

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Food allergy (FA) is a potentially life-threatening reaction after exposure to a food allergen, and allergic reactions may differ depending on the amount of food antigens, cooking methods, and the presence of co-factors, making serious allergic reactions unpredictable.1 In Asia, the overall prevalence of FA is estimated to affect 1–5% of children, and the incidence of food-related anaphylaxis in children has more than doubled over the past few decades.234 The mortality rate of food-induced anaphylaxis is reported to be approximately 0.03 to 0.3 deaths per million person years in the Unites States.5
Caregivers of children with FAs always have to do additional work to prepare allergen-free foods and avoid exposure to food allergens at schools and restaurants and during social activities.6 Moreover, they are concerned about nutrient deficiencies that may arise from restricting allergenic foods.7 Previous studies have demonstrated that parents of children with FAs had poorer quality of life (QoL) and social relationships compared to those of healthy children.89 It has been reported that caregivers of children with peanut allergy have higher average levels of anxiety than the general population.10 Furthermore, anaphylaxis increases the risk of psychiatric problems such as posttraumatic stress symptoms, anxiety, and depression in patients and their mothers.11 Therefore, it is important to investigate the psychosocial impact of FAs on children and their families.12
The Food Allergy Quality of Life-Parental Burden (FAQL-PB) questionnaire was developed in the United States to assess the burden of care of parents of children aged 0–17 years diagnosed with FAs,13 and it has been widely used.1415 Although it has been translated into Korean, its validity and reliability have not been verified.16 In this study, we aimed to validate the Korean version of FAQL-PB and identify factors related to parental psychosocial burden of caring for children with FA.
METHODS
Study design and participants
Parents of children between 6 months and 17 years with immunoglobulin E (IgE)-mediated FAs were recruited from five university hospitals between November 2020 and September 2021. They were given questionnaires to be completed. Diagnosis of FA was based on either: 1) a convincing history of repetitive allergic reactions (urticaria, angioedema, cough, wheezing, dyspnea, vomiting, diarrhea, abdominal pain, and hypotension) occurring within 2 hours after ingestion of offending foods with a specific IgE test > 0.35 kU/L or 2) a positive oral food challenge test within the past 12 months. Patients with pollen-food allergy syndrome were excluded from this study.
Translation and culture adaptation of FAQL-PB
The FAQL-PB consists of 17 items on a seven-point scale ranging from “not at all (1)” to “extremely (7).” The total score ranges from 17 to 119 and can be divided by 17 to obtain a mean total score from 1 to 7. A higher score indicates greater parental burden. The FAQL-PB was translated into Korean according to the World Health Organization guidelines.17 Forward translation into Korean was performed by two independent bilingual speakers.16 An expert panel consisting of three pediatric allergists reviewed the translated version and created a pre-final version. This version of the FAQL-PB was translated back into English by four independent bilingual speakers. The expert panel discussed the differences between the original and back-translated versions, and any discrepancies were revised in the final version. Then, 12 parents of children with FAs were individually interviewed face-to-face for interpretation and cultural adaptation, and there was no misunderstanding or misinterpretation of the questionnaires.
Data collection
Demographic information and clinical characteristics of the patients were obtained from their parents. To investigate the concurrent validity, participants asked to filled out the FAQL-PB, the Korean version of the Food Allergy Independent Measure-Parent Form (FAIM-PF),18 and the Korean version of Child Health Questionnaire-Parents Form 28 (CHQ-PF28) (Table 1).19202122232425 CHQ-PF28 was a generic health-related quality of life questionnaire (HRQLQ), while FAIM-PF was disease-specific FA measure questionnaire. The Korean version of Beck Anxiety Inventory (BAI),2122 the Korean version of Patient Health Qustionnaire-9 (PHQ-9),23 and the Korean version of Connor-Davidson Resilience scale (CD-RISC)2425 were also completed by study participants (Table 1). The CHQ-PF28, BAI, PHQ-9, and CD-RISC were validated with Korean versions and were approved by the survey owners for use in this study.
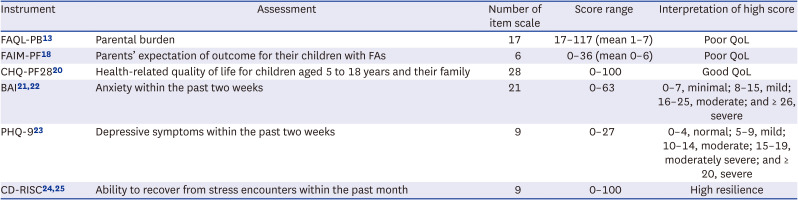
Table 1
Instruments for parents of children with FA
| Instrument | Assessment | Number of item scale | Score range | Interpretation of high score |
|---|---|---|---|---|
| FAQL-PB13 | Parental burden | 17 | 17–117 (mean 1–7) | Poor QoL |
| FAIM-PF18 | Parents’ expectation of outcome for their children with FAs | 6 | 0–36 (mean 0–6) | Poor QoL |
| CHQ-PF2820 | Health-related quality of life for children aged 5 to 18 years and their family | 28 | 0–100 | Good QoL |
| BAI2122 | Anxiety within the past two weeks | 21 | 0–63 | 0–7, minimal; 8–15, mild; 16–25, moderate; and ≥ 26, severe |
| PHQ-923 | Depressive symptoms within the past two weeks | 9 | 0–27 | 0–4, normal; 5–9, mild; 10–14, moderate; 15–19, moderately severe; and ≥ 20, severe |
| CD-RISC2425 | Ability to recover from stress encounters within the past month | 9 | 0–100 | High resilience |
FA = food allergy, FAQL-PB = Food Allergy Quality of Life-Parental Burden, FAIM-PF = Food Allergy Independent Measure-Parent Form, CHQ-PF28 = Child Health Questionnaire-Parents Form 28, BAI = Beck Anxiety Inventory, PHQ-9 = Patient Health Qustionnaire-9, CD-RISC = Connor-Davidson Resilience scale, QoL = quality of life.
![]()
Statistical analysis
All analyses were performed using STATA version 16 (StataCorp LLC, College Station, TX, USA). Descriptive statistics for demographic and clinical characteristics were presented using mean ± standard deviation (SD) for continuous data, whereas, using frequencies and percentage for categorical data. Statistical analyses for validation included internal consistency, floor or ceiling effects, test-retest reliability, concurrent validity, dimensionality, and discriminative validity. Cronbach’s α was used to measure the internal consistency of the FAQL-PB. Each scale value above 0.8 was considered to show a unitary construct. The floor/ceiling effect was calculated as the percentage of subjects with the lowest/highest score on the questionnaire, and < 15% was acceptable. Test-retest reliability was assessed by estimating the intra-class correlation (ICC) between the FAQL-PB scores rated at one-week intervals in eight randomly selected participants. An ICC of 0.70 or higher was regarded as excellent test-retest reliability. For concurrent validity, Pearson’s correlation was used to determine the relationship between FAQL-PB and other questionnaires such as CHQ-PF28 and FAIM-PF. Dimensionality, was assessed using principle components factor analysis with an orthogonal varimax rotation and scree plot with a cut-off of an eigenvalue of greater than 1. Items with factor-loading ≥ 0.40 were considered to make important contributions to the classification. For discriminant validity, t-test was performed to assess differences in FAQL-PB scores according to the experience of anaphylaxis or restricted food allergens.
Univariate and multivariate linear regression analyses were used to investigate the association between potential risk factors and parental burden. Variables for adjustment included age, sex, and children’s underlying diseases. Covariates with a P value < 0.1 in univariable analyses were chosen for the multivariable analyses. A P value < 0.05 was considered significant.
Ethics statement
Written informed consent was obtained from the parent participants prior to participation in the study. The protocol was reviewed and approved by the Institutional Review Boards (IRBs) of each institute (IRB number: SMC 2020-08-090, SMC 2020-06-124, CNUSH 2020-10-010-005, KUGH 2020-10-011, HKS 2020-12-005, and PNUH 2101-026-099).
RESULTS
Characteristics of study participants
Of the 190 parents enrolled in this study, 177 (93.2%) were mothers (Table 2). The mean age of children and their caregivers was 5.7 ± 3.2 years and 38.3 ± 4.6 years, respectively. The most common offending food was egg white (87.4%), followed by cow’s milk (CM; 54.2%) and wheat (46.3%). Overall, 62.1% and 66.8% of patients experienced anaphylaxis and used self-injectable epinephrine, respectively. The mean value of FAQL-PB was 4.3 ± 1.3. The highest burden was observed in social activity limitation, with a mean score of 5.3±1.4 (Fig. 1). The mean BAI score of the caregivers was 7.2 ± 7.8 (65.6%, normal; 21.2%, mild; 10%, moderate; and 3.2%, severe). The mean PHQ-9 and CD-RISC scores were 4.8 ± 5.1 (59.4%, normal; 25.3%, mild; 9.5%, moderate; 3.7%, moderately severe; 2.1%, severe) and 61.3 ± 13.9, respectively. Individual psychosocial scores of the study participants were presented using a bubble plot (Fig. 2A). Moderate to strong positive correlation (coefficient 0.407 to 0.661) was observed between FAQL-PB, BAI, and PHQ-9 scores, whereas moderate negative correlation was observed between FAQL-PB and CD-RISC scores (all P < 0.001) (Fig. 2B).
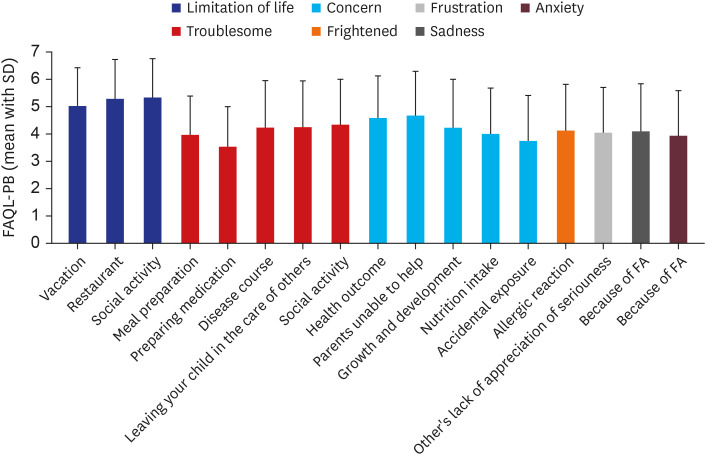
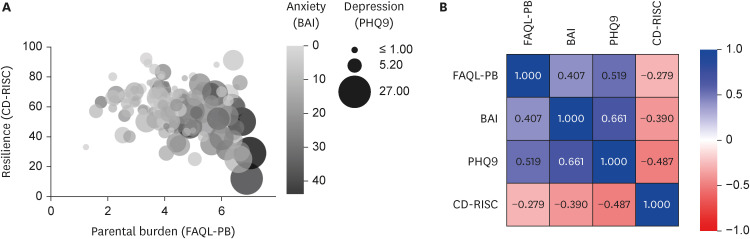
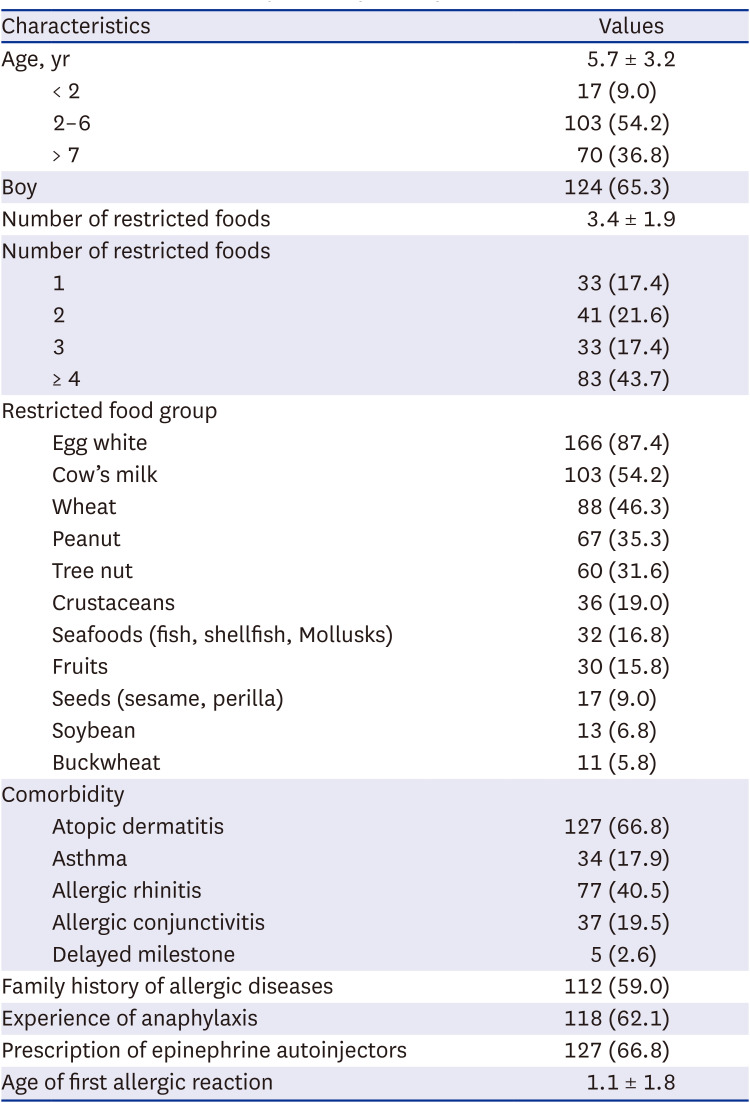
Fig. 1
Mean values of the Korean version of FAQL-PB for each of 17 items.
FAQL-PB = Food Allergy Quality of Life-Parental Burden.
![]()
Fig. 2
Correlation between parental burden and psychosocial factors in parents of children with IgE-mediated food allergies. (A) Bubble plot representation of psychological instruments. The darker bubble color represents higher anxiety scores (ranged 0 to 44), and bubble sizes are proportional to the depression score (ranged 0 to 27). (B) Spearman correlation matrix for parental burden, anxiety, depression, and resilience (all P < 0.001).
IgE = immunoglobulin E, FAQL-PB = Food Allergy Quality of Life-Parental Burden, BAI = Beck’s Anxiety Inventory, CD-RISC = Connor-Davidson Resilience scale, PHQ-9 = Patient Health Qustionnaire-9.
![]()
Table 2
Characteristics of patients (N = 190)
![]()
Factor analysis of FAQL-PB
The Kaiser-Meyer-Olkin value was 0.945, indicating adequate sample homogeneity. Two factors were extracted based on eigenvalue of greater than 1 and inspection of scree plot and two factors account for 93.61% variance of the FAQL-PB total variance. Item 1 to 3 had factor loading of more than 0.4 for factor 1, and otherwise item had factor loadings more than 0.4 (Supplementary Table 1). Factor 1 was labeled as limitation of life and factor 2 as emotional stress.
Validation and reliability of FAQL-PB
All items had good to excellent reliability (Cronbach’s α coefficients > 0.8). The percentage with the highest score was 0.5% (ceiling effect), and there were no participants with the lowest score (floor effect). The intra-class correlation value for test-retest reliability was 0.716 (P = 0.029), indicating good reproducibility. The FAQL-PB scores showed excellent correlation with FAIM-PF scores (r = 0.765, P < 0.001), while the FAQL-PB scores were negatively associated with the total CHQ-PF scores (r = −0.172, P = 0.017) (Table 3).

Table 3
Concurrent validity of FAQL-PB
FAQL-PF = Food Allergy Quality of Life-Parental Burden, HRQLQ = health-related quality of life questionnaire, CHQ-PF28 = Child Health Questionnaire-Parents Form 28, FAIM-PF = Food Allergy Independent Measure-Parent Form, FA = food allergy, QoL = quality of life.
*P < 0.05, **P < 0.001.
![]()
The total FAQL-PB scores were higher in the parents of children who had experienced anaphylaxis than in those who had not (P = 0.008) (Table 4). Higher scores of limitations of life and emotional stress domain scores, sub-scales of the FAQL-PB, were also observed in parents of patients with anaphylaxis than in those without anaphylaxis (P < 0.001 and P = 0.032, respectively).

Table 4
FAQL-PB scores by experience of anaphylaxis
| FAQL-PB scores | Anaphylaxis (n = 118) | No anaphylaxis (n = 72) | P value | |
|---|---|---|---|---|
| Total | 4.5 ± 1.2 | 4.0 ± 1.3 | 0.008 | |
| Limitation of life | 4.9 ± 1.1 | 4.2 ± 1.3 | < 0.001 | |
| Emotion stress | 4.0 ± 1.3 | 3.8 ± 1.4 | 0.032 | |
Scores represent the mean ± standard deviation of the sum of items ranging from 1 to 7.
FAQL-PB = Food Allergy Quality of Life-Parental Burden.
![]()
Factors associated with parental burden of children with FA
The FAQL-PB score was higher in the parents of children who avoided CM or soybean than in the parents of those who did not (P = 0.003 and P = 0.018, respectively) (Fig. 3). However, there were no differences in FAQL-PB scores between caregivers of children who restricted egg whites, wheat, peanuts, tree nuts, or crustaceans and those who did not. Univariable analysis showed that CM allergy (coefficient, 9.47; 95% CI, 3.31 to 15.64) and soybean allergy (coefficient, 14.86; 95% CI, 2.6 to 27.13) were significantly associated with higher FAQL-PB scores. There was no significant association of FAQL-PB with children’s age (coefficient, −0.05; 95% CI, −0.11 to 0.01), comorbidities of allergic diseases or delayed milestone (coefficient, 0.35; 95% CI, −0.32 to 1.03), the number of food allergens (coefficient, 0.05; 95% CI, −0.08 to 0.17), presence of siblings (coefficient, 0.1; 95% CI, −0.50 to 0.71) and carriage of epinephrine autoinjectors (coefficient, −0.09; 95% CI, −0.62 to 0.43). After adjusting for sex, age, and underlying diseases which showed P values < 0.1 in the univariable analysis, in the multivariable analysis, experience of anaphylaxis (coefficient, 9.32; 95% CI, 2.97 to 15.68), CM allergy (coefficient, 8.24; 95% CI, 2.04 to 14.44), soybean allergy (coefficient, 13.91; 95% CI, 1.62 to 26.20), higher anxiety (coefficient, 1.05; 95% CI, 0.07 to 1.41), higher depression (coefficient, 2.15; 95% CI, 1.61 to 2.69), and lower resilience (coefficient, −0.42; 95% CI, −0.64 to −0.20) were significantly associated with greater parental burden in parents of children with IgE-mediated FAs (Table 5).
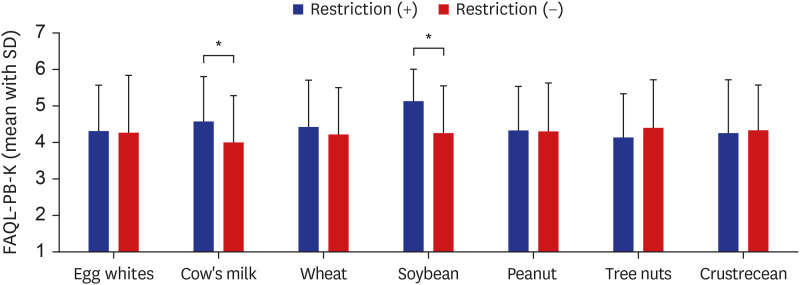
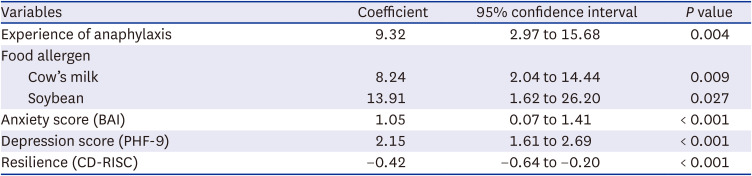
Fig. 3
The comparison of mean (SD) scores of FAQL-PB by restricted foods. The parental burden of caring for children with cow’s milk and soybean allergies was significantly higher than caring for those without these allergies.
SD = standard deviation, FAQL-PB = Food Allergy Quality of Life-Parental Burden.
*P < 0.05.
![]()
Table 5
Multivariable regression analysis of factors associated with FAQL-PB
Adjusted for age, sex, and underlying diseases (co-allergic diseases and delayed milestones).
FAQL-PB = Food Allergy Quality of Life-Parental Burden, BAI = Beck Anxiety Inventory, PHQ-9 = Patient Health Qustionnaire-9, CD-RISC = Connor-Davidson Resilience scale.
![]()
DISCUSSION
To the best of our knowledge, this is the first study to validate the Korean version of the FAQL-PB and investigate the risk factors associated with a heavier parental burden in Korea. We found excellent constructive validity, good internal consistency, and strong test-retest reliability for the FAQL-PB in assessing the parental burden of pediatric FA patients. The FAQL-PB showed no floor or ceiling effects. We also found that higher parental burden was associated with experience of anaphylaxis; CM or soybean allergies; and parental psychological distress, such as higher levels of anxiety and depression with lower resilience. This study provides a better understanding of the psychological burden and related factors in caregivers of Korean children with IgE-mediated FAs.
Recognizing the psychosocial impact of children’s FAs on families is crucial for developing FA management plans and supporting parents of FA patients, especially in countries with a high parental burden of raising children and low fertility rates.26 It is necessary to identify the factors that affect the burden of parents of children with FA through a relevant and valid measurement, as the burden of raising children varies depending on social background and culture.27
The FAQL-PB score with mean value of 4.3 in the present study was similar to the mean values of 2.1–4.3 in previous studies conducted in other countries.12 In accordance with previous studies, the highest burden was shown in social activity limitation rather than emotional stress.12 Korean parents of children with FAs gave the highest scores to social activity limitation for participating in social activities, while the highest scores were placed on difficulties in choice of restaurants in the USA and UK.1517 This might be due to the relatively low social awareness of FA and the consequent lack of consideration for children with FAs in communities and during social activities.
Unsurprisingly, a history of anaphylaxis in children was significantly associated with impaired parental QoL in the current study. These results are consistent with those of previous studies using the FAQL-PB.15282930 Anaphylaxis can occur in unpredictable circumstances and is often accompanied by severe systemic symptoms, which have a negative impact on parental burden and serious psychological stress in caregivers.31 Therefore, social attention and support from public policy are necessary to reduce parental burden in families of children with anaphylaxis.
Our observation that parents of children with allergies to soybeans or CM are likely to have worse QoL could be associated with dietary patterns and food ubiquity. CM allergy is known to be the most important food allergen affecting QoL in FA patients and their families. This is because dairy products are commonly consumed as meals and snacks due to them being a good source of calcium and energy in young children.32 Recent studies have shown that children with CM allergy have the greatest burden compared to other FAs because avoidance of CM is associated with serious social limitations, severe anxiety, and greater economic burden.33 A study of 876 families of children with FAs reported that parents of children with CM or egg allergies had a higher burden score on the FAQL-PB than those of children with peanut or tree nut allergies.29 Meanwhile, poor parental QoL associated with soybean avoidance in our results may be culturally specific and provide insight into the perceived burden of FAs in Asian populations. Frequent intake of soybean is unique to traditional Asian cuisines, which is different from Western food culture.34 In addition, many Korean dishes for children use soy sauce, soybean oil, and soybean paste, as well as tofu, soy milk, and soybeans because children cannot consume spicy sauce-food.35 In the analysis using machine learning on a validated dataset consisting of 3,238 menus and 3,036 ingredients for Korean children, soybean-free menus were found in 21.3%, while 78.4% of the menus did not include eggs.36
Our study also supports a previous investigation that health-related burden for caregivers of children with FAs was significantly associated with psychological distress such as anxiety and depression.3738 Furthermore, the mean BAI score indicating anxiety was 7.2 for parents in the present study, which is higher than a score of 4.3 in the general population in Korea.39 Similarly, a UK study of caregivers of children with peanut allergy reported that their anxiety and depression scores were significantly higher than those of the general population in the UK.10 Approximately 13.2% and 15.3% of parents in the present study showed moderate-to severe levels of anxiety and depressive symptoms, indicating needs for psychological counseling. This can be associated with parents’ daily difficulties in caring for children with FA, including managing uncertainty related to accidental exposures, advocating for their child across systems, and maintaining treatment tasks such as epinephrine autoinjector use and oral immunotherapy.40 Importantly, all of our psychological stress domains were inversely associated with resilience, which is the ability to maintain a positive developmental trajectory in the face of adversity.254041 These findings suggest that building resilience may be important to be better positioned to maintain a good parental QoL in caring for children with FAs. Resilience factors include education regarding problem solving, self-efficacy, enhancing social support, and meaning-making.4042
Caution is needed to generalize our research findings, because the present study was conducted in tertiary hospitals. Approximately 60% of subjects experienced anaphylaxis and more than half of patients restricted 3 or more foods. Although these characteristics of the study population have the possibility of bias in the results of the current study, the parental burden was not compared with healthy controls or those with less severe symptoms. Another limitation is that the CHQ-PF28, which was used for concurrent validation, evaluated general health perceptions as well as parental burden. However, this issue is not limited to the present study, as the original version of the FAQL-PB was also compared with CHQ-PF28 for the validation.13 Despite these limitations, this study is clinically meaningful in that these validated tools can be used to assess the parental burden after treatment options or social support to alleviate the burden in caregivers of pediatric FA patients.
In conclusion, the FAQL-PB is a reliable and valid tool for assessing parental QoL in parents of Korean children with FAs. Experience of anaphylaxis, CM or soybean allergies, increased anxiety and depression symptoms, and lower resilience were associated with poorer QoL in the parents of children with FAs. Therefore, pediatric allergists should assess the risk factors of poor QoL in caregivers of patients with FAs and develop psychosocial interventions and resilience enhancement strategies for them. Our data will be helpful in raising awareness of the seriousness of FA management in Korea.
 XML Download
XML Download