

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Adult congenital heart disease (ACHD) leads to an increased risk of cardiovascular disease (CVD) in later life compared with the general population, despite surgical and medical management of congenital heart disease (CHD) itself. Not only CHD-related complications but also acquired medical conditions can influence mortality in ACHD survivors. CHD has been identified as a significant risk factor for stroke, myocardial infarction, all-cause mortality, and major adverse cardiovascular events in the Korean National Health Insurance Service from 2006 to 2017.1 Additionally, the Dutch CONCOR national registry from 2001 to 2009 demonstrated a significantly higher risk of death in ACHD, particularly those with severe CHD, a history of myocardial infarction, arrhythmias, or heart failure.2
Chronic kidney disease (CKD) is not a result of metabolic syndrome (MS) or cardiorenal syndrome. CKD is a main contributing factor to cardiovascular mortality and morbidity.34 Although the incidence and severity of CKD in the general population has been well reported,56 few studies have the incidence of CKD or its prognostic effects in ACHD. Another cause of early death in ACHD is the high prevalence of MS. Several previous epidemiologic data demonstrated that the survivors from the CHD were more frequently obese, hypertensive, or in abnormal glucose metabolism which are known as risk factors for CVD than non-CHD population.789 The prevalence of MS varies depending on how it is defined, but it ranges from 22% to 36.5% in the general population.1011121314 However, little is known about the incidence of MS in adult Asian patients with CHD. Therefore, we aimed to identify the incidence and prognostic implication of CKD and MS in ACHD.
METHODS
Study population and protocol
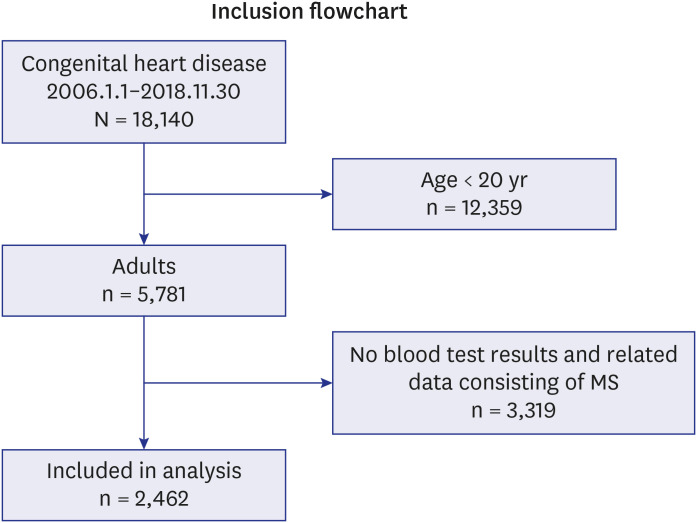
This retrospective cohort study analyzed 2,462 patients with ACHD from a database of 18,140 CHD patients treated at Samsung Medical Center, Seoul, Korea, from 2006 through 2018 (Fig. 1). Systolic blood pressure (SBP), diastolic blood pressure (DBP), body height, body weight, and laboratory data were collected at the time of CHD diagnosis. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Blood samples were collected from the antecubital vein after overnight nil per os. Total cholesterol, triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), fasting blood sugar (FBS), hemoglobin, and serum creatinine level were measured. Anemia was defined as a hemoglobin level < 12g/dL in females and < 13 g/dL in males.15 Information about comorbid conditions such as hypertension, type 2 diabetes mellitus (diabetes), dyslipidemia, angina, myocardial infarction, heart failure, arrhythmia, cerebrovascular accident (CVA, including ischemic stroke, hemorrhagic stroke, and transient ischemic attack), cancer, anemia, and CHD-related surgery/procedures was obtained from the electronic medical records. In this study, we used mortality data from 2006 through 2019 that we obtained from Ministry of the Interior and Safety in Korea.
ACHD
We used primary and secondary diagnosis for ACHD. Specific types of CHD were classified according to the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). Based on the degree of medical complexity and severity of ACHD,1617 we classified the type of ACHD into great complexity and moderate complexity disease. We additionally divided them into cyanotic and acyanotic CHD because these two types significantly differ in disease severity and cardiovascular prognosis (Supplementary Tables 1 and 2).18
CKD
We calculated the estimated glomerular filtration rate (eGFR) using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. The CKD-EPI equation has been widely used in epidemiological studies and clinical practice. CKD was defined as an eGFR of less than 60 mL/min/1.73m2 for at least 3 months. To identify the association between the severity of CKD and clinical outcomes in ACHD, we categorized the degrees of renal dysfunction as stage 1 (≥ 90 mL/min/1.73 m2, n = 1,266), stage 2 (60–89 mL/min/1.73 m2, n = 1,010), stage 3 (30–59 mL/min/1.73 m2, n = 119), stage 4 (15–29 mL/min/1.73 m2, n = 31), and stage 5 (< 15 mL/min/1.73 m2, n = 36).
MS
According to the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) and International Diabetes Federation (IDF) guidelines, MS was diagnosed in the presence of three or more of the following parameters1920: 1) Obesity, defined as a BMI ≥ 25 kg/m2 (World Health Organization, Asia-Pacific guidelines for obesity). We analyzed central obesity using BMI instead of waist circumference (WC). According to the MS criteria of the IDF, if the condition of obesity using BMI can be satisfied, abdominal obesity (as shown by WC) does not need to be measured; 2) TG levels higher than 150 mg/dL (high TG); 3) HDL-C levels less than 40 mg/dL for males, or less than 50 mg/dL for females (low HDL); 4) Hypertension, defined as an SBP greater than 130 mmHg or a DBP greater 85 mmHg (high blood pressure); and 5) FBS greater than 100 mg/dL (high FBS). The subjects were classified into two groups: normal and non-MS (non-MS, n = 1,577) and MS (n = 885).
Statistical analyses
Differences in the general and clinical characteristics of the CKD and MS groups were examined using the student’s t-test for continuous variables and the χ2 test for categorical variables. Simple and multiple logistic regression analyses were used to determine the association between MS as an independent variable and CKD as a dependent variable after adjusting for age, sex, and anemia. Simple and multiple Cox proportional hazards analyses for ACHD were carried out using the variables of age, sex, ACHD complexity, MS, CKD, or degree of renal dysfunction, anemia, comorbidities (angina, myocardial infarction, heart failure, arrhythmia, CVA, and cancer). We also show adjusted hazard ratio (HR) for the coexistence of CKD and MS: non-CKD and non-MS (CKD-MS−, reference), non-CKD and MS (CKD−MS+), CKD and non-MS (CKD+MS−), and CKD and MS (CKD+MS+).
Ethics statement
This study protocol was reviewed and approved by the Institutional Review Board of Samsung Medical Center (IRB number 2019-04-151). Because this study was retrospective, informed consent was exempted by IRB. The exemption of consent does not adversely affect the rights or well-being of the study subjects.
RESULTS
Among the 2,462 ACHD in our study population (mean age 52.5 ± 14.3 years, 48.7% of male), 7.6% had CKD. The ACHD with CKD were older than those with normal renal function. The rate of cardiovascular comorbidities and malignancy also differed significantly between patients with and without CKD. CHD-related surgical interventions were more frequently performed in CKD patients (48.3% vs. 39.5%, P = 0.018). The degree of ACHD complexity was also higher in the CKD group (P = 0.020). The rate of MS was significantly higher in ACHD with CKD than in those without CKD (60.7% vs. 33.9%, P < 0.001). In our entire study population, 113 (4.6%) had both MS and CKD (Table 1, Supplementary Table 3).
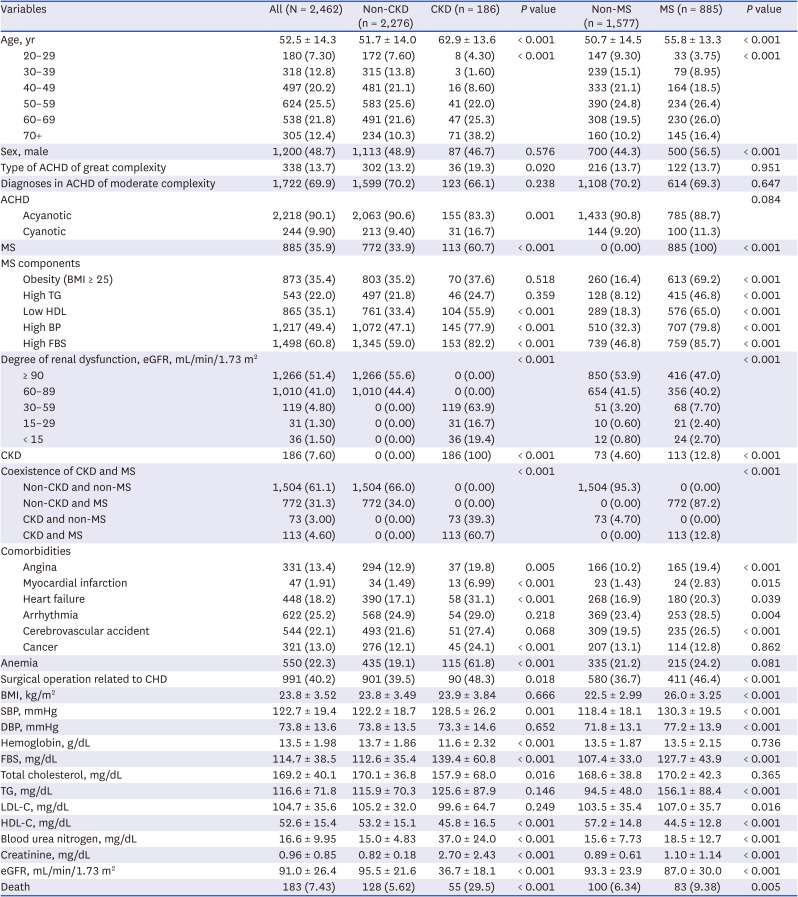
Table 1
Distribution of general and clinical factors according to CKD and MS in ACHD (N = 2,462)
Values are presented as mean ± standard deviation or number (%).
CKD = chronic kidney disease, MS = metabolic syndrome, ACHD = adult congenital heart disease, BMI = body mass index, TG = triglyceride, HDL = high-density lipoprotein, BP = blood pressure, FBS = fasting blood sugar, eGFR = estimated glomerular filtration rate, CHD = congenital heart disease, SBP = systolic blood pressure, DBP = diastolic blood pressure, LDL-C = low-density lipoproteins cholesterol, HDL-C = high-density lipoproteins cholesterol.
![]()
The overall incidence of MS in ACHD was 35.9%. Patients with MS were more frequently male and older than those without MS (male: 56.5% vs. 44.5%, P < 0.001, and age: 55.8 ± 13.3 years vs. 50.7 ± 14.5 years, P < 0.001). The incidence of MS did not differ significantly according to ACHD complexity. All 5 parameters indicating MS were much more abnormal in the MS group than the non-MS group (all P < 0.001). Patients with MS also showed a higher incidence of CKD than those without MS (12.8% vs. 4.6%, P < 0.001). CHD-related surgical interventions were more frequently performed in the MS group (46.4% vs. 36.7%, P < 0.001). Although the complexity and severity of ACHD did not differ between patients with and without MS, the rate of angina (P < 0.001), myocardial infarction (P = 0.015), heart failure (P = 0.039), arrhythmia (P = 0.004), and CVA (P < 0.001) was higher in the MS group than the non-MS group (Table 1).
CKD was significantly associated with MS and its components regardless of the age, gender, or the presence of anemia. The adjusted odds ratio (OR) for MS was 2.62 (95% confidence interval [CI], 1.89–3.63) (Table 2).
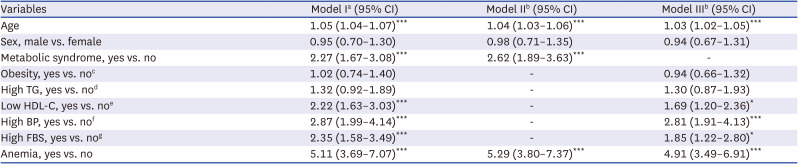
Table 2
Adjusted OR and 95% CI for CKD with and without MS or MS components
OR = odds ratio, CI = confidence interval, CKD = chronic kidney disease, MS = metabolic syndrome, TG = triglyceride, HDL-C = high-density lipoproteins cholesterol, BP = blood pressure, FBS = fasting blood sugar.
aLogistic regression after adjustment for age.
bWith adjustments for age, sex, and anemia, the adjusted OR for CKD with and without MS in Model II and the adjusted OR for CKD with and without MS components in Model III were calculated.
cBody mass index ≥ 25 kg/m2.
dTG levels ≥150mg/dL.
eHDL-C < 40 mg/dL in males or < 50 mg/dL in females or use of antilipidemic drug therapy.
fBlood pressure ≥ 130/85 mmHg or use of antihypertensive drug therapy.
gFBS ≥ 100 mg/dL or use of oral hypoglycemic agents or insulin.
*P < 0.05, ***P < 0.001.
![]()
ACHD patients who were older than 60 years, male, with the great complexity type of ACHD, CKD, myocardial infarction, or cancer were significantly associated with increased all-cause mortality (Table 3). Although the presence of MS was initially associated with mortality in the univariate analysis, this connection became insignificant after adjusting for other clinically relevant factors. On the other hand, the presence of CKD was independently associated with increased mortality and this association was proportional to the severity of renal failure. The adjusted HR for CKD on mortality was higher than other variables related to survival. Specifically, the coexisting MS and CKD in ACHD was significantly associated with mortality, regardless of their cardiovascular comorbidities. Moreover, the adjusted HR for myocardial infarction and cancer were found to be higher for mortality. However, the adjusted HR for angina for mortality was negative.
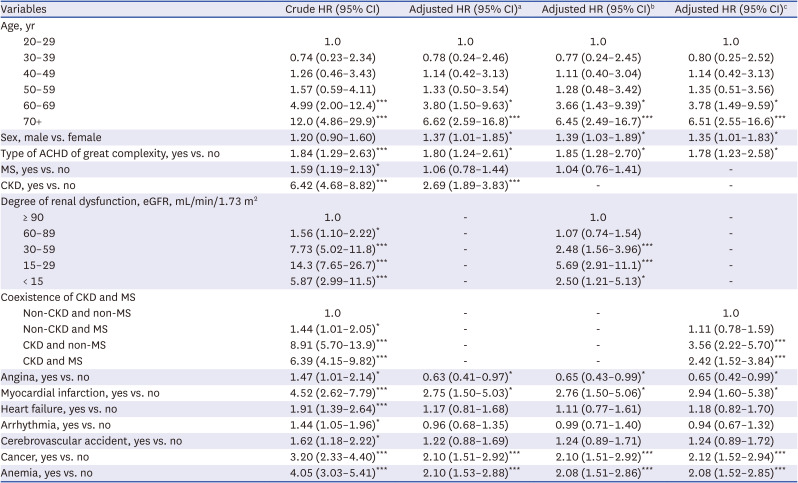
Table 3
HR and 95% CI for mortality in ACHD after adjusting for age and other confounders
HR = hazard ratio, CI = confidence interval, ACHD = adult congenital heart disease, MS = metabolic syndrome, CKD = chronic kidney disease, eGFR = estimated glomerular filtration rate.
aEstimated by multiple Cox proportional hazard model analyses after adjusting for age, sex, type of ACHD of great complexity, MS, CKD, angina, myocardial infarction, heart failure, arrhythmia, cerebrovascular accident, cancer, and anemia.
bEstimated by multiple Cox proportional hazard model analyses after adjusting for age, sex, type of ACHD of great complexity, MS, eGFR grade, angina, myocardial infarction, heart failure, arrhythmia, cerebrovascular accident, cancer, and anemia.
cEstimated by multiple Cox proportional hazard model analyses after adjusting for age, sex, type of ACHD of great complexity, coexistence of MS and CKD, angina, myocardial infarction, heart failure, arrhythmia, cerebrovascular accident, cancer, and anemia.
*P < 0.05, ***P < 0.001.
![]()
In additional analyses related to the coexistence of CKD and MS, the death distribution during follow up was 4.92% in CKD−MS− patients, 6.99% in CKD−MS+ patients, 35.6% in CKD+MS− patients, and 25.6% in CKD+MS+ patients (Supplementary Table 3).
DISCUSSION
In this study, we investigated the incidence and prognostic implications of CKD and MS in ACHD. MS commonly accompanies ACHD. Although the presence of MS was not independently associated with clinical outcomes in multiple analysis, it correlated closely with the presence of CKD. All-cause mortality was significantly higher in CKD patients than in those without CKD, regardless of MS.
Previous studies demonstrated that CKD occurred more frequently in CHD patients than in the general population.2122 CHD patients have several risk factors that make them more likely than others to develop CKD later in life including pathophysiological changes related to a structurally abnormal heart and circulation such as chronic hypoxia, changes in renal blood flow, impaired neurohormonal activation, and chronic cardiorenal syndrome.21 Our data show that ACHD patients with CKD face increased mortality compared to those without CKD. The presence of CKD is a well-known independent prognostic factor for CVD, even after adjusting for cardiovascular risk factors such as hypertension and diabetes.23 Especially in elderly survivors of ACHD, the presence of CKD was one of the strongest predictors of mortality.24 Therefore, close monitoring and management of renal dysfunction in ACHD is very important.
Compared with the general population data in the Korea National Health and Nutrition Examination Survey,1125 the incidence of MS was also higher in ACHD.26 This high incidence of MS has several possible explanations. CHD patients often have limited activity and a sedentary lifestyle due to their underlying disease,27 and a focus on treating the CHD might neglect management of MS. Furthermore, the restriction of exercises may have been common due to CHD.28
In our data, the presence of MS was not independently associated with increased mortality in multiple analysis, perhaps for the following reasons. First, although obesity is one of the main factors used to diagnose MS, many studies have reported that obesity is associated with favorable cardiovascular outcomes.293031 However, in concordance with our data, among 3,069 ACHD patients in London, United Kingdom, from 2001 to 2015, those with a higher BMI showed lower mortality.32 Second, although we did not examine our patients’ medication histories, the lipid profiles, blood sugar levels, and blood pressures in the MS group at the time of presentation were within the normal ranges. Lastly, in this study, the mean LDL-C in the MS group was 107.0 (± 35.7) mg/dL, which is lower than that of the general population.25 Therefore, MS could have a neutralizing effect on the HR for mortality in ACHD.24
We found an association between CKD and MS in ACHD by observing that, as CVD risk factors, CKD and MS correlated with cardiovascular outcomes in this study. As an anatomical factor attributable to the CHD itself, we found no difference between the MS and non-MS groups in ACHD complexity or diagnoses. However, the CKD groups had worse ACHD complexity than the non-CKD groups. Surgical operations to treat CHD as an intervention factor occurred more frequently in the CKD and/or MS groups than in the non-CKD and/or non-MS groups. Unfortunately, we could not conduct sufficient subgroup analysis, such as between the CKD+MS+ and the CKD+MS− groups or among the degrees of renal dysfunction, to further investigate the association with the increased death rate.
Furthermore, our study found that among the cardiovascular comorbidities, the adjusted HR for myocardial infarction, and cancer was higher in ACHD, which is consistent with earlier studies.3334353637 For instance, the Swedish National Patient Register from 1970 to 2017 identified myocardial infarction as a significant risk factor for death in ACHD,38 and multiple large population studies have shown that cancer is a major cause of death in ACHD.39
Our study has several limitations. First, as it is a retrospective study, we cannot establish a cause-and-effect relationship between CKD or MS and mortality. Second, the study was conducted in a single tertiary hospital in Seoul, Korea, which may limit the generalizability of the findings to other populations and settings. Therefore, further research is needed to evaluate the effect of treatment or interventions on clinical outcomes for individuals with CKD or MS in the ACHD patients.
In conclusion, while the distribution of MS is higher in ACHD, our study found that ACHD with CKD had increased mortality compared to those without CKD, regardless of the presence of MS. Furthermore, MS was closely associated with CKD in ACHD. Therefore, survivors of ACHD should receive close monitoring and management of their renal dysfunction and metabolic parameters to improve their clinical outcomes.
 XML Download
XML Download