

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hypertension is one of the main causes of chronic diseases that accompany complications such as stroke, heart failure, and angina [1]. The prevalence of hypertension has decreased from 26.0% in 1998 to 21.8% in 2021, however, the absolute number of hypertension patients has increased steadily according to the Korea Hypertension Fact Sheet 2023 [2]. Although genetic and lifestyle factors are cited as risk factors for hypertension [3], it is well known that excessive sodium intake increases the prevalence of hypertension [4]. Furthermore, sodium intake increases the risk of kidney disease and gastrointestinal disease [56]. Therefore, a low-sodium diet can help decrease the risk of chronic diseases such as hypertension.
Although a previous study showed that sodium intake in Korea decreased in 2017 compared with 2013, it was still above the recommended daily allowance for all age groups except for the group of 1–9 years old. In this regard, ‘noodles and dumplings’ and ‘ramyeon’ were found as the main dishes contributing to sodium intake in Korea [7]. A study on the relationship between noodle consumption and hypertension among middle-aged Korean women also showed that the greater the consumption of noodles, the higher the sodium intake [8].
Previous studies have reported that noodle consumption is associated with a high serum phosphorus level, which is associated with cardiovascular disease and a high triglyceride level accompanied with obesity [910]. A previous cohort study conducted in Korea also showed a proportional association between noodles and hypertension among women [8]. However, the previous study includes only 2 areas near the capital city and the number of participants is small. Therefore, this study aimed to investigate the association between noodle intake and hypertension among Korean adults aged 40–69 years in the Health Examinees (HEXA) study that was more up-to-date data and with a larger participant, and region size than previous studies.
SUBJECTS AND METHODS
Study population
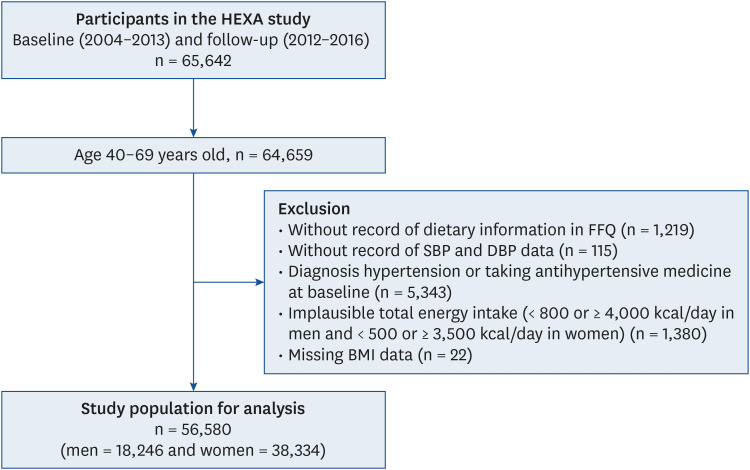
This study included participants from the HEXA study in the Korean Genome and Epidemiology Study Consortium, which is a large-scale genomic cohort study conducted by the Korea Disease Control and Prevention Agency. A total of 65,642 participants aged 40–69 were selected through physical and blood tests at 38 general hospitals and examination centers in 8 regions throughout Korea. The baseline survey was performed from 2004 to 2013 and the follow-up survey was carried out from 2012 to 2016. The design and selection criteria for hospital and examination centers and participants of the HEXA study have been described in the literature [1112]. Among 65,642 participants, those aged less than 40 or over 69 years (n = 983), with no food frequency questionnaire (FFQ) data (n = 1,219), with no systolic blood pressure (SBP) and diastolic blood pressure (DBP) data (n = 115), with hypertension (SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg) or taking hypertension medicine at baseline survey (n = 5,343), with inappropriate total energy intake (< 800 or ≥ 4,000 kcal/day for men and < 500 or ≥ 3,500 kcal/day for women) (n = 1,380), or with missing body mass index (BMI) data (n = 22) were excluded. A total of 56,580 participants (18,246 men and 38,334 women) remained in the final analysis (Fig. 1).
Fig. 1
The selection process for the study population in the HEXA study.
HEXA, Health Examinees; FFQ, food frequency questionnaire; SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index.
All participants voluntarily signed an informed written consent form before enrollment. This study was performed per the guidelines specified in the Declaration of Helsinki, and the study protocol was approved by the local Institutional Review Board (IRB) of the Ethics Committee of the Korean National Institute of Health and the IRBs of all the participating hospitals (IRB No. E–1503–103–657).
Dietary assessment
Dietary consumption was evaluated by the FFQ including 106 food items, which was used to analyze noodle consumption and nutrient intake among the participants. The FFQ presents the frequency of intake in 9 categories (none or rarely, once/month, 2–3 times/month, 1–2 times/week, 3–4 times/week, 5–6 times/week, once/day, twice/day, and thrice/day) and the serving size of intake in 3 categories (0.5, 1, and 1.5 servings). The size of 1 serving was decided by considering the most common serving sizes found in the food 24-hour recall data and reference serving sizes of Dietary Reference Intakes for Koreans and the Korean Nutrition Society. For more precise estimating serving sizes, booklets containing pictures of 1 serving size for all food items were prepared [13]. The validity and reproducibility of this FFQ have been proven in a previous study [14]. Noodles included ramyeon, chopped noodles/jangguk noodles/udon, black bean sauce noodles/jjamppong noodles (spicy noodles), and cold noodles/buckwheat noodles. A gram of 1 serving size is 120 g for ramyeon, 300 g for chopped noodles/jangguk noodles/udon, 430 g for black bean sauce noodles/jjamppong noodles, and 110 g for cold noodles/buckwheat noodles. Total noodle consumption was the sum of the average serving size of each noodle consumption per day between baseline and follow-up surveys. Participants were divided into quintiles according to total noodle consumption. Total energy intake (kcal/day) and macronutrient intake (g/day) including carbohydrates, protein, fat, sodium (Na, mg/day), and potassium (K, mg/day) were calculated using a food composition table specified by the Korean Health and Industry of Development Institute [15]. The percentage of inadequate intake of sodium and adequate intake of potassium was calculated using the reference intake of 2020 Dietary Reference Intakes for Koreans [16]. The inadequate intake of sodium was defined as daily sodium intake was defined as the proportion of participants whose daily sodium intake is more than 2,300 mg for 40–64 years old and 2,100 mg for 65–69 years old. The appropriate potassium intake ratio refers to the proportion of participants with a daily potassium intake of more than 3,500 mg.
Assessment of hypertension
Blood pressure, such as SBP and DBP were recorded twice using mercury sphygmomanometers, and the average of the measurements was used for analysis. This study followed the definition of hypertension from The Korean Society of Hypertension (SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg). In addition, participants with taking hypertension medications or were diagnosed with hypertension [17].
Covariates
Sociodemographic factors that can affect hypertension include age, gender, education level, income level, marital status, BMI, and lifestyle factors such as alcohol consumption, smoking status, and physical activity. The participants were divided into 3 age groups: "40 ≤ age ≤ 49", "50 ≤ age ≤ 59", and "60 ≤ age ≤ 69". Income level was categorized as "income < 3 million won" and "income ≥ 3 million won". Education level was classified as "under middle school", "high school", and "beyond college". Marital status was divided into 2 groups: "married" and "other". Alcohol consumption was categorized as "current drinker" (still drinks alcohol) and "non-drinker" (never drank alcohol or abstained for more than 2 months). Smoking status was classified into 3 categories: "never smoker" (never smoked cigarettes), "past smoker" (smoked more than 400 cigarettes in the past but not did not smoke at the time of the survey), and "current smoker" (smoked cigarettes at the time of the survey and smoked more than 400 cigarettes). Physical activity was divided into 2 categories: "active" (exercised for ≥ 30 min once a day for ≥ 3 days a week) and "inactive". BMI was measured by dividing the weight by the square of the height (kg/m2). BMI values were categorized as "normal" (BMI < 25 kg/m2) and "obese" (BMI ≥ 25 kg/m2) [18].
Statistical analysis
All statistical analyses were conducted according to gender to determine the association of noodle consumption with hypertension. Continuous variables are presented as means and SD, and categorical variables are presented as numbers and percentages. Differences in baseline characteristics across the quintiles of noodle consumption were analyzed by analysis of the chi-square test for categorical variables and the general linear regression model for continuous variables. To analyze the association of noodle consumption with hypertension, Cox proportional hazard models were used to calculate the hazard ratio (HR) and 95% confidence interval (CI) of hypertension based on the quintiles of noodle consumption, with the lowest quintile as the reference. In model 1, age and BMI were adjusted. The covariates in model 1 and income level (< 3 million won, ≥ 3 million won), education level (under middle school, high school, or beyond college), marital status (married or others; single, separated), smoking status (never, past, or current smoker), alcohol consumption (non-drinker or current drinker), physical activity (active or inactive), energy intake (continuous), carbohydrate intake (continuous), and sodium intake (continuous) were adjusted in model 2. The covariates included in model 2 and hypertension-related diseases such as hyperlipidemia, diabetes, stroke, transient ischemic attack, and angina were adjusted in model 3. This study was performed with SAS version 9.4 (SAS Institute, Cary, NC, USA), and P < 0.05 was considered statistically significant.
RESULTS
General characteristics according to noodle consumption
The general characteristics of the subjects according to the quintiles of noodle consumption are presented in Table 1. Among men, higher income and alcohol consumption were associated with higher noodle consumption. Regardless of gender, younger age, obese, and inactive groups were associated with higher noodle consumption (P < 0.05). Compared with the lowest noodle consumption group, BMI was high for both men and women according to increased noodle consumption. The marital status of men showed others and women showed married according to noodle consumption. Among men and women, high school completion was significantly associated with the highest noodle consumption group.
Table 1
General characteristics of the study population at baseline examination according to the quintiles of noodle consumption and gender in the Health Examinees study
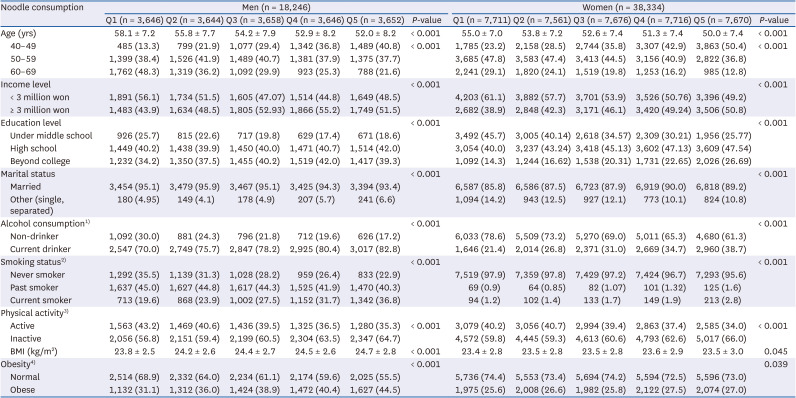
Values are presented as mean ± SD or number (%).
P-values were calculated by χ2 test for categorical variables and general linear regression for continuous variables.
BMI, body mass index
1)Non-drinker, never drank alcohol or abstained for > 2 mon; current drinker, still drinks alcohol.
2)Never smoker, never smoked cigarettes; past smoker, smoked > 400 cigarettes in the past but did not smoke at the time of the survey; current smoker, smoked cigarettes at the time of the survey or smoked > 400 cigarettes.
3)Active, exercised for ≥ 30 min once a day for ≥ 3 days a week: Inactive, participants not in the active group.
4)Obesity, normal: BMI < 25 kg/m2; obese: BMI ≥ 25 kg/m2.
Nutrient and food intake according to noodle consumption
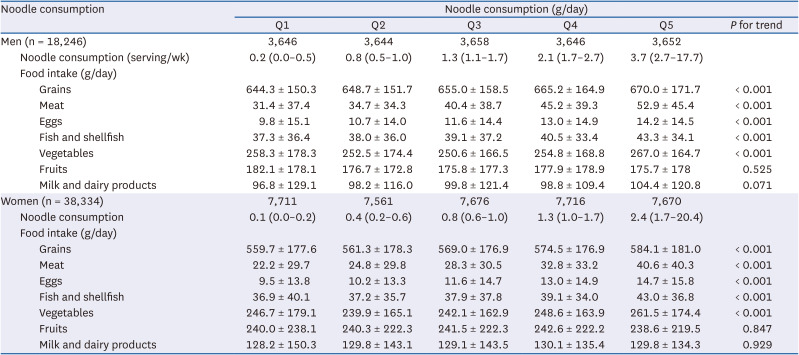
The daily intake of nutrients according to the quintiles of noodle consumption is presented in Table 2. In comparison with participants who consumed lower noodles, those who consumed more noodles had higher intakes of total energy, carbohydrates, protein, and fat. Participants with increased noodle consumption had lower intakes of sodium, potassium, and the percentage of inadequate intake of sodium and adequate intake of potassium. However, the ratio of sodium/potassium was significantly increased with increasing quintiles of noodle consumption. All P-values were < 0.001. The daily intake of different groups of food according to the quintiles of noodle consumption is presented in Table 3. Regardless of gender, the intake of grains, meat, eggs, fish and shellfish, and vegetables was significantly higher with increasing quintiles of noodle consumption (P < 0.001). There is no significant difference between noodle consumption with fruits and Milk and dairy products consumption.
Table 2
Macronutrient intake and energy (percent) according to the quintiles of noodle consumption and gender in the Health Examinees study
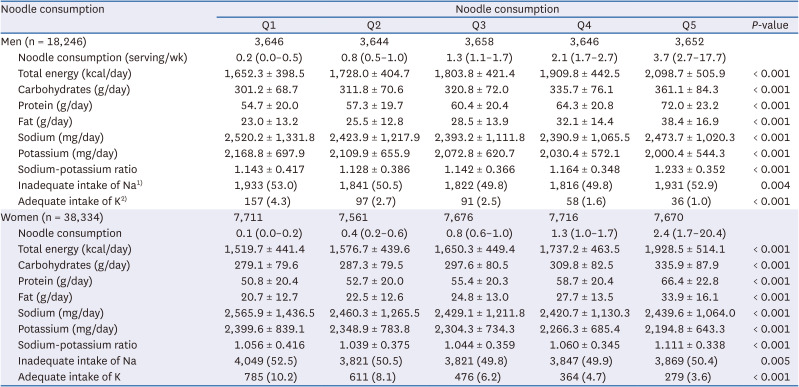
Values are presented as the median (interquartile range) or mean ± SD or number (%).
P-values were calculated by general linear regression for continuous variables.
1)The proportion of inadequate Na intake refers to the proportion of participants whose daily sodium intake is more than 2,300 mg for 40–64 years old and 2,100 mg for 65–69 years old.
2)The appropriate K intake ratio refers to the proportion of participants with a daily potassium intake of more than 3,500 mg.
Table 3
Daily intake of different groups of food according to the quintiles of noodle consumption and gender in the Health Examinees study
Association of noodle consumption with hypertension
During 279,184.8 person-years of follow-up (mean: 4.9 years, SD: 1.8), 14,299 hypertension events were identified. The multivariate-adjusted HR and 95% CI for the prevalence of hypertension according to noodle consumption quintiles and gender are shown in Table 4. Higher noodle consumption was associated with increased hypertension among men (HR, 1.273; 95% CI, 1.166–1.390; P for trend < 0.0001) and women (HR, 1.116; 95% CI, 1.038–1.199; P for trend = <0.001) after adjusting for potentially confounding variables such as sociodemographic and lifestyle factors (age, BMI, income level, education level, marital status, smoking status, alcohol consumption, and physical activity), energy intake, sodium intake, and hypertension-related diseases (hyperlipidemia, diabetes, stroke, transient ischemic attack, and angina). The HRs for the types of noodles are shown in Supplementary Tables 1 and 2. A higher intake of all types of noodles (ramyeon, chopped noodles/jangguk noodles/udon, black bean sauce noodles/jjamppong noodles, and cold noodles/buckwheat noodles) increased the incidence of hypertension in men compared with a lower intake group of each type of noodles, and women were associated with a higher intake of ramyeon and chopeed noodles/jangguk noodles/udon.
Table 4
HR of hypertension according to the quintiles of noodle consumption and gender in the Health Examinees study
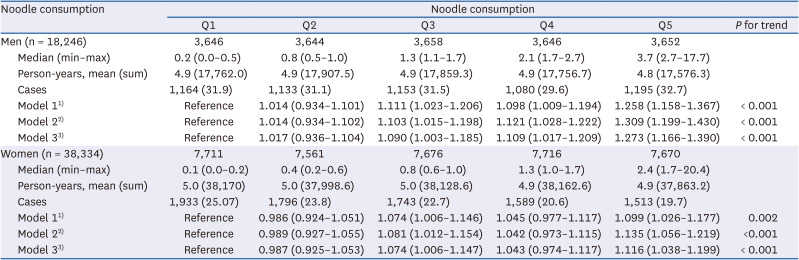
Values are presented as the HR (95% confidence interval) or number (%).
HR, hazard ratio.
1)Model 1: age (continuous) and body mass index (continuous).
2)Model 2: including covariates in model 1 and income level (< 3 million won, ≥ 3 million won), education level (under middle school, high school, or beyond college), marital status (married or others), smoking status (never, past, or current smoker), alcohol consumption (non-drinker or current drinker), physical activity (active or inactive), energy intake (continuous), carbohydrate intake (continuous), and sodium intake (continuous).
3)Model 3: including covariates in model 2 and hypertension-related diseases (hyperlipidemia, diabetes, stroke, transient ischemic attack, and angina.
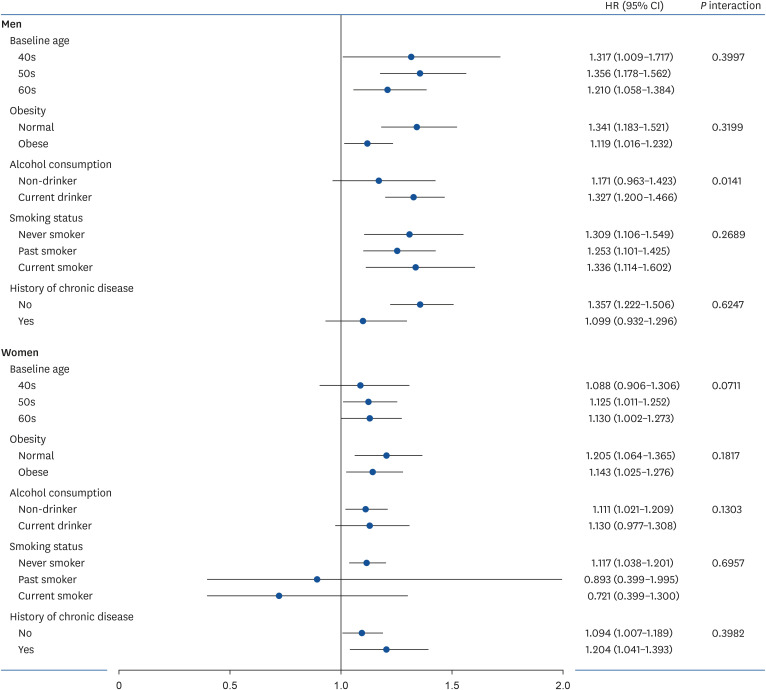
Association of noodle consumption with hypertension as stratified covariates
The HRs of hypertension in a comparison of the extreme quintiles of noodle consumption according to gender stratified by baseline age, obesity, alcohol consumption, smoking status, and chronic disease are shown in Fig. 2. There is no significant interaction between the subgroups of stratified covariates except alcohol consumption in men. Among men, those who were current drinkers (HR, 1.171; 95% CI, 0.963–1.423) were significantly relative with the high risk of hypertension compared with those who were non-drinkers (HR, 1.327; 95% CI, 1.200–1.466; P interaction = 0.014).
DISCUSSION
This study analyzed the association of noodle consumption with hypertension using participants from the HEXA study in Korea from 2004 to 2013. In this study, participants with higher noodle consumption generally had increased hypertension, as demonstrated by the HR. The results of our study are consistent with the findings of a previous study on noodle consumption conducted in Korea [8]. The previous study showed that frequent noodle consumers (≥ 5 servings/week) among Korean women had a 2.3-fold higher risk of hypertension compared with the risk of those who never consumed noodles (HR, 2.31; 95% CI, 1.33–4.01; P for trend = <0.001). There was no significant association between the risk of hypertension and noodle consumption among men [8]. However, in our study, among men, there was also associated with a higher risk of hypertension according to a higher noodle consumption. The previous study only showed significant results for middle-aged women, and there were only around 5,000 individuals [8]. In contrast, our study was conducted on a larger scale than the previous analysis.
In our study, male drinkers consuming higher noodles had a higher risk of hypertension as compared with non-drinkers. This result may be associated with our analysis that drinkers are more likely to consume more noodles. In women, there was no significant difference in HR values between non-drinkers and drinkers, but non-drinkers had a significantly higher risk of hypertension with noodle intake. This may be associated with a lower frequency of drinking in women than in men. Therefore, regardless of drinking, our results may imply that consumption of noodles may be associated with hypertension.
Several studies may explain the association between noodle intake and the risk of abnormal cardiovascular events [19]. A positive association was observed between the frequency of instant noodle consumption and plasma triglyceride levels, DBP, and fasting blood glucose levels among Korean college students [19]. Furthermore, through the Korea National Health and Nutrition Examination Survey (KNHANES) cross-sectional survey of Koreans, it was found that the intake of instant ramyeon (22 times/week) was associated with a high prevalence of metabolic syndrome and slightly higher abdominal obesity among women [20].
Prior studies have demonstrated the role of sodium in the association between the intake of noodles and the risk of hypertension [8]. According to the KNHANES 2013–2017 in Korea, noodles and dumplings are the top sources of sodium intake (536.7 mg/day), and consumers obtained large amounts of sodium from instant ramyeon (190.5 mg/day), jangguk noddles (104.2 mg/day), and black bean sauce noodles (67.6 mg/day) [7]. The results of previous studies revealed that instant noodles made in Korea contain large amounts of sodium in one serving (600–2,770 mg) [21]. The consumption of excessive sodium is known to increase blood pressure as sodium ions accumulate in the body, increasing the amount of extracellular fluid volume, vascular and cardiac function, and the excitability and resistance of the arterial wall [22]. In the results of a previous review, an increased intake of salt was clearly related to an increase in blood flow and blood pressure [2223]. Therefore, noodle consumption could affect the risk of developing hypertension in that it is accompanied by sodium intake.
However, in this study, sodium intake didn’t increase significantly according to the increase in noodle consumption, if anything, it showed a decreasing trend. In addition, in our study, after adjusting carbohydrate and sodium intake, the risk of hypertension was significant. This might be related to the group with higher noodle intake in this study results showing a lower potassium intake, lower fruit intake, and higher sodium-potassium ratio. In previous studies reported that the sodium-potassium ratio was associated with high blood pressure [242526]. Differences in hypertension prevalence between several groups are generally attributed to differences in the amount of dietary sodium but may also reflect differences in potassium intake. The guidelines of the World Health Organization recommend a Na/K ratio of approximately < 1.0 for preventing cardiovascular health benefits [24]. A study conducted in Japan analyzed the association between urinary Na/K ratio and blood pressure, the increased urinary Na/K ratio was linearly associated with hypertension [2425]. In addition, the dietary Na/K ratio is associated with the risk of blood pressure, and this study suggested that urine-induced sodium excretion helps reduce blood pressure [26].
It has been shown in previous meta-analysis that increasing potassium intake could lower the blood pressure and protect against cardiovascular disease. Moreover, compared with the effect of sodium or potassium alone in hypertension, the sodium-potassium ratio has been more strongly associated with blood pressure [27]. An appropriate sodium-potassium ratio is important not only for maintaining homeostasis in the body but also for the prevention of various vascular diseases.
The current study has several limitations. First, dietary intake may vary during the period between baseline and follow-up. In addition, in this study, the noodle recipe was not considered. The results could not be generalized globally as the study surveyed only domestic participants of a certain age group (40–69 years). Therefore, to investigate the age difference is needed to study the association between the consumption of noodles by young adults, adolescents, or other age groups and hypertension. Finally, hypertension was diagnosed based on the measured blood pressure and hypertension treatment history.
Despite these limitations, the current study has several strengths. First, compared with similar previous studies, the study evaluated a larger number of Korean adults aged 40–69 years using the HEXA data. Moreover, as research on the correlation between noodle intake and hypertension is insufficient, further studies on the cause of hypertension in adults are necessary.
Using large-scale HEXA data for both men and women aged 40–69 years, the higher noodle intake was associated with an increased risk of hypertension. The results of our study may provide evidence that reducing noodle intake may be important for the prevention of hypertension in dietary habits. For the management of hypertension, it is recommended to reduce the intake of noodles and sodium and consume more vegetables and fruits to increase the intake of potassium. In addition, this study showed a positive association between noodle consumption and the incidence of hypertension, but further investigations and verification from large-scale cohort studies in other countries might be necessary to validate these results.
 XML Download
XML Download