban) and Anseong (rural) regions of South Korea [18]. Both the semi-quantitative food frequency questionnaire (SQFFQ) and psychosocial well-being index-short form (PWI-SF) data were exclusively available in the second follow-up survey conducted in 2005–2006. The analysis involved 1,656 adults (889 men, 767 women) born between 1955 and 1963. Subjects with a daily energy intake of less than 500 kcal or exceeding 5,000 kcal and those who did not respond to the SQFFQ and PWI-SF questionnaires were excluded (Fig. 1). Approval for this study was obtained from the Institutional Review Board (IRB) of Sungshin Women’s University (IRB No. SSWUIRB-2021-017).
Mediterranean-type diet score (MTDS)
This study utilized a SQFFQ, which comprised 106 items and underwent a revision in 2004. The revision was based on the SQFFQ developed and validated in 2001 by the Korea Disease Control and Prevention Agency (KDCA) [1920]. The SQFFQ was employed to evaluate the participants’ usual dietary intake. The questionnaire featured nine levels of food frequency (rarely, once a month, 2–3 times a month, 1–2 times a week, 3–4 times a week, 5–6 times a week, once a day, twice a day, 3 times a day) and three levels of serving size (less than reference, reference, and more than reference) over the past year. The serving sizes were determined based on the actual consumption amounts reported by Korean adults aged 40–69 yrs, derived from the 24-h recall data of the Korea National Health and Nutrition Examination Survey (KNHANES).
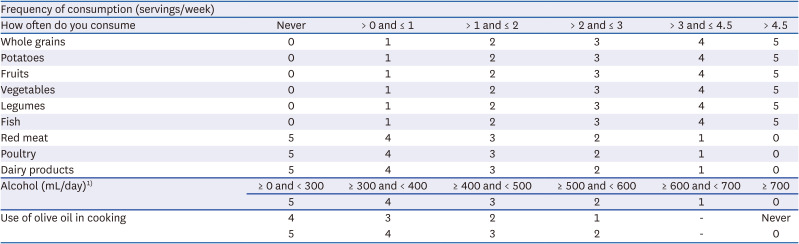
To assess adherence to the Mediterranean diet, we utilized the Mediterranean diet tool based on the Mediterranean diet score (MDS) developed by Panagiotakos et al. [21] and tailored for the community cohort data [22]. The MTDS comprises 11 components: Whole grains, potatoes, fruits, vegetables, legumes, fish, red meat, poultry, dairy products, alcohol, and olive oil. Table 1 details the MTDS components and scoring criteria for this study. Scores for the 11 food group items were aggregated to calculate the MTDS, ranging from 0 to 55, wherein higher scores reflect better adherence to the Mediterranean diet. The consumption of food groups was translated into weekly intake frequency. For the calculation of the MTDS, individuals are assigned points based on their consumption of whole grains, potatoes, fruits, vegetables, legumes, and fish: 0 points for no consumption, 1 point for 0–1 serving/week, 2 points for 1–2 servings/week, 3 points for 2–3 servings/week, 4 points for 3–4.5 servings/week, and 5 points for more than 4.5 servings per week. Conversely, scores were allocated on the inverse scale for the intake of red meat, poultry, and dairy products. Data on alcohol consumption and olive oil were assessed through a dietary habit questionnaire, not the SQFFQ. Daily alcohol intake (mL/day) was calculated by converting the average amount of ethanol consumed per day (g) according to the type and amount of alcoholic beverage consumed. In this study, unlike existing scoring methods that assign the lowest score when alcohol consumption is zero, the criteria were adjusted to evaluate low alcohol consumption including zero as higher scores: 0 points for more than 700 mL/day, 1 point for 600–700 mL/day, 2 points for 500–600 mL/day, 3 points for 400–500 mL/day, 4 points for 300–400 mL/day, and 5 points for less than 300 mL/day. This adjustment was derived based on findings from an earlier domestic study [23] which suggested that moderate alcohol consumption did not demonstrate a discernible benefit in lowering all-cause, cancer, and cardiovascular disease associated mortality. Furthermore, this adjustment is deemed reasonable as certain studies [24] consider regional variations in their calculation of the MDS and, as a result, occasionally exclude alcohol consumption as a criterion. Consumption of olive oil was assessed by asking about the type of oil used in four Korean cooking methods: ‘frying,’ ‘stir-frying,’ ‘Buchim’ (Korean pancakes), and ‘Muchim and Namul’ (Korean salads, cooked and seasoned vegetables). The use of olive oil in all four cooking methods was assigned 5 points. The use of olive oil received 4 points if it was used in three cooking methods, 3 points for two cooking methods, and 2 points for one cooking method. If no olive oil was used, a score of 0 was assigned. Kimchi and pickles were omitted from the vegetable group, while seaweed and mushrooms were included. Items containing juice were excluded from the fruit group.
Table 1
Overview of MTDS components and the scoring scheme of the MTDS in this study
Psychosocial stress
To assess an individual’s psychosocial stress level, we utilized the PWI-SF, tailored for Korean conditions and proposed by Jang [25]. The PWI-SF facilitates a comparative study of stress and mental health across demographic characteristics. It aims to identify associations between risk factors associated with stress and disease and comprises 18 questions regarding physical and psychosocial conditions experienced or felt in recent weeks. Respondents rate the 18 items on a 4-point scale (0-1-2-3), and the cumulative score measures stress levels. The PWI-SF scores range from 0 to 54, with higher scores indicating elevated stress levels. A score of 27 or more categorizes an individual into the high-risk stress group, 9 to 26 into the potential stress group, and 8 or less into the healthy group.
Covariate
Demographic characteristics, socioeconomic status, and lifestyle factors of participants, including age, obesity level, daily energy intake, monthly household income, education level, smoking experience, and physical activity, were systematically assessed. Obesity levels, determined by the body mass index (BMI, kg/m2), were classified into 4 groups: underweight (< 18.5 kg/m2), normal weight (18.5 to < 23 kg/m2), overweight (23 to < 25 kg/m2), and obesity (25 kg/m2 or higher). Monthly household income was classified into 4 groups: < 1,000,000 won (Korean currency; 1 million Korean won = 765 USD), 1,000,000 to < 2,000,000 won, 2,000,000 to < 4,000,000 won, and 4,000,000 won or higher. Education levels were segmented into 4 groups: elementary school or less, middle school, high school, and college graduate or higher. Smoking status was categorized into 3 groups: never smoked, former smoker, and current smoker. Physical activity, assessed by the metabolic equivalent of tasks (METs) per day, was divided into three intensity levels: light, moderate, and vigorous.
Statistical analysis
Categorical and continuous data were summarized into frequencies, percentages, means, and standard deviations, respectively. The statistical differences between independent groups were analyzed using the χ2 test and one-way analysis of variance, followed by Duncan’s post-hoc test. The distribution of intakes of food groups and nutrients in the MTDS was described with the interquartile range (IQR). The MTDS was divided into tertiles, and food group and nutrient intakes for each quartile were described in the form of the IQR. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated by logistic regression to analyze the association between the MTDS (tertiles) and the prevalence of high-level psychosocial stress by gender. All data were processed, and statistical tests were analyzed using SAS 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Comparative analysis of general characteristics according to the tertiles of the MTDS
The analysis of the general characteristics of the subjects based on the MTDS tertiles is presented in Table 2. The ranges of the MTDS tertile groups for men were T1 (20–33 points), T2 (34–37 points), and T3 (38–39 points), while those for women were T1 (20–33 points), T2 (34–37 points), and T3 (38–48 points). The PWI-SF score was significantly lower at T3 compared to T1 and T2 in men (P = 0.014), and it was significantly lower at T2 and T3 compared to T1 in women (P = 0.027). There was no statistically significant difference in the general characteristics of subjects between the tertile groups for both men and women. However, women in the T3 group exhibited a higher educational level compared to the other groups (P = 0.001).
Table 2
General characteristics of study subjects according to the tertiles of the MTDS
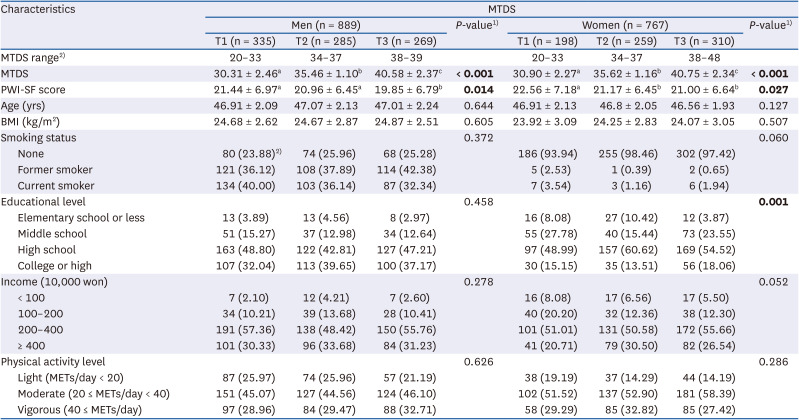
Values are presented as the mean ± SD or percentages. Bold styled values indicate statistical significance.
MTDS, Mediterranean-type diet score; PWI-SF, psychosocial well-being index-short form; BMI, body mass index; METs, metabolic equivalent of tasks.
a-cDifferent superscript letters are significantly different (P < 0.05 by Duncan post hoc test).
1)Differences between groups were tested using a one-way analysis of variance analysis for continuous variables and a χ2 test for categorical variables.
2)The values are presented as the maximum and minimum of MTDS.
Relationship between the intake of food groups and the MTDS tertiles
The intake of food groups according to the MTDS tertiles is presented in Table 3. The results of the energy-adjusted logistic regression analysis revealed that the consumption of whole grains, potatoes, fruits, vegetables, legumes, and fish increased with higher MTDS, while the consumption of red meat and dairy products decreased in both men and women (P for trend < 0.05). Additionally, poultry and alcohol consumption decreased as MTDS decreased in men (P for trend < 0.05), whereas P for the trend was not obtained, given the absence of a difference in the median value of intake between the tertile groups in women.
Table 3
Food group intake frequency (servings/week) for the tertiles of the MTDS
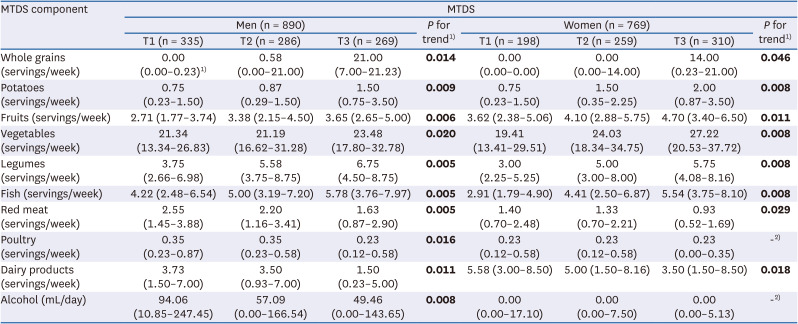
Values are presented as the interquartile range. Bold styled values indicate statistical significance.
MTDS, Mediterranean-type diet score.
1)P for the trend was obtained from logistic regression model analysis adjusted for energy intake (kcal/day) and age (yrs).
2)No values were obtained as there were no differences in the median value of food group intake between the tertile group.
Relationship between the nutrition intake and the tertiles of the MTDS
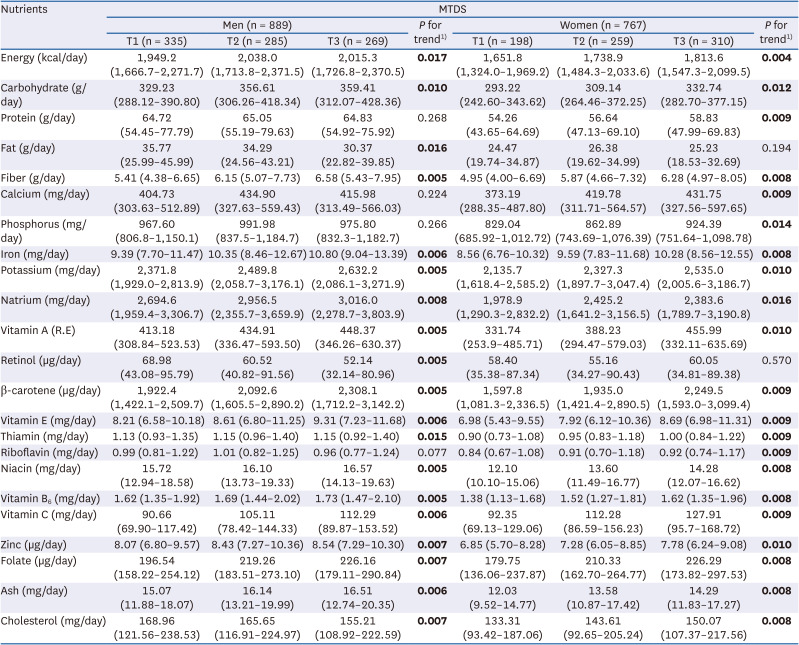
A summary of the energy and nutrient intakes including carbohydrates, proteins, fats, fiber, calcium, phosphorus, iron, potassium, natrium, vitamin A, retinol, β-carotene, vitamin E, thiamin, riboflavin, niacin, vitamin B6, vitamin C, zinc, folate, ash, and cholesterol according to the tertiles of the MTDS is presented in Table 4. As MTDS increased, energy and nutrient intakes excluding protein, calcium, phosphorus and riboflavin increased in men (P for trend < 0.05) and energy and nutrient intakes excluding fat and retinol increased in women (P for trend < 0.05).
Table 4
Nutrient intake IQR for the tertiles of the MTDS
Prevalence of high levels of psychosocial stress according to the MTDS tertiles
Table 5 presents the adjusted OR and 95% CIs for high psychosocial stress from the multiple logistic regression analyses by MTDS tertiles. A higher MTDS was significantly associated with a lower prevalence of high psychosocial stress and showed a declining trend (P for trend = 0.016 for men and 0.026 for women). Men in the highest MTDS tertile had a 41% lower OR of high psychosocial stress compared with those in the lowest tertile (OR, 0.59; 95% CI, 0.38–0.91). Similarly, women in the highest tertile of the MTDS had a 39% lower OR of high psychosocial stress compared with those in the lowest tertile (OR, 0.61; 95% CI, 0.40–0.95).
Table 5
The association between the tertiles of the MTDS and high level of psychosocial stress1)
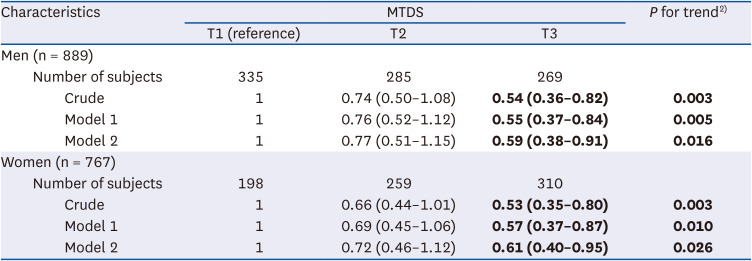
Values are presented as odds ratio (95% confidence interval). Bold styled values indicate statistical significance.
Model 1 was adjusted for age (yrs), and energy intake (kcal/day). Model 2 was adjusted for age (yrs), energy intake (kcal/day), education level (primary school or less, middle school, high school, and college graduate or higher), monthly household income (< 1,000,000 won (Korean currency; 1 million Korean won = 765 USD), 1,000,000 to < 2,000,000 won, 2,000,000 to < 4,000,000 won, and 4,000,000 won or higher), physical activity level (light, moderate, and vigorous activity), smoking status (never, former, and current smoker), obesity (underweight [< 18.5 kg/m2], normal [18.5 to < 23 kg/m2], overweight [23 to < 25 kg/m2], and obesity 25 kg/m2 or higher]).
PWI-SF, psychosocial well-being index-short form; MTDS, Mediterranean-type diet score.
1)High levels of psychosocial stress were defined as scores of 27 or higher on the PWI-SF questionnaire, while scores below that threshold were considered part of the reference group [25].
2)P for trend was obtained from logistic regression model analysis.
DISCUSSION
This study used data from the third stage (2005–2006) of the KoGES to analyze the association between adherence to the Mediterranean diet and psychosocial stress for those born between 1955 and 1963, the baby boomer generation. Results showed that higher adherence to the Mediterranean diet was associated with a lower prevalence of high levels of psychosocial stress.
Psychosocial stress plays an important role in physiological processes, contributing to adverse health outcomes. Chronic psychosocial stress has the potential to elevate the risk of mental health issues, such as depression [26], as well as aging, obesity, metabolic syndrome, type 2 diabetes, cardiovascular disease, stroke, Alzheimer’s disease, and cancer [27282930]. In earlier studies, Mohan et al. [28] suggested that the prevention and treatment of cancer should aim to reduce stress and stress-induced lifestyle behaviors while Sparrenberger et al. [29] suggested that chronic stress is a cause of sustained elevated blood pressure. In addition, psychosocial stress has been shown to have a significant impact on C-reactive protein, a strong marker of systemic inflammation associated with several disease conditions, including malignancy [30].
Evidence has consistently shown that diet can play an important role in brain health and can influence mental health and cognitive function [313233]. Inflammation is a risk factor for depression, psychosis, and other major mental illnesses [34]. Inflammation is typically triggered by stress, and different types of stressors, such as psychosocial stress or lifestyle factors, including physiological and physical inactivity and smoking, can lead to increased inflammatory activity [35]. Individuals with inflammatory dietary patterns are at a greater risk of developing depression over time [36]. Adopting a healthy dietary pattern, such as the Mediterranean diet, has been shown to reduce systemic inflammation [3738]. Oxidative stress, an imbalance of oxidative and antioxidant processes, can cause cellular damage to lipids, proteins, and DNA, and persistent oxidative stress has been implicated as a potential mechanistic pathway for depression and other mental health disorders [39]. The anti-inflammatory effects of the Mediterranean diet can reduce the levels of products associated with oxidative damage, increase total antioxidant capacity and antioxidant levels, normalize neurotransmitter production, and positively affect mood [40].
The Mediterranean diet is characterized by plant-based components, including fruits, vegetables, whole grains, and legumes, ensuring a substantial intake of fiber, potassium, flavonoids, and carotenoids. These bioactive compounds contribute to the positive effects on metabolic health and cognitive function provided by this diet [41]. Our study revealed a positive association between an enhanced adherence to the Mediterranean diet and the augmented consumption of plant-based foods and fish. Additionally, this heightened adherence resulted in an increased intake of fiber, vitamins, and minerals. Fiber, which is abundant in plant-based diets, has been shown to reduce inflammatory responses to lipopolysaccharides, which are pro-inflammatory bacterial components that can pass through the intestinal mucosa and trigger local and systemic inflammatory responses [42]. A diet rich in plant-derived foods may also increase the intake of minerals, vitamins, and polyphenols that play a role in antioxidant cellular defense for brain health [43]. In a systematic review, most studies found a positive effect of fruit and/or vegetable intake on mental health [44]. A prominent research discovery and hypothesis concerning the relationship of an individual's dietary and nutrient intake with depression involves the metabolism of homocysteine facilitated by the B vitamins [45]. The decreased intake of B vitamins may contribute to the mechanisms involved in the etiology of depression by causing homocysteine accumulation and decreased monoamine synthesis in the brain [46]. N-3 fatty acids have anti-inflammatory effects and inhibit the production of pro-inflammatory cytokines [47], making them one of the most studied nutrients in the field of depression, along with the B vitamins. Healthy fat characteristic of the Mediterranean diet, such as mono- and polyunsaturated fatty acids found in olive oil, fish, seeds, and nuts, have been shown to play an active role in brain cells. A cohort study of fish and n-3 fatty acids consumption and depression in Japan suggested that moderate fish consumption may be recommended for the prevention of major depressive disorders in older adults [48].
Our study has several limitations. This study is a cross-sectional study. Hence, it is difficult to determine a causal relationship between the Mediterranean diet and stress reduction. Dietary assessments may underestimate or overestimate the dietary intake due to recall and social desirability bias. The psychosocial stress was estimated using self-administered structured questionnaires. Therefore, measurement errors or misclassifications could contribute to some degree of residual confounding. Nevertheless, this study represents the first study of the association between the Mediterranean diet and stress in aging Korean baby boomers. The findings suggest that adherence to a Mediterranean diet may be beneficial in reducing stress.
In conclusion, promoting adherence to a Mediterranean diet among baby boomers could positively impact healthy aging, consequently benefiting the nation. Hence, future studies should explore effective dietary interventions to encourage adherence to the Mediterranean diet among baby boomers.
 XML Download
XML Download