

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiometabolic health outcomes encompass the overall state of health and well-being related to the cardiovascular system and metabolic processes in the body. They range from conditions such as blood pressure (BP), blood lipids (cholesterol and triglycerides [TG]), and blood glucose to cardiometabolic diseases (CMDs) like metabolic syndrome (MetS), type 2 diabetes (T2D), and more severe diseases including cardiovascular disease (CVD) and stroke [1]. And CMDs have long been recognized as primarily attributed to an unhealthy lifestyle characterized by smoking, physical inactivity, and unhealthy diet [2]. Health-promoting lifestyle behaviours play a crucial role in both prevention and control of CMDs. Thus, lifestyle modification may be the most effective way to reduce the burden of CMDs [3].
A healthy diet, incorporating fruits, vegetables, and low-fat foods, has been extensively studied on the association with risk of CMDs [4]. Nevertheless, further evidence to discover novel dietary factors for the prevention of CMDs are still needed. Among dietary factors, mushrooms have been utilized as a medicinal product over 2 millennia, with evidence suggesting their potentials to exert favorable effects on health conditions, including oxidative stress [4], inflammation [5], immunity [6], and atherogenic lipid profile [7]. The potentials of mushrooms have highlighted the presence of various nutrients and bioactive compounds. Edible mushrooms are notably rich sources of vitamins such as thiamine, riboflavin, vitamin B12, biotin, folate, vitamin C, and vitamin D, as well as essential minerals encompassing iron (Fe), magnesium (Mg), phosphorus (P), potassium (K), zinc (Zn), and selenium (Se) [89]. Furthermore, their bioactive components such as beta-glucan, ergosterol, ergothioneine, and polysaccharides may contribute to the potential health benefit of mushrooms [91011].
Although there is limited evidence from epidemiological studies examining the relationship between dietary mushroom consumption and cardiometabolic health outcomes, 2 systematic reviews were identified [1213]: The first one was on the CMDs such as coronary heart disease (CHD), stroke, T2D, and hypertension (HTN) but encompassed only seven articles, [12]; The second one investigated a wide range of cardiometabolic health outcomes [13] such as BPs, blood lipids (total cholesterol [TC], high-density lipoprotein cholesterol [HDL-C], low-density lipoprotein cholesterol (LDL-C), and TG, etc.), and fasting blood glucose (FBG). However, these systematic reviews were some limitations to conclude mushrooms and CMDs, particularly for the general population [13]: 1) both systematic reviews included studies among only patients with a specific disease, such as CHD and T2D [1213]; 2) the second systematic review included dietary pattern with a high factor loading value for mushroom consumption [13]; and 3) additionally, some effect sizes were extracted from studies that did not focus on mushrooms as the main exposure, without considering potential confounders [13].
Therefore, this systematic review aimed to explore the link between mushrooms and cardiometabolic health outcomes by analysing data from prospective cohort studies and clinical trials that targeted the general population, with a primary focus on mushrooms as a major exposure rather than a component of dietary pattern.
SUBJECTS AND METHODS
Data search sources and strategy
This systematic review followed the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines provided by The PRISMA Group [14]. Relevant original articles published until July 2023 were screened by a comprehensive search strategy, using PubMed (https://www.ncbi.nlm.nih.gov/pubmed/) and Ovid-Embase (http://ovidsp.tx.ovid.com). Grey literature recently published was identified through Google Scholar. The specific searching index terms were shown in Supplementary Tables 1 and 2. The search filters provided by Cochrane handbook were used as a term for study design.
Inclusion and exclusion criteria
We included cohort, randomized controlled trial (RCT), and clinical studies of mushroom intake and cardiometabolic health outcomes in the populations who are ≥ 18 years old. Exclusion criteria were as follows: studies among participants who were pregnant woman or composed of only patients with a specific disease such as T2D, dyslipidemia, HTN, chronic obstructive pulmonary disease, or ulcerative colitis and Crohn’s disease; studies analyzing with specific diet or pattern, not with mushroom itself; studies intervening with extracted components of mushroom; studies not reporting predefined outcome; case series or case report, pilot studies, or animal studies. All selected literatures were original, full-length, and published in English.
Data extraction and study quality
We extracted the following data from each study: title; authors; country; year of publication; study design; population; follow up or duration years; basic information of the subjects (race, sample sizes, age range, sex distribution, description, and dietary assessment); intervention (exposed) and control (comparison) regimes (number of participants, sex distribution, age range, intake form of mushroom, intake amount); outcome results.
To evaluate various study designs with one tool, the Joanna Briggs Institute (JBI) critical appraisal was used (https://jbi.global/critical-appraisal-tools). A critical assessment (the trustworthiness: yes/no/unclear) was undertaken individually by two investigators with the given manual. Any disagreement was resolved by consensus with a third investigator. Article that received a ‘Yes’ score of less than 70% was excluded from the overall evaluation due to low quality.
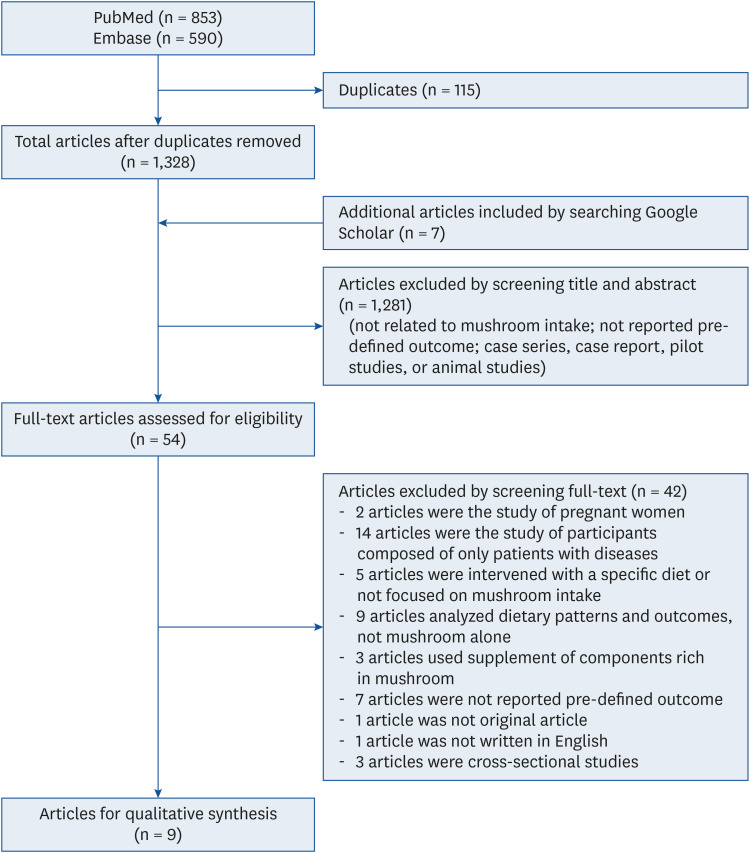
Two independent reviewers also conducted the screening process, first by reviewing the titles and abstracts, and then by reviewing the full-text articles (Fig. 1). If they could not reach a consensus about the eligibility of an article, it was resolved by a third investigator together.
Data synthesis
The results could not be quantitatively synthesized (i.e., meta-analyzed) due to the small number of articles. Instead of conducting a meta-analysis, we synthesized the results qualitatively and summarized the characteristics of the included studies (e.g., study population, design, intervention, results, and conclusion). The hazard ratios (HRs) and odds ratios (ORs) were extracted as outcome results of observational studies and the changes (%) and differences in cardiometabolic health outcomes during the intervention were presented for the experimental studies.
RESULTS
Literature search results
A total of 1,328 articles (853 from PubMed and 590 from Embase with 115 duplicate records) that met the inclusion criteria were initially identified. Additional 7 articles were identified through hand-searching in google scholar (Fig. 1). After screening the titles and abstracts, 54 articles remained for full text evaluation and by reviewing full articles for the eligibility, a total 9 articles [151617181920212223] were included in the systematic review (Tables 1 and 2).
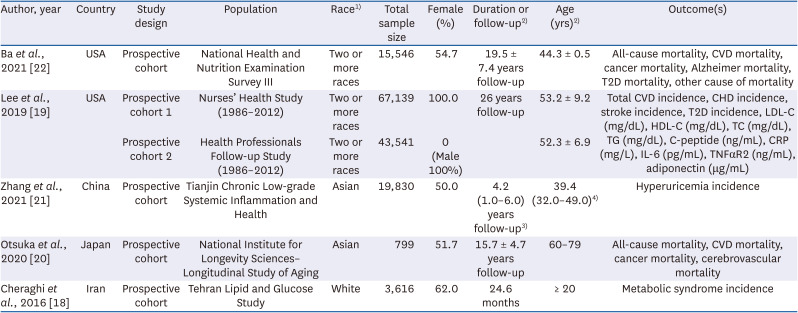
Table 1
Characteristics of observational studies included in the systematic review of mushroom consumption and cardiometabolic health outcomes
| Author, year | Country | Study design | Population | Race1) | Total sample size | Female (%) | Duration or follow-up2) | Age (yrs)2) | Outcome(s) |
|---|---|---|---|---|---|---|---|---|---|
| Ba et al., 2021 [22] | USA | Prospective cohort | National Health and Nutrition Examination Survey III | Two or more races | 15,546 | 54.7 | 19.5 ± 7.4 years follow-up | 44.3 ± 0.5 | All-cause mortality, CVD mortality, cancer mortality, Alzheimer mortality, T2D mortality, other cause of mortality |
| Lee et al., 2019 [19] | USA | Prospective cohort 1 | Nurses’ Health Study (1986–2012) | Two or more races | 67,139 | 100.0 | 26 years follow-up | 53.2 ± 9.2 | Total CVD incidence, CHD incidence, stroke incidence, T2D incidence, LDL-C (mg/dL), HDL-C (mg/dL), TC (mg/dL), TG (mg/dL), C-peptide (ng/mL), CRP (mg/L), IL-6 (pg/mL), TNFαR2 (ng/mL), adiponectin (μg/mL) |
| Prospective cohort 2 | Health Professionals Follow-up Study (1986–2012) | Two or more races | 43,541 | 0 (Male 100%) | 52.3 ± 6.9 | ||||
| Zhang et al., 2021 [21] | China | Prospective cohort | Tianjin Chronic Low-grade Systemic Inflammation and Health | Asian | 19,830 | 50.0 | 4.2 (1.0–6.0) years follow-up3) | 39.4 (32.0–49.0)4) | Hyperuricemia incidence |
| Otsuka et al., 2020 [20] | Japan | Prospective cohort | National Institute for Longevity Sciences–Longitudinal Study of Aging | Asian | 799 | 51.7 | 15.7 ± 4.7 years follow-up | 60–79 | All-cause mortality, CVD mortality, cancer mortality, cerebrovascular mortality |
| Cheraghi et al., 2016 [18] | Iran | Prospective cohort | Tehran Lipid and Glucose Study | White | 3,616 | 62.0 | 24.6 months | ≥ 20 | Metabolic syndrome incidence |
BMI, body mass index; C-peptide, connecting peptide; CHD, coronary heart disease; CRP, C-reactive protein; CVD, cardiovascular disease; DBP, diastolic blood pressure; FBG, fasting blood glucose; HDL-C, high-density lipoprotein cholesterol; IL-6, interleukin-6; LDL-C, low-density lipoprotein cholesterol; NA, not available; NAFLD, non-alcoholic fatty liver disease; NR, not reported or not evaluated; SBP, systolic blood pressure; T2D, type 2 diabetes mellitus; TC, total cholesterol; TG, triglyceride; TNFαR2, tumor necrosis factor-α receptor type 2; WC, waist circumference.
1)Among 6 categories (White, Black or African American, American Indian or Alaska Native, Asian, Native Hawaiian and Other Pacific Islander, Two or more races).
2)Data presented as mean ± SD or range.
3)Data presented as median (range).
4)Data presented as median (interquartile range).
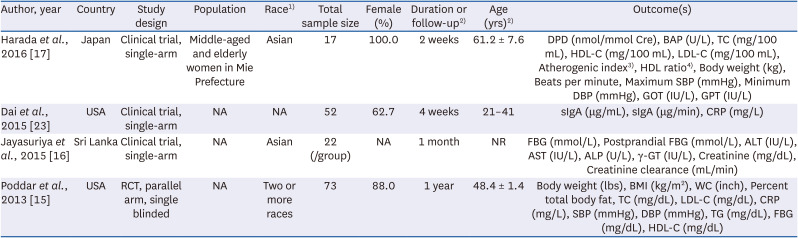
Table 2
Characteristics of experimental studies included in the systematic review of mushroom consumption and cardiometabolic health outcomes
| Author, year | Country | Study design | Population | Race1) | Total sample size | Female (%) | Duration or follow-up2) | Age (yrs)2) | Outcome(s) |
|---|---|---|---|---|---|---|---|---|---|
| Harada et al., 2016 [17] | Japan | Clinical trial, single-arm | Middle-aged and elderly women in Mie Prefecture | Asian | 17 | 100.0 | 2 weeks | 61.2 ± 7.6 | DPD (nmol/mmol Cre), BAP (U/L), TC (mg/100 mL), HDL-C (mg/100 mL), LDL-C (mg/100 mL), Atherogenic index3), HDL ratio4), Body weight (kg), Beats per minute, Maximum SBP (mmHg), Minimum DBP (mmHg), GOT (IU/L), GPT (IU/L) |
| Dai et al., 2015 [23] | USA | Clinical trial, single-arm | NA | NA | 52 | 62.7 | 4 weeks | 21–41 | sIgA (μg/mL), sIgA (μg/min), CRP (mg/L) |
| Jayasuriya et al., 2015 [16] | Sri Lanka | Clinical trial, single-arm | NA | Asian | 22 (/group) | NA | 1 month | NR | FBG (mmol/L), Postprandial FBG (mmol/L), ALT (IU/L), AST (IU/L), ALP (U/L), γ-GT (IU/L), Creatinine (mg/dL), Creatinine clearance (mL/min) |
| Poddar et al., 2013 [15] | USA | RCT, parallel arm, single blinded | NA | Two or more races | 73 | 88.0 | 1 year | 48.4 ± 1.4 | Body weight (lbs), BMI (kg/m2), WC (inch), Percent total body fat, TC (mg/dL), LDL-C (mg/dL), CRP (mg/L), SBP (mmHg), DBP (mmHg), TG (mg/dL), FBG (mg/dL), HDL-C (mg/dL) |
ALP, alkaline phosphatase; ALT, alanine amino transferase; AST, aspartate amino transferase; BAP, bone-specific alkaline phosphatase; BMI, body mass index; CRP, C-reactive protein; DBP, diastolic blood pressure; DPD, deoxypyridinoline; FBG, fasting blood glucose; γ-GT, gamma glutamyltransferase; GOT, glutamate oxaloacetate transaminase; GPT, glutamate pyruvate transaminase; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; NA, not available; NR, not reported or not evaluated; TC, total cholesterol; SBP, systolic blood pressure; sIgA, secretory immunoglobulin A; TG, triglyceride; WC, waist circumference.
1)Among 6 categories (White, Black or African American, American Indian or Alaska Native, Asian, Native Hawaiian and Other Pacific Islander, Two or more races).
2)Data presented as mean ± SD or range.
3)Atherogenic Index = (TC − HDL-C)/HDL-C.
4)HDL Ratio = HDL-C/TC × 100.
General characteristics of selected articles
There were 5 prospective cohort studies [1819202122] (Table 1) and 4 experimental studies (3 clinical trials [161723] and 1 RCT [15]) (Table 2). Countries of prospective cohort studies included the United States of America (USA), China, Japan, and Iran. Studies involved at least almost 800 participants, ranging from 799 to 67,139. The mean or median follow-up period of the prospective cohort studies varied 24.6 months to 26 years.
As for experimental studies, there were two studies in the USA, one Japanese study, and one Sri Lanka study. The sample sizes ranged from 17 to 73 with healthy participants. The length of intervention ranged from two weeks to one year, and there was variation in the types of edible mushrooms administered across studies. In terms of the form of mushroom, three studies provided dried mushroom [161723] and only one study provided fresh form [15].
Quality assessment
In Supplementary Tables 3, 4, 5, the results of the quality assessment of articles were presented. All 5 observational and 4 experimental articles were qualitatively acceptable.
Effects of mushroom consumption on cardiometabolic health outcomes
CMD mortality and morbidities
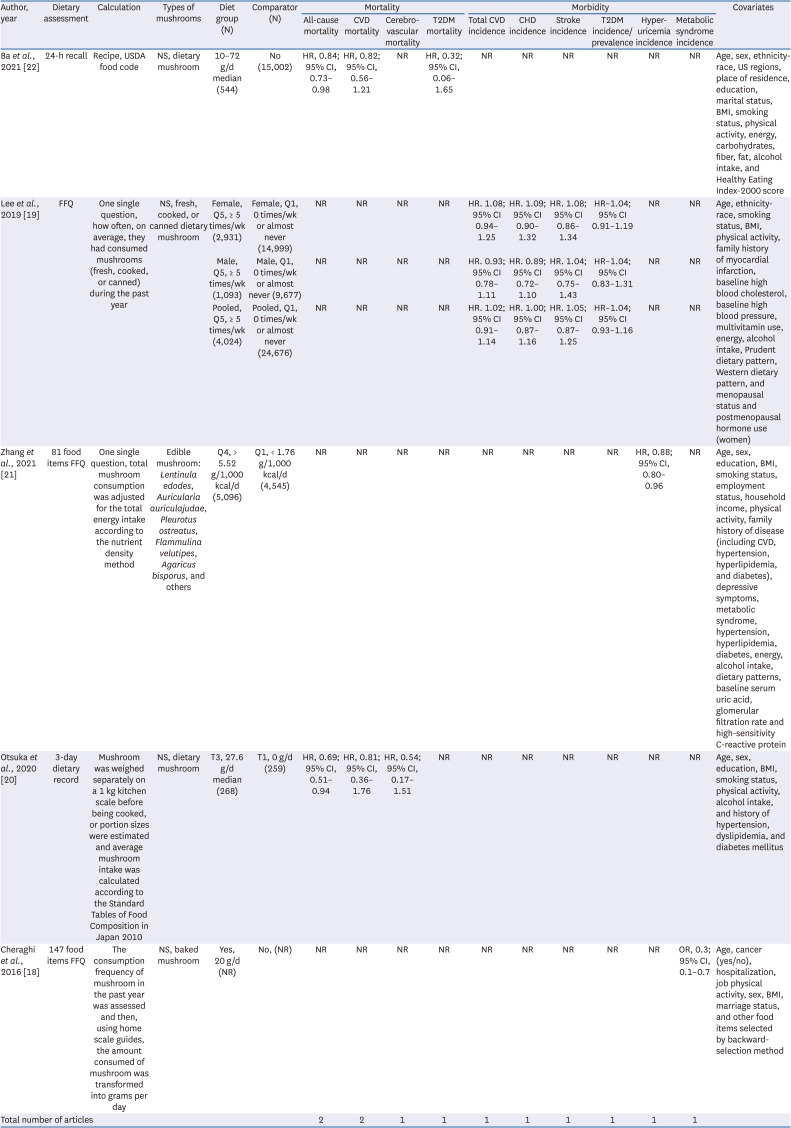
The qualitative review of mortality and morbidity across various health outcomes is presented in Table 3. Although not included in the initial search term, an inverse association between mushroom consumption and all-cause mortality was revealed (in the group consuming mushroom vs. the group not eating: HR, 0.84; 95% CI, 0.73–0.98 [22], and HR, 0.69; 95% CI, 0.51–0.94 [20]). On the other hand, there was no association in the mortality of T2D [20], CVDs [20], and cerebrovascular diseases [22].
Table 3
Quantitative summary of observational studies evaluating cardiometabolic disease mortality and morbidities consuming higher vs. lower amounts of mushrooms
| Author, year | Dietary assessment | Calculation | Types of mushrooms | Diet group (N) | Comparator (N) | Mortality | Morbidity | Covariates | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All-cause mortality | CVD mortality | Cerebrovascular mortality | T2DM mortality | Total CVD incidence | CHD incidence | Stroke incidence | T2DM incidence/prevalence | Hyperuricemia incidence | Metabolic syndrome incidence | |||||||
| Ba et al., 2021 [22] | 24-h recall | Recipe, USDA food code | NS, dietary mushroom | 10–72 g/d median (544) | No (15,002) | HR, 0.84; 95% CI, 0.73–0.98 | HR, 0.82; 95% CI, 0.56–1.21 | NR | HR, 0.32; 95% CI, 0.06–1.65 | NR | NR | NR | NR | NR | NR | Age, sex, ethnicity-race, US regions, place of residence, education, marital status, BMI, smoking status, physical activity, energy, carbohydrates, fiber, fat, alcohol intake, and Healthy Eating Index-2000 score |
| Lee et al., 2019 [19] | FFQ | One single question, how often, on average, they had consumed mushrooms (fresh, cooked, or canned) during the past year | NS, fresh, cooked, or canned dietary mushroom | Female, Q5, ≥ 5 times/wk (2,931) | Female, Q1, 0 times/wk or almost never (14,999) | NR | NR | NR | NR | HR. 1.08; 95% CI 0.94–1.25 | HR. 1.09; 95% CI 0.90–1.32 | HR. 1.08; 95% CI 0.86–1.34 | HR–1.04; 95% CI 0.91–1.19 | NR | NR | Age, ethnicity-race, smoking status, BMI, physical activity, family history of myocardial infarction, baseline high blood cholesterol, baseline high blood pressure, multivitamin use, energy, alcohol intake, Prudent dietary pattern, Western dietary pattern, and menopausal status and postmenopausal hormone use (women) |
| Male, Q5, ≥ 5 times/wk (1,093) | Male, Q1, 0 times/wk or almost never (9,677) | NR | NR | NR | NR | HR. 0.93; 95% CI 0.78–1.11 | HR. 0.89; 95% CI 0.72–1.10 | HR. 1.04; 95% CI 0.75–1.43 | HR–1.04; 95% CI 0.83–1.31 | NR | NR | |||||
| Pooled, Q5, ≥ 5 times/wk (4,024) | Pooled, Q1, 0 times/wk or almost never (24,676) | NR | NR | NR | NR | HR. 1.02; 95% CI 0.91–1.14 | HR. 1.00; 95% CI 0.87–1.16 | HR. 1.05; 95% CI 0.87–1.25 | HR–1.04; 95% CI 0.93–1.16 | NR | NR | |||||
| Zhang et al., 2021 [21] | 81 food items FFQ | One single question, total mushroom consumption was adjusted for the total energy intake according to the nutrient density method | Edible mushroom: Lentinula edodes, Auricularia auriculajudae, Pleurotus ostreatus, Flammulina velutipes, Agaricus bisporus, and others | Q4, > 5.52 g/1,000 kcal/d (5,096) | Q1, < 1.76 g/1,000 kcal/d (4,545) | NR | NR | NR | NR | NR | NR | NR | NR | HR, 0.88; 95% CI, 0.80–0.96 | NR | Age, sex, education, BMI, smoking status, employment status, household income, physical activity, family history of disease (including CVD, hypertension, hyperlipidemia, and diabetes), depressive symptoms, metabolic syndrome, hypertension, hyperlipidemia, diabetes, energy, alcohol intake, dietary patterns, baseline serum uric acid, glomerular filtration rate and high-sensitivity C-reactive protein |
| Otsuka et al., 2020 [20] | 3-day dietary record | Mushroom was weighed separately on a 1 kg kitchen scale before being cooked, or portion sizes were estimated and average mushroom intake was calculated according to the Standard Tables of Food Composition in Japan 2010 | NS, dietary mushroom | T3, 27.6 g/d median (268) | T1, 0 g/d (259) | HR, 0.69; 95% CI, 0.51–0.94 | HR, 0.81; 95% CI, 0.36–1.76 | HR, 0.54; 95% CI, 0.17–1.51 | NR | NR | NR | NR | NR | NR | NR | Age, sex, education, BMI, smoking status, physical activity, alcohol intake, and history of hypertension, dyslipidemia, and diabetes mellitus |
| Cheraghi et al., 2016 [18] | 147 food items FFQ | The consumption frequency of mushroom in the past year was assessed and then, using home scale guides, the amount consumed of mushroom was transformed into grams per day | NS, baked mushroom | Yes, 20 g/d (NR) | No, (NR) | NR | NR | NR | NR | NR | NR | NR | NR | NR | OR, 0.3; 95% CI, 0.1–0.7 | Age, cancer (yes/no), hospitalization, job physical activity, sex, BMI, marriage status, and other food items selected by backward-selection method |
| Total number of articles | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||
95% CI, 95% confidence interval; BMI, body mass index; CHD, coronary heart disease; CVD, cardiovascular disease; d, day; HR, hazard ratio; FBG, fasting blood glucose; FFQ, food frequency questionnaire; NR, not reported or not evaluated; NS, not specified; OR, odds ratio; T2DM, type 2 diabetes mellitus; USDA, United States Department of Agriculture.
As for morbidity studies, there were three studies on the occurrence of various conditions such as CVDs [19], CHD [19], stroke [19], T2D [1924], hyperuricemia [21], and MetS [18]. Articles on hyperuricemia [21] and MetS [18] suggested an inverse association (HR, 0.88; 95% CI, 0.80–0.96 for hyperuricemia and OR, 0.3; 95% CI, 0.1–0.7 for MetS).
CMD risk factors in the observational studies and clinical trials
Supplementary Tables 6, 7 and Table 4 present the relationships between the consumption of mushroom and cardiometabolic conditions before the diagnosis of CMDs. Various conditions were examined in the prospective cohort studies and clinical trials as follows: LDL-C, HDL-C, TC, TG, FBG, connecting peptide (C-peptide) C-reactive protein (CRP), interleukin-6 (IL-6), tumor necrosis factor-α receptor type 2 (TNFαR2), body mass index (BMI), waist circumference (WC), systolic blood pressure (SBP), diastolic blood pressure (DBP), glomerular filtration rate (GFR), serum uric acid (SUA), waist/hip index (WHI), triacylglycerols (TAG), alanine aminotransferase (ALT), deoxypyridinoline (DPD), bone-specific alkaline phosphatase (BAP), glutamate oxaloacetate transaminase (GOT), glutamate pyruvate transaminase (GPT), secretory immunoglobulin A (sIgA), aspartate amino transferase (AST), alkaline phosphatase (ALP), and gamma glutamyltransferase (γ-GT). However, limited evidence was available. Among prospective studies (Supplementary Table 5), only 1 study reported the relationship between mushroom consumption and cardiometabolic conditions [19], which used data of mushroom consumption collected in 1986 and of CMDs biomarkers collected between 1989 and 1990 for the Nurses’ Health Study and between 1993 and 1994 for the Health Professional follow up study. They did not found any statistically significant association of mushroom consumption and CMDs biomarkers, as well as several CMDs such as CVDs and T2D.
Table 4
Quantitative summary of experimental studies evaluating cardiometabolic disease risk factors consuming higher vs. lower amounts of mushrooms1)
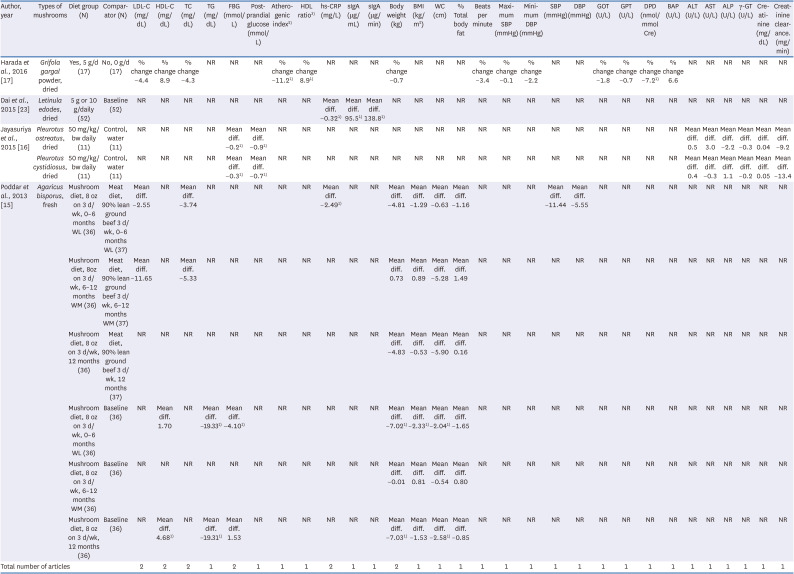
| Author, year | Types of mushrooms | Diet group (N) | Comparator (N) | LDL-C (mg/dL) | HDL-C (mg/dL) | TC (mg/dL) | TG (mg/dL) | FBG (mmol/L) | Postprandial glucose (mmol/L) | Atherogenic index2) | HDL ratio3) | hs-CRP (mg/L) | sIgA (μg/mL) | sIgA (μg/min) | Body weight (kg) | BMI (kg/m2) | WC (cm) | % Total body fat | Beats per minute | Maximum SBP (mmHg) | Minimum DBP (mmHg) | SBP (mmHg) | DBP (mmHg) | GOT (U/L) | GPT (U/L) | DPD (nmol/mmol Cre) | BAP (U/L) | ALT (U/L) | AST (U/L) | ALP (U/L) | γ-GT (U/L) | Creatinine (mg/dL) | Creatinine clearance. (mg/min) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Harada et al., 2016 [17] | Grifola gargal powder, dried | Yes, 5 g/d (17) | No, 0 g/d (17) | % change −4.4 | % change 8.9 | % change −4.3 | NR | NR | NR | % change −11.21) | % change 8.91) | NR | NR | NR | % change −0.7 | NR | NR | NR | % change −3.4 | % change −0.1 | % change −2.2 | NR | NR | % change −1.8 | % change −0.7 | % change −7.21) | % change 6.6 | NR | NR | NR | NR | NR | NR |
| Dai et al., 2015 [23] | Letinula edodes, dried | 5 g or 10 g/daily (52) | Baseline (52) | NR | NR | NR | NR | NR | NR | NR | NR | Mean diff. −0.321) | Mean diff. 95.51) | Mean diff. 138.81) | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Jayasuriya et al., 2015 [16] | Pleurotus ostreatus, dried | 50 mg/kg/bw daily (11) | Control, water (11) | NR | NR | NR | NR | Mean diff. −0.21) | Mean diff. −0.91) | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | Mean diff. 0.5 | Mean diff. 3.0 | Mean diff. −2.2 | Mean diff. −0.3 | Mean diff. 0.04 | Mean diff. −9.2 |
| Pleurotus cystidiosus, dried | 50 mg/kg/bw daily (11) | Control, water (11) | NR | NR | NR | NR | Mean diff. −0.31) | Mean diff. −0.71) | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | Mean diff. 0.4 | Mean diff. −0.3 | Mean diff. 1.1 | Mean diff. −0.2 | Mean diff. 0.05 | Mean diff. −13.4 | |
| Poddar et al., 2013 [15] | Agaricus bisporus, fresh | Mushroom diet, 8 oz on 3 d/wk, 0–6 months WL (36) | Meat diet, 90% lean ground beef 3 d/wk, 0–6 months WL (37) | Mean diff. −2.55 | NR | Mean diff. −3.74 | NR | NR | NR | NR | NR | Mean diff. −2.49 1) | NR | NR | Mean diff. −4.81 | Mean diff. −1.29 | Mean diff. −0.63 | Mean diff. −1.16 | NR | NR | NR | Mean diff. −11.44 | Mean diff. −5.55 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Mushroom diet, 8oz on 3 d/wk, 6–12 months WM (36) | Meat diet, 90% lean ground beef 3 d/wk, 6–12 months WM (37) | Mean diff. −11.65 | NR | Mean diff. −5.33 | NR | NR | NR | NR | NR | NR | NR | NR | Mean diff. 0.73 | Mean diff. 0.89 | Mean diff. −5.28 | Mean diff. 1.49 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | ||
| Mushroom diet, 8 oz on 3 d/wk, 12 months (36) | Meat diet, 90% lean ground beef 3 d/wk, 12 months (37) | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | Mean diff. −4.83 | Mean diff. −0.53 | Mean diff. −5.90 | Mean diff. 0.16 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | ||
| Mushroom diet, 8 oz on 3 d/wk, 0–6 months WL (36) | Baseline (36) | NR | Mean diff. 1.70 | NR | Mean diff. −19.331) | Mean diff. −4.101) | NR | NR | NR | NR | NR | NR | Mean diff. −7.021) | Mean diff. −2.331) | Mean diff. −2.041) | Mean diff. −1.65 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | ||
| Mushroom diet, 8 oz on 3 d/wk, 6–12 months WM (36) | Baseline (36) | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | Mean diff. −0.01 | Mean diff. 0.81 | Mean diff. −0.54 | Mean diff. 0.80 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | ||
| Mushroom diet, 8 oz on 3 d/wk, 12 months (36) | Baseline (36) | NR | Mean diff. 4.68 1) | NR | Mean diff. −19.31 1) | Mean diff. 1.53 | NR | NR | NR | NR | NR | NR | Mean diff. −7.031) | Mean diff. −1.53 | Mean diff. −2.581) | Mean diff. −0.85 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | ||
| Total number of articles | 2 | 2 | 2 | 1 | 2 | 1 | 1 | 1 | 2 | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |||
ALP, alkaline phosphatase; ALT, alanine amino transferase; AST, aspartate amino transferase; BAP, bone-specific alkaline phosphatase; BMI, body mass index; CRP, C-reactive protein; DBP, diastolic blood pressure; DPD, deoxypyridinoline; FBG, fasting blood glucose; γ-GT, gamma glutamyltransferase; GOT, glutamate oxaloacetate transaminase; GPT, glutamate pyruvate transaminase; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; NR, not reported or not evaluated; SBP, systolic blood pressure; sIgA, secretory immunoglobulin A; TC, total cholesterol; TG, triglycerides; WC, waist circumference; WL, weight loss; WM, weight maintain.
1)Results are displayed based on statistically significant differences in the original manuscript. ↑: increase; ↓: decrease; ≠: no change.
2)Atherogenic Index = (TC – HDL-C)/HDL-C.
3)HDL Ratio = (HDL-C/TC) × 100.
Intervention studies regarding cardiometabolic conditions were also insufficient (Table 4, Supplementary Table 6). However, reviewing the literature revealed some possibly beneficial results of mushroom intervention on cardiometabolic risk factors in more than one study or different indices. Fresh mushroom (Agaricus bisporus) [15] and powdered mushroom (Grifola gargal) [17] showed a possible benefit on HDL-C (raised HDL-C concentration; raised HDL-C ratios; lowered atherogenic index.
More than one study has reported beneficial findings for both FBG level [1516] and postprandial glucose level [16], irrespective of whether dried (Pleurotus ostreatus and Pleurotus cystidiosus) [16] or fresh mushroom [15] were consumed. Similarly, inverse associations of high-sensitivity C-reactive protein (hs-CRP) were observed with both dried (Letinula edodes) [23] and fresh mushroom consumption [15]. In terms of obesity indices [17], an weight loss was observed in an intervention of 8 oz on 3 d/wk fresh mushroom for 6 months [15]. TG [15], sIgA [23], and DPD [17] were also inversely associated with mushroom consumption in one study, respectively.
DISCUSSION
For this systematic review examining the relationship between mushroom consumption and the risk of cardiometabolic conditions in the general populations, we selected only five prospective cohort studies and four clinical trials. Reviewing these studies revealed a potentially inverse link with the risk of all-cause mortality, hyperuricemia, and MetS in prospective cohort studies and with some cardiometabolic conditions [blood glucose (both fasting and postprandial), HDL-C (including HDL-C, HDL/TC ratio, and atherogenic index), hs-CRP, and obesity indices (body weight, BMI, and WC). However, it is essential to acknowledge that definitive conclusion could not be drawn due to the limited number of available studies for each cardiometabolic conditions.
In 2021, global production of mushrooms and truffles data was estimated to reach 44.21 tons, primarily in China, marking about 40% increase compared to 33.78 tons in 2012 [25]. Regarding mushroom consumption across countries, China and Japan are supposed to have relatively high mushroom consumption rates [26], although we could not compare mushroom consumption between countries due to variations in units for mushrooms consumption between studies [such as weekly frequencies of mushrooms consumption (times/week), weekly consumption (g/week), and daily amount (g/d or g/1,000 kcal/d)]. But the dosage of mushrooms in clinical trials seemed to be relatively higher (75.6 g/day of the fresh form) [15] than those in observational studies (10–72 g/day in observational studies) [1822], although there was not a big difference.
To date, there was little evidence on CMDs and its conditions related to edible mushroom, despite their functional use over centuries. In the current systematic review, we could select only 9 articles. In terms of cancer, it seemed that mushroom consumption has been consistently reported to be inversely associated in the systematic review and meta-analysis [2728]. Many studies included in those reviews were conducted in Asian countries (China, Japan, and Korea) where the rate of mushrooms consumers are high. The inverse association of the risk of all cancers was also found only in Eastern region, not in Western region, in the meta-analysis [27]. They pointed that the differences between Eastern and Western countries may result from differences in the amounts and types of mushrooms consumed between regions [2627]. This possibility was also suggested in T2D study on mushroom consumption from the Nurses’ Health Study and the Health Professionals Follow-up Study on T2D [19]. However, prospective cohort studies on dietary factors and the risk of CMDs have primarily been conducted in the US and Europe. In these populations, the variation of mushroom consumption between the low and high consumption groups may be narrow, limiting the robustness of research. This limitation could be a crucial factor contributing to the scarcity of evidence regarding the association between mushroom consumption and CMDs and their conditions. Therefore, further evidence on the association between edible mushrooms and each CMD and their risk factor should be obtained and accumulated from large-scale cohort studies, particularly Asian population cohorts.
Despite the limited research, upon a comprehensive examination of the existing studies on the mortality and morbidity of CMDs, the current evidence did not reveal any significant association of mushroom consumption with the mortality and morbidity in CMDs (CVD, stroke, and T2D). Conversely, two different cohort studies suggested an inverse association with hyperuricemia [21] and MetS [18], respectively. First, hyperuricemia was characterized by elevated levels of uric acid in the blood and it has been associated with an increased risk of CMDs, particularly hypertension and CVDs [29] and additionally other metabolic abnormalities such as insulin resistance, dyslipidimia, and obesity [30]. Mushrooms are low in purines, compounds that break down into uric acid, making them a favorable dietary choice for individuals with hyperuricemia [31]. The protective association of mushroom consumption with hyperuricemia may be related to antioxidants of mushrooms, which may help reduce inflammation [5] and oxidative stress [4] associated with elevated uric acid levels. Besides, some studies suggest that certain mushroom species, such as L. edodes (oak mushroom or shiitake), may help lower uric acid levels [32]. We could not support its effect on hyperuricemia, because L. edodes was measured as one of mushrooms for total mushroom consumption and because we could not dissociate the effect of L. edodes on the risk of hyperuricemia from those of other mushrooms. As for MetS, an Iranian cohort study suggested an inverse association of mushroom consumption with the risk of MetS [18].
In terms of cardiometabolic conditions, the potential links of blood glucose, HDL-C lipid profiles, hs-CRP, and obesity were suggested in more than one study or indices: fasting and postprandial blood glucose, HDL-C related indices (HDL-C, HDL-C ratio, and atherogenic index), and obesity indices (body weight, BMI, and WC). Similarly, two previous systematic reviews suggested some potential health benefits, such as lipid profiles and BP [12] and TG, CRP, and some indices of CMD [13]. However, as mentioned earlier, the current systematic review differs from 2 previous systematic reviews in its focus on studies, where mushrooms themselves serve as a primary exposure among the general population, and in the extraction of data from covariates-unadjusted models. Thus, it is worth to note our findings, despite the very limited number of studies. These potential associations of mushrooms with blood glucose, lipid profiles, and weight loss might be related to mushroom bioactive compounds, including polysaccharides, phenolic compounds, and antioxidants, modulate lipid metabolism, glucose regulation, and inflammatory pathways [3334353637]. In addition, properties such as low-calorie content and high fiber [38] may also aid weight management and enhance glycaemic control. Besides, bioactive compounds like beta-glucans [7] and polyphenols [38] in mushrooms may have anti-obesity, anti-diabetic, and lipid-lowering effects. Beta-glucans impact cholesterol metabolism and lipid absorption through bile acids and intestinal microorganisms [7], improving insulin sensitivity, reducing inflammation, and modulating lipid metabolism [33].
To the best of our knowledge, this study is the first systematic review on the epidemiological association of mushroom intake with cardiometabolic health outcomes in the general populations. However, certain limitations should be acknowledged to interpret the findings. Firstly, it is important to recognize that the number of studies is insufficient to draw conclusions for specific cardiometabolic health outcomes, even for the overall CMDs. The scarcity of available data hampers the establishment of robust associations. Secondly, an important consideration is that the variations in the types of mushrooms consumed by different study populations may lead to differences in the types and quantities of bioactive components present [39]. However, due to a dearth of information, we were unable to systematically consider the specific types of edible mushrooms in our review. This may ultimately contribute to the inconsistency in the findings observed across studies, making it challenging to generalize the results. Thirdly, it is important to consider the inherent biases and potential confounding factors that can arise in dietary studies, such as self-recall bias, selection bias, or confounding by other dietary factors. Finally, although studies in the present systematic review considered several covariates in the analyses, it is crucial to note that there remains the possibility of residual or unmeasured confounding factors that could influence the outcomes.
In summary, the available evidence suggests possible associations between mushroom consumption and cardiometabolic health outcomes, including blood glucose, HDL-C related indices, hs-CRP, and obesity indices. Nevertheless, the lack of sufficient studies prevents the drawing of any conclusive recommendations. Therefore, it is crucial to emphasize the need for further investigations to determine the quantitative extent and nature of this relationship. A more comprehensive understanding is imperative for informed and suitable recommendations in the general population.
 XML Download
XML Download