

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The novel coronavirus disease 2019 (COVID-19) started in Wuhan, China in December 2019, and rapidly spread around the world.1 In Korea, the first outbreak occurred in February 2019 around Daegu city.234 Although vaccines were developed and many people were vaccinated, the number of infected patients continues and variants of COVID-19 are spreading within global populations.56 Chest radiography is the simplest, easiest, and most accessible method to assess the presence of pneumonia and monitor the disease course in COVID-19 patients.78 To efficiently utilize the medical system, it would be best to use chest imaging at the appropriate time and for patients who need it.79 The Fleischner Society established consensus guidelines for the use of chest imaging for COVID-19 patients.9 According to the guidelines, chest imaging is not indicated for asymptomatic or mildly symptomatic patients unless they are at risk of disease progression (age > 65 years and presence of comorbidities).9 Chest imaging is indicated for patients with moderate to severe features such as hypoxemia or dyspnea and for COVID-19 patients with evidence of worsening respiratory symptoms. A recent study from Singapore revealed that screening chest radiograph in young and middle-aged adults with asymptomatic and minimally symptomatic COVID-19 is not indicated because more than 98% had normal chest radiographs.10 However, their study population was restricted to only young asymptomatic patients; therefore, the clinical utility of chest radiograph in the patients recommended to undergo chest radiograph was not fully evaluated.
In our hospital, chest radiographs were taken for all COVID-19 patients at the time of admission and during hospitalization regardless of their symptoms and risk factors. Therefore, we were able to investigate the prevalence of pneumonia and the adverse outcomes by dividing groups according to symptoms and risk factors of patients and assess the suitability of the Fleischner society imaging guidelines in evaluating chest radiographs of COVID-19 patients.
METHODS
Patients
Our institution was designated as a cohort hospital for admitting patients with COVID-19. In total, 822 patients who were diagnosed with COVID-19 using real-time reverse transcriptase-polymerase chain reaction of sputum or nasal secretions in screening clinics were consecutively admitted to the hospital from 21st February 2020 to 17th May 2020.
This was during the first outbreak of COVID-19 in South Korea, so there were no established admission criteria. Therefore, all the diagnosed patients had to be hospitalized regardless of their symptoms or risk factors.
Among them, 33 patients under the age of 19, 101 patients who had been previously quarantined at isolation facilities or transferred from other hospitals, and 3 patients whose symptoms were unspecific because of severe communication difficulties or missing data were excluded. Therefore, a total of 685 patients (204 men, 481 women; 58 ± 17.9 years) were finally included in this study. Among 685 patients, 236 patients overlapped with our previous study.8
Clinical data extraction
Patient’s demographic data, presence of comorbidities (hypertension, diabetes, hyperlipidemia, chronic lung disease, cardiovascular disease, neurovascular disease, chronic liver disease, chronic kidney disease, and malignancy), symptom types, severity of symptoms, symptom onset dates, initial peripheral oxygen saturation, and initial laboratory findings were reviewed and collected. Adverse outcomes included severe pneumonia, intensive care unit (ICU) admission, and death. The World Health Organization (WHO) criteria (fever or suspected respiratory infection plus one of the following: respiratory rate > 30 breaths/min, severe respiratory distress, or peripheral oxygen saturation ≤ 90% on room air) were used to define severe pneumonia.11 We also investigated whether the symptoms had developed during the hospitalization period among initially asymptomatic patients.
Patient groups according to the Fleischner Society Guidelines
Radiologists and dedicated clinicians classified the patients into 4 groups according to the initial symptom severity and presence of risk factors for disease progression according to the Fleischner guidelines. Mild symptoms were defined when there was no evidence of significant pulmonary dysfunction or damage (absence of hypoxia, no dyspnea). Moderate to severe symptoms were defined when there was evidence of significant pulmonary dysfunction or damage (hypoxemia, presence of dyspnea). The definition of “risk factor for disease progression” was age > 65 years, and having comorbidities as mentioned above.9
Group 1 included asymptomatic COVID-19 patients. Group 2 included mildly symptomatic COVID-19 patients without risk factors for disease progression. Group 3 included COVID-19 patients with mild symptoms and a risk factor for disease progression. Group 4 included COVID-19 patients with moderate to severe symptoms. According to the Fleischner Society guidelines, chest imaging is not indicated for groups 1 and 2, but is indicated for groups 3 and 4.9 We compared the prevalence of pneumonia, pneumonia score, and adverse outcomes between groups.
Chest radiograph
In the hospital where our COVID-19 cohort was treated, all premises were designated as a contaminated isolation zone. Therefore, all medical staff wore personal protective equipment to enter the hospital. Radiographers also wore personal protective equipment and acquired chest radiographs. A digital radiography (INNOVISION, DK Medical systems) system was used and most chest radiographs were performed with the patient in the erect position (posterior-anterior projection) except when the patient could not stand. All patients underwent initial chest radiography on the day or the next day of admission. Follow-up chest radiographs were taken every two or three days until discharge.
Chest radiograph scoring
We scored the chest radiographs at the time of admission, at the time of highest symptom severity during hospitalization, and before discharge. In the case of patients with negative chest radiographs at the time of admission, and for those who newly developed pneumonia after a few days, we also scored chest radiographs at the time they were newly seen. We used the Brixia scoring system, which is designed exclusively for semi-quantitative assessment of lung disease in COVID-19, ranking the pulmonary involvement on an 18-point severity scale according to the extent and characteristics of lung abnormalities.12 The radiograph fields were divided into six zones: upper, middle, and lower lung zones on each side. Then, the lung abnormalities in each zone were scored from 0 to 3 as follows: score 0: no lung abnormalities, score 1: interstitial infiltrates, score 2: interstitial and alveolar infiltrates (interstitial predominance), and score 3: interstitial and alveolar infiltrates (alveolar predominance). The scores of the six lung zones were then added, with scores ranging from 0 to 18.12 We did not score the opacity caused by other underlying lung diseases that are not related to COVID-19, such as tuberculosis, lung cancer, post-operative changes, metastasis, or atelectasis. Initial chest radiograph images were independently reviewed by two radiologists (blinded to the clinical information) and inter-observer agreement was assessed. Follow-up and last chest radiograph scores were assessed by a single radiologist.
Statistical analysis
Categorical variables are presented as numbers with percentages, and continuous variables are presented as means and standard deviations. Differences between groups were analyzed using the χ2 or Fisher’s exact test for categorical variables and the independent Student’s t-test or the Mann-Whitney U test for continuous variables. Statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). P values < 0.05 were considered statistically significant.
RESULTS
Patient characteristics
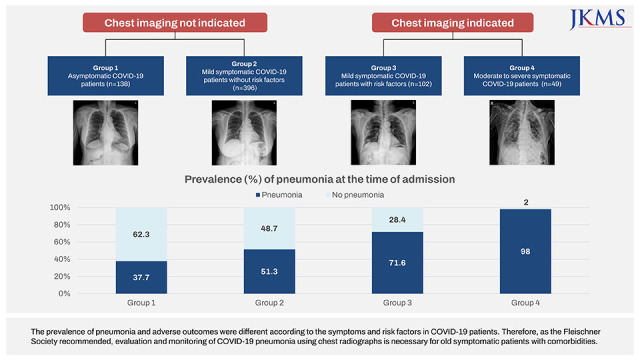
In total, 685 COVID-19-diagnosed patients were analyzed and there were 204 men (29.8%) and 481 women (70.2%), with a mean age of 58 ± 17.9 years. Among the 685 patients, 138 (20.1%) patients were initially asymptomatic (group 1), 396 (57.8%) patients had mild symptoms without risk factors (group 2), 102 (14.9%) patients had mild symptoms with risk factors (group 3), and 49 (7.1%) patients had moderate to severe symptoms (group 4) (Fig. 1). The clinical characteristics according to each group are summarized in Table 1. Age was significantly older in groups 3–4 than in groups 1–2 (P < 0.001), while it was not significantly different between groups 3 and 4 (P = 0.622). Comorbidities, such as hypertension, diabetes, hyperlipidemia, chronic lung disease, cardiovascular disease, neurovascular disease, and chronic liver disease, were significantly more frequent in groups 3-4 than in groups 1–2 (P < 0.05). White blood cell count, absolute neutrophil count, C-reactive protein, and lactate dehydrogenase levels were higher in groups 3–4 than in groups 1–2 (P < 0.001). Absolute lymphocyte count was significantly lower in groups 3–4 than in groups 1–2 (P < 0.001).
Fig. 1
Study population. According to the Fleischner Society guidelines, chest imaging is not indicated for groups 1 and 2, but is indicated for groups 3 and 4.
COVID-19 = coronavirus disease 2019, Risk factors = 65 years and comorbidities.

Table 1
Characteristics of patients according to the groups
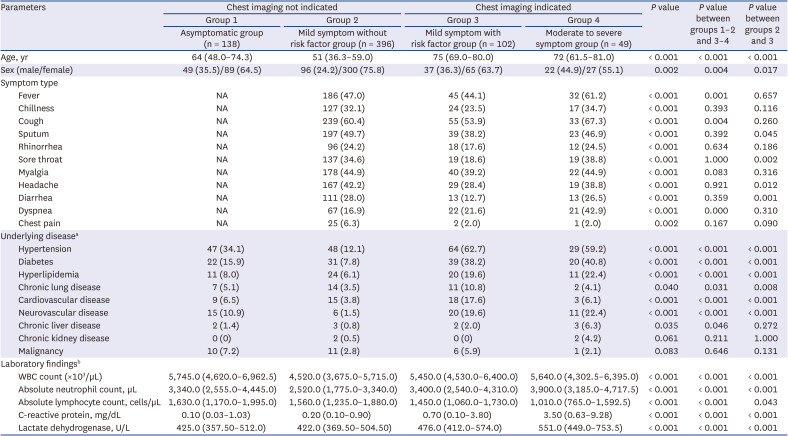
Data are presented as the number of patients (%) and median (25th–75th percentile).
WBC = white blood cells.
aAmong 685 patients, 1 patient was excluded due to an unknown underlying disease. bAmong 685 total patients, all laboratory results were not available in 2 patients, C-reactive protein and lactate dehydrogenase levels were not available in 1 patient, and lactate dehydrogenase level was not available in 2 patients.
Prevalence of pneumonia on chest radiographs according to the groups
The prevalence of pneumonia at the initial chest radiograph is summarized in Table 2 and Fig 2. On the initial chest radiograph at the time of admission, pneumonia was observed in 37.7% and 51.3% of patients in groups 1 and 2, respectively. Groups 3 and 4 showed pneumonia significantly more frequently (71.6% and 98%, respectively) on the initial chest radiographs than groups 1 and 2 (P < 0.001). In addition, groups 3 (median score: 4, 25th to 75th percentile, score: 2–7) and 4 (median score: 7, 25th to 75th percentile, score: 3–9) showed significantly higher pneumonia scores than group 1 (median score: 3, 25th to 75th percentile, score: 2–5) and 2 (median score: 3, 25th to 75th percentile, score 2–5) (P < 0.001) (Fig. 3). The maximum pneumonia score during the hospitalization period was also higher in groups 3–4 than in groups 1–2 (P < 0.001).
Table 2
Prevalence of pneumonia on chest radiographs according to the groups

Fig. 2
Prevalence of pneumonia at the time of admission. Group 1 = asymptomatic COVID-19 patients, Group 2 = mildly symptomatic COVID-19 patients without risk factors for disease progression (age > 65 years with comorbidities), Group 3 = COVID-19 patients with mild features and a risk factor for disease progression, and Group 4 = COVID-19 patients with moderate to severe features (hypoxemia and dyspnea).
COVID-19 = coronavirus disease 2019.
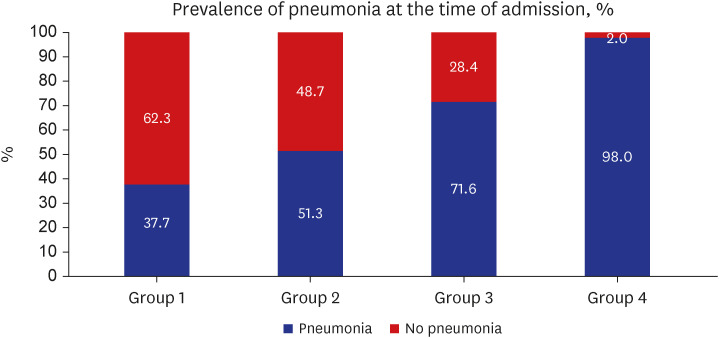
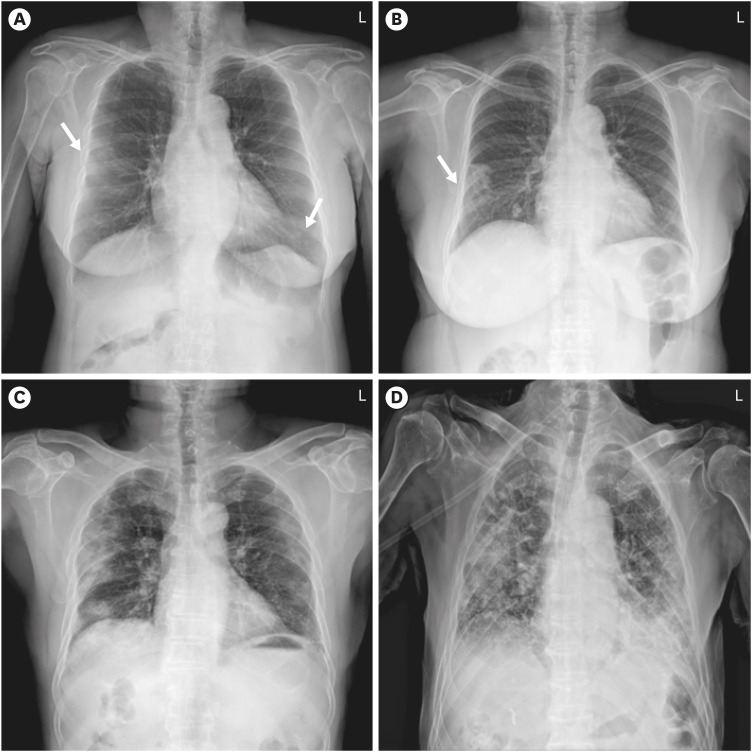
Fig. 3
Pneumonia at the time of admission according to the groups. All of these chest radiographs presenting coronavirus disease 2019 pneumonia were taken on the day of admission. (A) A 60-year-old female patient without any symptoms (Group 1). She had a history of hypertension. The chest radiograph shows focal increased parenchymal opacities (arrows) in the right middle lung field and left lower lung field. The chest radiograph score was 2. (B) A 68-year-old female patient with sore throat and myalgia. She was over 65 years old, but she had no underlying comorbidities (Group 2). The chest radiograph shows focal consolidations in the right middle and lower lung field, scoring 4. (C) A 69-year-old male patient with fever. He was over 65 years old and had hypertension and an old myocardial infarction (Group 3). The chest radiograph shows multifocal consolidations in both lungs, especially in the peripheral zone. The chest radiograph score was 9. (D) An 80-year-old male patient with fever. At the time of admission, he was on an O2 mask due to sudden hypoxemia (sat O2 < 80%) (Group 4). He had chronic lung disease, cardiovascular disease, and rheumatic disease. The chest radiograph shows diffuse consolidations involving all segments, scoring 11.
Clinical outcomes according to the groups
Adverse outcomes by group are summarized in Table 3. Adverse outcomes were significantly higher for imaging-indicated group 3 and 4 patients than for non-indicated group 1 and 2 patients. Progression to severe pneumonia (51%), admission to the ICU (34.7%), and death (14.3%) caused by COVID-19 were significantly higher in group 4 than in groups 1––3 (P < 0.001). The adverse outcome rate sharply increased in group 4. The prevalence rates of severe pneumonia and ICU admission were not significantly different between groups 2 and 3 (P > 0.05). Death was significantly more common in group 3 than in group 2 (P = 0.035).
Table 3
Prevalence of adverse outcomes on chest radiographs according to the groups

Adverse outcomes also occurred in groups 1 and 2, although their prevalence was lower than that in groups 3–4 (P < 0.001). In group 1, 8% (11/138) of patients had adverse events. All of these patients were asymptomatic at the time of admission, but symptoms developed a few days after admission. Most of these patients (9/11, 81.8%) had risk factors for disease progression (mean 80 ± 8.5 years, and 9 patients had comorbidities). In group 2, 3.5% (14/396) of patients had adverse events. Among them, 78.6% (11/14) of patients met one of the definitions of risk of progression (mean 57.5 ± 12 years, range 46–88 years, and 9 patients had comorbidities).
Group 1 – subgroup comparison
In group 1 of initially asymptomatic patients, 46.4% (64/138) of patients developed symptoms during follow up and 53.6% (74/138) of patients were asymptomatic until discharge. The clinical and radiographic findings between subgroups are summarized in Supplementary Table 1. Persistently asymptomatic patients were significantly younger than patients who developed symptoms subsequently. Among 74 persistently asymptomatic patients, 17 patients (23%) showed features of pneumonia on chest radiographs at the time of admission, which was a lower percentage than that for patients who developed symptoms subsequently (54.7%, P < 0.001). The initial and maximum pneumonia scores were not significantly different between groups (P > 0.05). All adverse outcomes only occurred in patients who developed symptoms subsequently and there were no adverse events in consistently asymptomatic COVID-19 patients. Among 64 patients who were initially asymptomatic but developed subsequent symptoms, 17.2% (11/64) progressed to severe pneumonia, 10.9% (7/64) were admitted to the ICU, 4.7% (3/64) needed mechanical ventilation, and 6.3% (4/64) died (Fig. 4). These 11 patients who progressed to adverse events were older (mean 80 ± 8.5 years, range 60–94 years) and most of them (9/11, 81.8%) had comorbidities.

DISCUSSION
In this study, the prevalence of pneumonia by chest radiographs was different according to the severity of symptoms and risk factors in COVID-19 patients, which supports the current Fleischner Society imaging guidelines. Patients with moderate to severe symptoms showed a high rate of pneumonia on chest radiographs and adverse outcomes than mildly symptomatic or asymptomatic patients. Therefore, evaluation and monitoring of the severity of pneumonia using imaging according to the current guidelines are essential. On the other hand, adverse outcomes did not occur in consistently asymptomatic patients, even though they showed pneumonia on chest radiographs. Therefore, imaging tests are not necessary for asymptomatic COVID-19 patients as recommended in the guidelines.9 However, among the initially asymptomatic patients, a considerable number of patients (46.4%, 64/138) developed symptoms after a few days, and 17.1% (11/64) of them had adverse outcomes. The patients who were initially asymptomatic but developed adverse outcomes were old and had comorbidities. Therefore, we should recognize that initially asymptomatic patients may be in the initial incubation period and need close follow-up, especially if they are old or have comorbidities.
In mildly symptomatic patients, the indication of chest imaging is based on the presence of risk factors in the current guidelines.913 The definition of risk factors in the guidelines is a combination of age > 65 years and presence of comorbidities.7 In this study, a small portion (3.5%) of patients with mild symptoms without risk factors (group 2) had adverse outcomes. These patients satisfied only one of the two definitions in the risk factors (i.e., close to 65 years of age and had comorbidities or were over 65 years of age but had no comorbidities). Although chest imaging is not indicated in patients who had only one risk factor, close monitoring is needed to detect disease progression at the discretion of the clinician. Although the Fleischner Society regards a combination of age > 65 years and presence of comorbidities as a risk factor for disease progression, the WHO guidelines considered one or more of age more than 60 years, pre-existing comorbidities, or immunosuppressive condition as risk factors for severe disease.11 Therefore, using chest imaging should be determined with the assessment of the risk for each individual by clinicians and their medical environments. In addition, the Fleischner Society recommends using imaging for patients when their symptoms progress during self-monitoring.9 This helps in the early detection of pneumonia, even in initially asymptomatic or mildly symptomatic patients as seen in our study.14
Chest imaging is indicated for patients with mild symptoms with risk factors (group 3) and patients with moderate to severe symptoms (group 4). Most of these patients showed pneumonia on initial chest radiographs (71.6% in group 3 and 98% in group 4), and they showed significantly higher rates of adverse events than patients who are not indicated for chest imaging. In addition, the levels of inflammatory laboratory markers, which were known as prognostic factors in COVID-19, were also significantly higher in these patients.15 Therefore, the current guidelines appropriately classify those who need imaging and close follow-up.
There were several limitations in this study. First, this study had a retrospective design and was conducted at a single hospital. Second, we only evaluated chest radiographs; therefore, the prevalence of pneumonia may be underestimated because of the low sensitivity of radiographs compared to chest computed tomography.
In conclusion, the incidence of pneumonia differs according to the patient’s symptom severity and presence of risk factors. Imaging analysis revealed that patients who had moderate to severe symptoms or mild symptoms with risk factors showed more frequent rates of pneumonia and adverse events. In the persistently asymptomatic group, imaging is not useful as no adverse events occur even if pneumonia is observed. However, old patients with comorbidities may progress to have adverse events even if they are initially asymptomatic or mildly symptomatic. Therefore, as the Fleischner Society recommended, it is necessary to use chest radiographs to evaluate and monitor pneumonia in old symptomatic COVID-19 patients with comorbidities.
 XML Download
XML Download