

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Breast-conserving surgery (BCS) is the most commonly performed surgical treatment for early-stage breast cancer today [1]. The long-term oncological results and feasibility of BCS are well described, but aesthetic outcomes according to patient opinion are not fully understood [2]. However, preserving the external appearance of the breast has better psychosocial effects after breast cancer surgery [3].
Since the 1990s, the concept of oncoplastic surgery (OPS) has been developed to improve BCS to provide better aesthetic and functional outcomes. In addition, OPS has expanded the indications for BCS by avoiding mastectomy in some cases [4]. European Organization for Research and Treatment of Cancer (EORTC) developed the Quality of Life Questionnaire Core 30 (QLQ-C30) for the evaluating overall quality of life in cancer patients in 1993 [5]. After that, EORTC developed QLQ-Breast Cancer (QLQ-BR23) with only breast cancer-specific items [6]. However, the QLQ-BR23 has a limitation due to it not reflecting the satisfaction of patients who underwent OPS [7]. EORTC developed a new questionnaire named QLQ-Breast Reconstruction module (QLQ-BRECON23) to measure satisfaction in patients undergoing breast reconstruction in 2018. QLQ-BRECON23 was used in the study due to ease of application, objective sexual scale evaluation, and containing specific questions for patients undergoing reconstruction [8].
In recent years, there have been studies evaluating the effectiveness of the QLQ-BRECON23 in patients with post-mastectomy breast reconstruction [910]. However, there is no study in the literature comparing the satisfaction of BCS and OPS by using the QLQ-BRECON23.
We aimed to compare overall quality of life and satisfaction with breast reconstruction in patients undergoing BCS and OPS using QLQ-C30 and QLQ-BRECON23.
METHODS
Patients
This cross-sectional descriptive study was conducted on consecutive patients who were operated on for invasive breast cancer in a tertiary hospital by 2 surgical oncology specialists between January 1, 2018 and December 31, 2021. Participants were divided into 2 groups; underwent BCS (lumpectomy) or OPS. The data on the patient, tumor and treatment characteristics were obtained from a prospectively collected database at the hospital.
Ethical approval was obtained from the Institutional Clinical Research Ethics Committee of Mustafa Kemal University (date, January 13, 2022; No. 07). The principles of the Helsinki Statement have been followed. All participants signed a written informed consent form when they came for postoperative examination.
Eligibility criteria
The inclusion criteria were as follows: (1) female patients who underwent invasive breast carcinoma diagnosed previously by core biopsy, (2) patients aged 18 years or older, (3) patients who underwent lumpectomy or OPS, (4) patients with complete medical and pathological records, (5) patients with no neoadjuvant therapy, (6) patients who finished their treatments and passed at least 6 month after surgery, and (7) patients who were able to speak Turkish. The exclusion criteria were as follows: (1) patients aged 18 years or younger, (2) patients with an inability to understand or complete the questionnaires, (3) patients with incomplete medical or pathological data, (4) patients with synchronous and/or metastatic disease, (5) patients with recurrent or bilateral breast cancer, or underwent mastectomy, (6) patients who underwent replacement techniques (such as perforator-based flap, muscle sparing latissimus dorsi flap, and rectus abdominis myocutaneous flap), (7) patients with expander/implant reconstruction, and (8) patients who developed nipple-areolar complex necrosis.
Procedure
All patients were evaluated by clinical exam, mammography, ultrasonography, and/or MRI in the preoperative period. According to Consensus Definition and Classification System, we performed BCS if the resection was less than 20% of the breast volume and we performed OPS for larger resections [11]. In this study, lumpectomy was defined as the resection of breast tissue from the overlying skin to the major pectoral fascia with negative surgical margins and without skin. OPS was defined as volume displacement techniques and repositioning of the nipple with mobilization of the glandular tissue. Axillary lymph node dissection or sentinel lymph node dissection was performed for all patients. Radiotherapy was performed postoperatively for all breast-conserving patients. Chemotherapy and hormonal treatment were given according to recent national guidelines [12]. The patients were followed up by the operating surgeons and their data were prospectively recorded. Recorded data includes surgical techniques, postoperative complications, age, follow-up time, tumor size, distance to the closest negative margin, the volume of breast specimen, histological tumor type, immunohistological subtypes of tumor, tumor laterality, tumor location, the status of re-excision, axillary management techniques, the status of postsurgical treatment, and preoperative brassiere size. The volume of the breast specimen was calculated with data from the pathology report. The preoperative brassiere size reported by the patients was used to predict the volume of the breast.
Measures
Turkish versions of QLQ-C30 [13] and QLQ-BRECON23 [14] were used for the study. QLQ-C30 is made of 30 questions and evaluates psychosocial well-being, fatigue symptoms, and overall quality of life. A low score indicates a high quality of life for the first 28 questions associated with psychosocial well-being and fatigue symptoms. These questions were scored between 1 and 4 points. A high score indicates a high quality of life associated with the overall quality of life for the 29th and 30th questions. These questions were scored between 1 and 7 points.
QLQ-BRECON23 is made up of 23 questions and evaluates sexual well-being, sensation of the operative area, and satisfaction with the reconstruction. However, 5 questions were excluded from this study due to their association with flap reconstruction techniques. Finally, 18 questions were asked and scored between 1 and 4 points. A low score indicates a high quality of life associated with sexual well-being and sensation of the operative area for the first 6 questions. A high score indicates a high quality of life associated with satisfaction with the reconstruction for the last 12 questions.
Full English and Turkish versions of the EORTC QLQ-C30 and EORTC QLQ-BRECON23 were included in Supplementary Materials 1, 2, 3, 4.
Statistical analyses
We used IBM SPSS Statistics for Windows, ver. 25.0 (IBM Corp.) for data analyses. The normality of the distribution of continuous variables was assessed via the Kolmogorov-Smirnov test. The normally distributed continuous variables were given as mean ± standard deviation and were analyzed by using the Student t-test. The non-normally distributed continuous variables were expressed as median (range) and were analyzed by using the Mann-Whitney U-test. The categorical variables were given as frequency (percentages) and were analyzed by using the chi-square test or Fisher exact test as appropriate. A 2-sided P-value of <0.05 was considered significant.
RESULTS
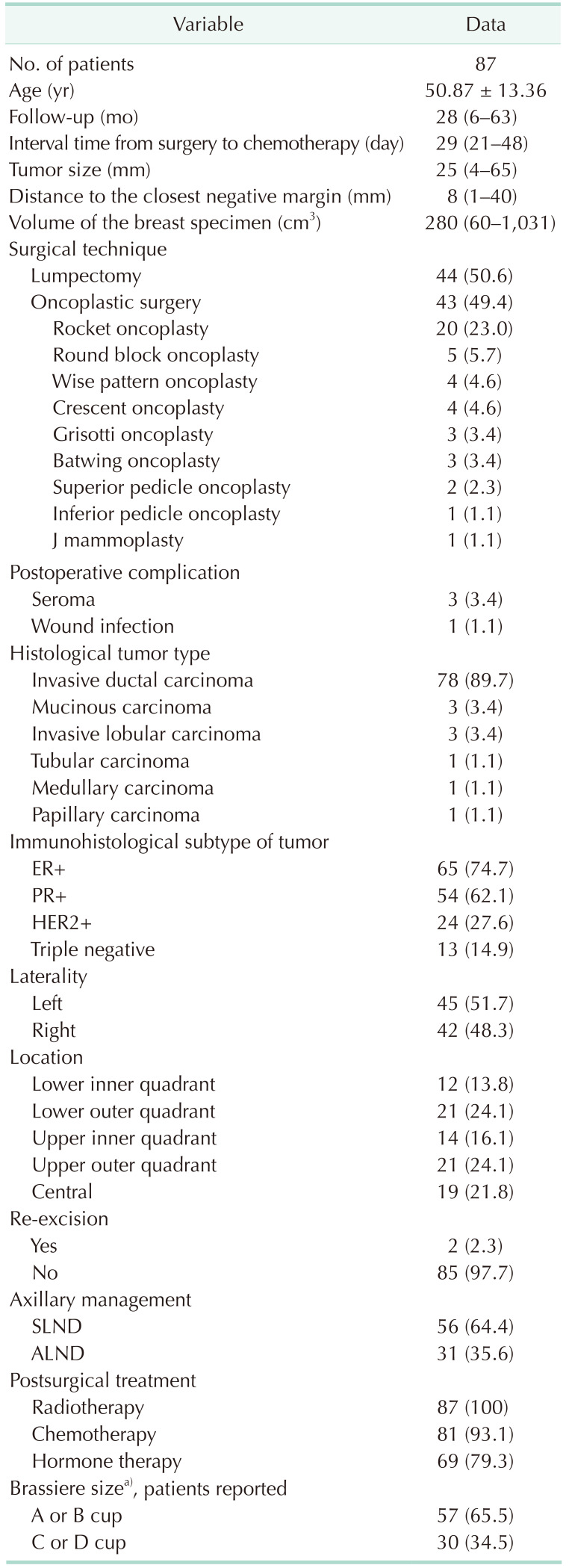
A total of 87 patients were included in this study. The mean age of participants was 50.87 ± 13.36 years. The median follow-up time was 28 months (range, 6–63 months). The interval time from surgery to chemotherapy was 29 days (range, 21–48 days). Table 1 shows the demographic characteristics of all patients.
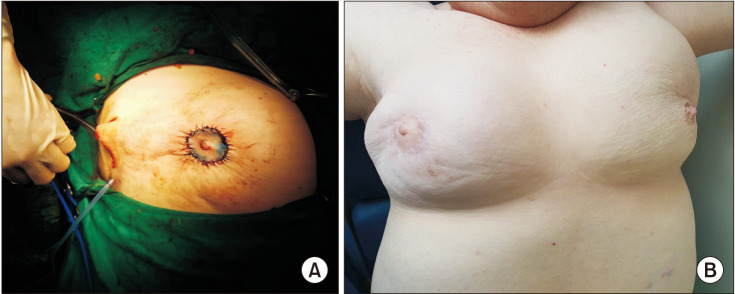
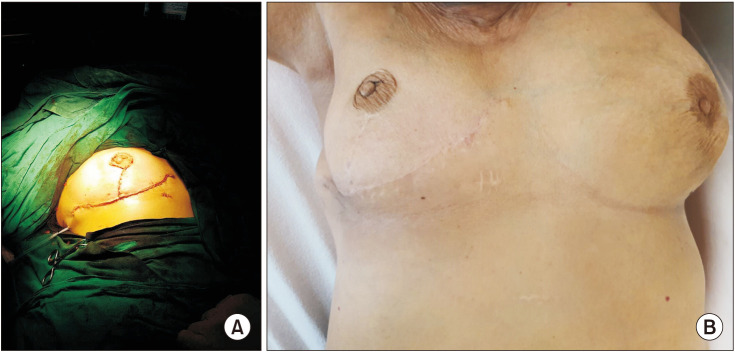
Among patients, 43 (49.4%) underwent OPS, and 44 (50.6%) underwent lumpectomy. Nine different surgical procedures of oncoplastic techniques were performed. Rocket OPS was the most common technique (n = 20, 23.0%) (Fig. 1), followed by round block OPS (n = 5, 5.7%) (Fig. 2), wise pattern OPS (n= 4, 4.6%) (Fig. 3), crescent OPS (n = 4, 4.6%), Grisotti OPS (n= 3, 3.4%) (Fig. 4), batwing OPS (n = 3, 3.4%) (Fig. 5), superior pedicle OPS (n = 2, 2.3%), inferior pedicle OPS (n = 1, 1.1%), and J mammoplasty (n = 1, 1.1%). Totally, 4 postoperative complications occurred; 3 seromas (3.4%) and 1 wound infection (1.1%). All were treated conservatively.
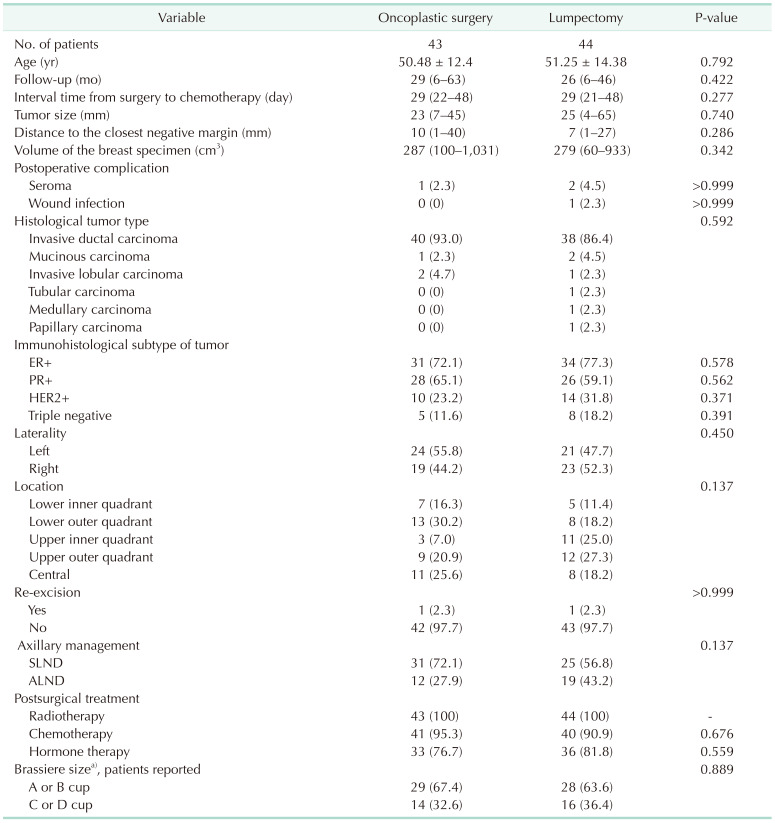
There was no significant difference between the 2 groups in terms of age, follow-up time, interval time from surgery to chemotherapy, tumor size, distance to the closest negative margin, the volume of the breast specimen, histological tumor type, laterality, location, re-excision, axillary management, postsurgical treatment, and brassiere size. The patients and tumor characteristics of the 2 groups are shown in Table 2.
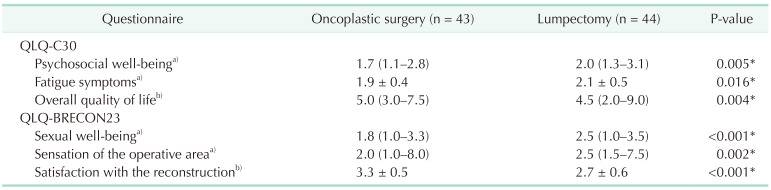
According to QLQ-C30 evaluation, there were significantly better outcomes for patients treated with OPS than those with BCS in terms of psychosocial well-being, fatigue symptoms, and overall quality of life (P = 0.005, P = 0.016, and P = 0.004; respectively). According to QLQ-BRECON23 evaluation, there were also significantly better outcomes in terms of sexual well-being, sensation of the operative area, and satisfaction of the reconstruction (P < 0.001, P = 0.002, and P < 0.001; respectively) (Table 3).
DISCUSSION
Since the first publications related to breast cancer described there was no difference between mastectomy and BCS for survival, the studies have continued to investigate surgical procedures on overall quality of life, and social, psychological, and sexual impact [15]. Aesthetic results after lumpectomy may not be satisfactory in nearly 30% of patients. Deformity and asymmetry may complicate physical adaptation and delay return to normal, remaining as a reminder of cancer [16]. OPS provides the opportunity to further expand the indications for BCS by changing the resection margins in patients whose tumor/breast size ratio is not suitable [17]. The rate of dissatisfaction is between 0% and 18% in patients undergoing OPS in the literature [18]. There are many factors that affect dissatisfaction after surgery such as age, tumor size, breast size, location of tumor, and excised breast volume [18]. The effect of excised breast volume on cosmetic outcomes was investigated in Asian patients undergoing OPS. In patients who underwent oncoplastic technique with less than 20% breast volume resection, satisfaction was found significantly higher regardless of tumor volume and distance from the tumor to the nipple. More complicated oncoplastic surgeries, such as replacement techniques, were recommended for patients if breast volume excision exceeded 20% [19]. In our study, it was important for standardization that there was no difference between the 2 groups in terms of volume of breast specimen and preoperative breast size.
In a study comparing the oncological outcomes of OPS and BCS, it was found that OPS is suitable for larger tumors (P = 0.002) and has a higher specimen weight (P < 0.0001) and volume (P < 0.0001), a wider negative surgical margin, and a lower recurrence rate (P = 0.002). No difference was observed in the complication rates. Considering the oncological results, it was emphasized that OPS is more advantageous [20]. In a meta-analysis conducted on oncological safety and survival rates between 2 surgical techniques (that were OPS and BCS), it was found that re-excision was lower in patients who underwent OPS (P = 0.009), but the positive surgical margin rate was not significantly different (P = 0.191). Other demographic data were similar between the 2 groups, and there were no differences in disease-free survival (hazard ratio [HR], 1.19; P = 0.112) and overall survival (HR, 1.14; P = 0.527) [21]. In our study, also there were no differences between the 2 groups in terms of demographic and oncological outcomes.
A study used the Breast Cancer Treatment Outcome Scale (BCTOS) to compare the aesthetic results of OPS and BCS. The patients were divided into 3 groups according to their aesthetic satisfaction after the questionnaire as good, intermediate, and poor outcomes. Tumor multifocality (P = 0.022), larger tumors (P = 0.033), and weight of breast specimens (P < 0.001) were found to be predictors of poor aesthetic outcomes for all patients. However, tumor multifocality did not predict poor aesthetic outcomes in patients who underwent OPS (P = 0.836). As a result, OPS has been recommended in patients with multifocal tumors [22].
“Breast Cancer Conservative Treatment. Cosmetic results (BCCT.core)” is a software program that discriminates aesthetic evaluation between 4 categories objectively (excellent, good, fair, and poor) [23]. In a study investigating the aesthetic results of patients who underwent BCS, using Breast-Q score and the BCCT.core evaluation, there was a significant association between the 2 methods in terms of breast satisfaction (odds ratio [OR], 3.4; 95% confidence interval [CI], 1.7–6.8) and physicosocial well-being (OR, 2.2; 95% CI, 1.1–4.2)] [24]. Similarly, Kim et al. [25] compared Breast-Q score and BCCT.core in 64 patients who underwent latissimus dorsi flap, and they found a significant correlation between the 2 evaluation methods in terms of satisfaction with all parameters. In another study, the OPS group had higher excellent aesthetic outcomes than the BCS group according to BCCT.core software analysis (P = 0.028). In addition, age over 70 years (P = 0.005), larger breast size (P < 0.001), and tumors in inferior, medial, central quadrants (P < 0.001) were significant risk factors for poor aesthetic outcomes after BCS [18]. In another similar study, psychosocial well-being was significantly better in patients treated with OPS than those treated with BCS (OR, 2.15; 95% CI, 1.25–3.69). However, there were no significant differences between the 2 techniques in terms of physical well-being (OR, 0.83; 95% CI, 0.50–1.39), satisfaction with breast (OR, 0.95; 95% CI, 0.57–1.59), and sexual well-being (OR,1.42; 95% CI, 0.78–2.58) [26]. A study, after the validation of QLQ-BRECON23, by Winters et al. [8] reported that it could be used safely in patients who underwent breast reconstruction instead of the QLQ-BR23. The symptom and function scales of BRECON23 were found between 0.61 to 0.87 [27]. There is only one study in Turkey using QLQ-BRECON23 [14]. This study compared the effect of surgical techniques on satisfaction in patients who were operated on with the diagnosis of periductal mastitis. It was emphasized that the round block method and periareolar combined radial incision techniques can be used safely. In our study, unlike other studies, the recently validated QLQ-BRECON23 was used. In addition, breast satisfaction was analyzed in 3 different subcategories as sexual well-being, the sensation of the operative area, and satisfaction with the reconstruction. We found that OPS was significantly better than BCS in all categories.
A major limitation of the study is that it was designed as a single-centered retrospective study. Therefore, there was no randomization and the study population was small. Another limitation was tumor locations and oncoplastic techniques being non-homogeneous.
We found that the overall quality of life and satisfaction with breast reconstruction in patients undergoing OPS are better than BCS. Although similar outcomes have been obtained with many old questionnaires in the literature, our study is critical because it is the first study comparing OPS and BCS using the QLQ-BRECON23, which was recently validated.



 XML Download
XML Download