

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Myopia has emerged as a public concern during the last decades in East Asia, where the prevalence of myopia is higher than other regions in the world.12 Due to coronavirus disease 2019, that trend is now being exacerbated with a growing speed of myopia progression,34 which eventually results in more people having pathologic myopia (usually occurs in patients with high myopia, diopters ≤ −6.0). Myopic choroidal neovascularization (mCNV), a vision-threatening complications of pathologic myopia which might lead to irreversible macular atrophy or fibrosis after 5 years of onset,567 ranked the first in the most common cause of choroidal neovascularization (CNV) in less-than-50-year-old working age group.89 Historically, the treatment had been restricted to photodynamic therapy (PDT) for subfoveal mCNV and laser photocoagulation for extra or juxtafoveal mCNV. However, anti-vascular endothelial growth factor (VEGF) drugs significantly improve the visual outcome in patients with mCNV,10 so that the anti-VEGF drugs became the first-line option for mCNV treatment since 200911 and following pivotal studies, the RADIANCE12 and MYRROR13 studies, confirmed the era of anti-VEGF drugs in treatment of mCNV. Howerver, as virtually nothing is known about these shifting in real-world practice; some lacked switching patterns among treatment options1415161718 and others did not take account for all treatment options including non-reimbursement treatment choices and off-label drugs.1618 Similar to other countries, the Korean National Health Insurance Scheme (NHIS) had not covered any anti-VEGF drugs until 2016, and therefore, the claims database from the NHIS is not suitable for research regarding the mCNV unlike exudative age-related macular degeneration (AMD),19 which NHIS have covered these treatments since 2007.
The Observational Health Data Sciences and Informatics (OHDSI), which is a global consortium established to accelerate observational data research, has introduced the Observational Medical Outcomes Partnership (OMOP)-Common Data Model (CDM).20 The OMOP-CDM provides a comprehensive ability to capture data in the same manner across places which enhance scalability of studies and to analyze data in a rigorous way which enables reproducible research. Studies using CDM have raised an academic attention in several fields of medicine as the CDM could generate the real-world evidence.21 Recently, studies in ophthalmology have been conducted using the data from the OMOP CDM to analyze the real-world incidence of endophthalmitis following anti-VEGF drugs22 and the real-world treatment intensities and pathways of macular edema following retinal vein occlusion (RVO).23 Unlike some diseases that need intensive chart review in addition to operational definition to confirm the accuracy of diagnosis,24 mCNV could be investigated using OMOP CDM. Therefore, in this research, we aimed at characterizing the treatment intensity and patterns in patients with mCNV.
METHODS
Data source and eligible criteria for study population
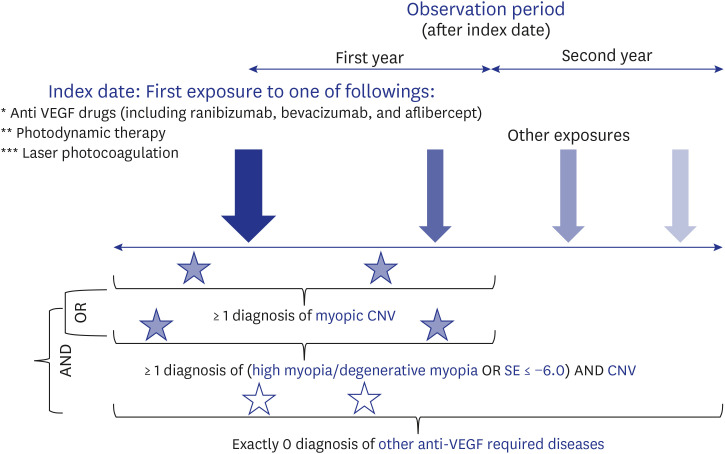
This was a retrospective, observational study using the OMOP CDM database (version 5.3.1) in Seoul National University Bundang Hospital (SNUBH), which included a number of 2,006,478 patients (47.6% female) from April 2003 to December 2020. For the analysis, we created a treatment-naïve mCNV cohort consisted of patients who exposed to any of three anti-VEGF drugs (ranibizumab, aflibercept, and bevacizumab) or any of two procedures (laser photocoagulation and PDT). The index date was defined as the date of the first exposure to these drugs or procedures. Of these, we included patients who had at least 365 days before the index date for wash-out period to ensure treatment-naïve profiles and had at least 365 days after the index date to observe the subsequent prescriptions.17 The end date of the cohort was the end of observation in each patient or the end of database at December 31, 2020. Then, we identified mCNV patients who had 1) the diagnosis for mCNV or 2) the diagnosis for CNV along with high myopia defined by the diagnosis of high myopia, degenerative myopia, or pathologic myopia or by the measurement of refractive errors (spherical equivalent ≤ −6.0 diopters)25 between 365 days before and after the index date. Lastly, we excluded all patients who had any other conditions which might require anti-VEGF drugs including exudative AMD, RVO, diabetic macular edema (DME), etc.26
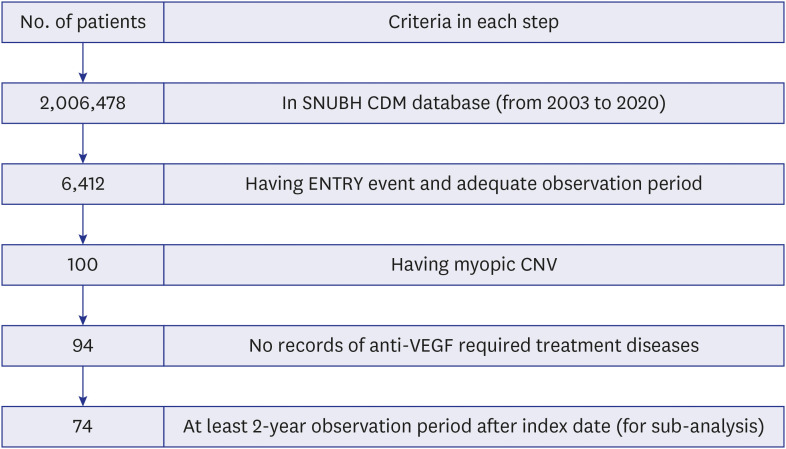
Fig. 1 depicts the Schematic diagram for definition of treatment naïve mCNV cohort, and Fig. 2 shows the Flow Chart for the eligible patients. Supplementary Table 1 provides standard concept codes used in the analyses.
Study outcomes, statistical analysis
We investigated the baseline characteristics of patients including age, gender, race, medical history, myopic status (measured in diopters). The visual acuity (presented in LogMAR) at baseline (index date) and the date of 90, 365, 730 days after the index date was also assessed; and the Generalized Estimating Equations (GEE) model was applied to treat these repeated measured visual acuities, considering the effect of drug types on the visual outcomes. Statistical significance was defined as P < 0.05. After that, we assessed the treatment intensity as follows. We first assessed the number of treatments in each patient, and also calculated the number of treatments in the first and second year after the index date. We stratified the results by calendar years and the three periods (the era of pre-anti-VEGF drug, from April 2003 to December 2005; the era of early anti-VEGF drugs, from January 2006 to November 2017; and the era of anti-VEGF drug reimbursement, from December 2017 to December 2020) based on the index date in each patient. We also confined the analysis to patients who completed at least 2 years of observation periods from the index date. In addition, we stratified the included patients according to their initial treatments. Lastly, among the patients having at least-2 year of observation periods, we assess the proportion of patients who did not have any prescriptions in the second year after their index date. By using logistic regression via GEE, we also studied the effect of previously known prognostic factors - namely “age”,27 “visual acuity at baseline”27 and “type of drugs received”28, plus another “gender” factor - on the treatment demand at the second year after treatment initiation. The functions provided in ATLAS version 2.10.1 with modification the source code (using open-source R package) were used. We also used R Studio version 3.6.3 and PostgreSQL version 8.0.2 in the analyses.
RESULTS
We included a total of 94 patients with mCNV, and of these, 74 patients completed at least 2 years of follow-up from the index date (Fig. 2). A majority of patients aged from 50 years old above (67.38%), most were females (73.4%), and all patients were Korean. While the accompanied visual system disorders were high (87.23%), less than 5% having chronic diseases such as diabetes or hypertension as well as other cardiovascular diseases. The myopia status at baseline were −5.79 ± 5.04 diopter (Supplementary Table 2). The visual acuity (LogMAR) were 0.291 (at baseline), 0.243 (after 90 days), 0.237 (after 365 days), and 0.237 (after 730 days) (Supplementary Fig. 1); however, the improvement in visual acuity was not statistically significant (P = 0.203) (Supplementary Table 3), even when the type of initial drugs was taken into account (P > 0.05) (Supplementary Table 4).
Treatment intensity in patients with mCNV
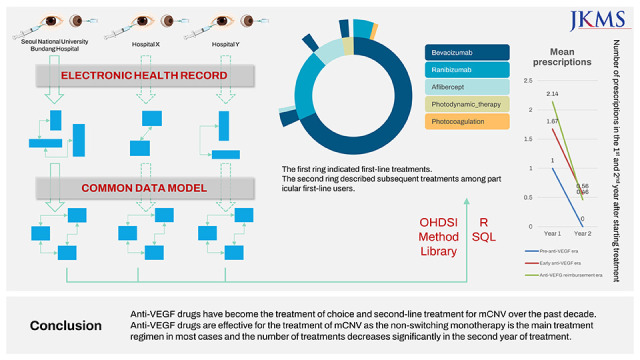
The number of treatments tended to increase over time, and bevacizumab was the most frequently selected treatment for mCNV throughout the study period (Supplementary Fig. 2). In the first era (2003–2005), only one patient was included and only one PDT was administered. The average number of treatments increased from 1.5 to 2.5 per patient per year in the second era (2006–2017) to 3 in the third era (2017–2020) (Supplementary Fig. 3). In each patient with mCNV, the number of treatments decreased dramatically in the second year of treatment in comparison with that of the first year from 2.09 to 0.47, and the trend was consistent irrespective of treatment modalities (Table 1). Similar trends were observed in those patients with at least 2-year observation period (Table 2). It was clearly seen that a large majority (77.03%) did not undergo any treatment in the second year (Supplementary Table 5). No significant prognostic factors of the treatment demand in the second year was found, except initial drug types with “Bevacizumab” (P = 0.003) and “Ranibizumab” (P = 0.009) (Supplementary Table 6). However, the number of patients in the reference category “Aflibercept” was very small and further studies are warranted.
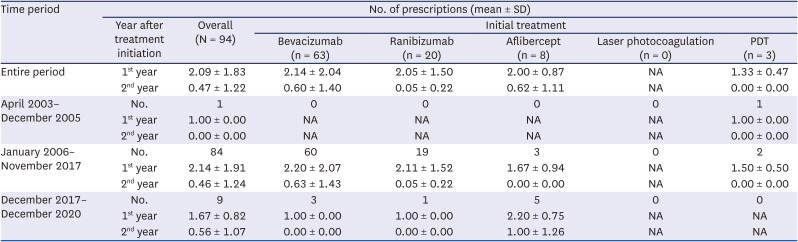
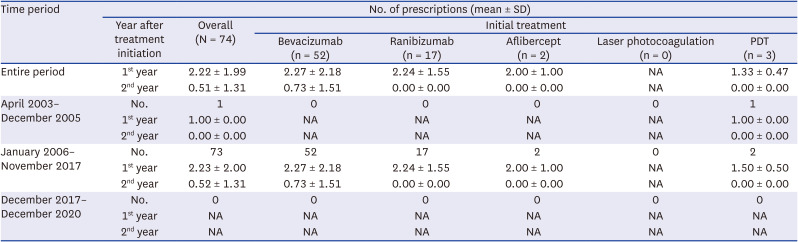
Table 1
Treatment intensity in the patients with myopic choroidal neovascularization throughout the study period (n = 94)
Patients were categorized into three different analysis periods based on their index date, and into different groups based on which therapies initiated first. The mean and the SD of prescriptions in the first year and in the second year after index date was calculated.
SD = standard deviation, PDT = photodynamic therapy, NA = not available.
![]()
Table 2
Treatment intensity in the patients with myopic choroidal neovascularization completing at-least 2 years of the observation period throughout the study period (n = 74)
Patients were categorized into three different analysis periods based on their index date, and into different groups based on which therapies initiated first. The average number of prescriptions in the first year and in the second year after index date was calculated.
SD = standard deviation, PDT = photodynamic therapy, NA = not available.
![]()
Treatment patterns in patients with mCNV
We identified 10 unique treatment patterns of patients with mCNV throughout the study period (Fig. 3A). A vast majority received anti-VEGF drugs as the initial treatment (96.8%) and the most prevalent first-line treatment for patients with mCNV belonged to bevacizumab (68.1%), whose figure was far higher than the second most popular, ranibizumab (20.2%). It was found that bevacizumab was still the most common choice of second-line anti-VEGF drugs among all patients with multitherapy regardless of their first-line treatment status, at 53.8%. Regarding the sub-analyses in the divided periods, in the period from April 2003 to December 2005, only one case of mCNV was detected. And the patient was initially treated with bevacizumab then switched to PDT (Fig. 3B). Bevacizumab first-line users accounted for 72.6% during the period from January 2006 to November 2017 (Fig. 3C). The period of December 2017 to December 2020 witnessed an absolute preference of anti-VEGF treatments without any session of laser photocoagulation nor PDT. The aflibercept took place of bevacizumab to be the dominant choice of first-line treatment (55.6% vs 33.3%) in this period (Fig. 3D).
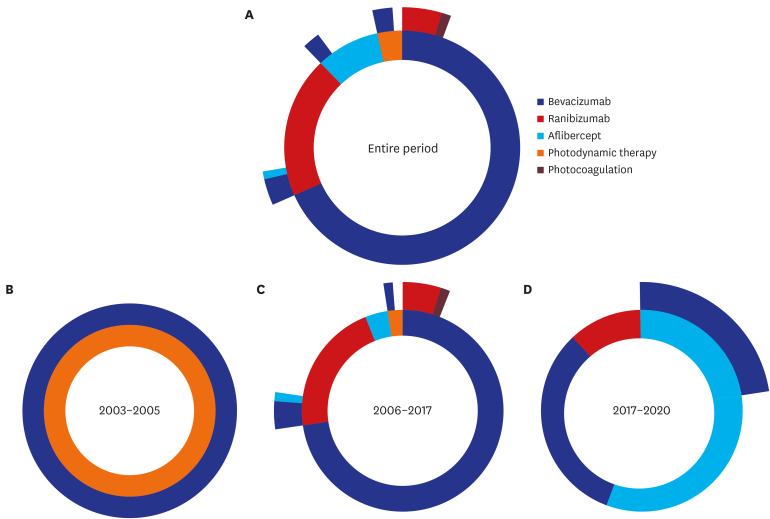
Fig. 3
Sunburst plots presenting the Treatment Pathways in patients with myopic choroidal neovascularization. First ring indicated the first-line treatment. The second ring described the subsequent treatments among those following the certain first line ones. Each period was plotted according to index date of each patient, subsequent treatment episodes were counted until the end of observation period (cohort exit date).
![]()
Loyal-to-one-treatment patients stood at a large percentage (86.2%) and the rest 13.8% opted for a switch to a second line. No cases received the third-line treatment. Of those patients who initiated their treatment with bevacizumab (68.1), large proportion (92.2%) did not need alternative therapy, as only a small number of patients switched to ranibizumab (6.25%) or PDT (1.5%). The similar patterns were observed in other therapies.
DISCUSSION
To the best of our knowledge, the present study is the first study describing the real-world treatment intensity and patterns in treatment-naïve mCNV patients using the OMOP CDM. The findings pointed out that patients with mCNV experienced one or two treatment modalities, and among over 60% of patients, bevacizumab was selected as the first line or in the second line treatments. The total number of prescriptions tended to increase year by year, which was consistent with current knowledge because anti-VEGF agents so far have been proving its efficiency and safety in the treatment of mCNV in the real world,293031 and they are also superior to other modalities demonstrated by two significant clinical trials (RADIANCE and BRILLIANCE).1232 In our study, the statistically insignificant improvement in visual acuity might be attributed to the incompleteness of visual acuity data. Before 2005, when anti-VEGFs were not introduced, extremely few patients were included in this study; mCNV patients were often not indicated for PDT or laser photocoagulation, so it is likely that most of them did not receive any treatment. When it comes to the number of included patients in the era of anti-VEGF drugs, the figures were disproportionate with 84 patients included in the period of 2006–2017 (12 years), compared to only 9 patients in the period of 2017–2020 (4 years). The backlog of patients waiting for the suitable treatment method might be a reasonable justification for this sudden surge in number of patients after introduction of anti-VEGF drugs.
With respect to the mean number of prescriptions, there was a remarkable decline between the first year and the second year in our study (from 2.09 to 0.47), suggesting that initial treatment might be adequate to deactivate the mCNV. It was in accordance with the established guideline of the prorenata treatment without loading phases regimen (one injection in the first episode and then as needed) in treating patients with mCNV,6 and the results from observational studies.1718 Two studies showed that the mean/median number of injections decreased from approximately three in the first year to just under 0.5 in the subsequent year, and other 12-month observation study treated with ranibizumab, more than half (52.2%) of patients received just one injection in the study period and about 90% of patients took less than three injections.16 No prognostic factors were found regarding the 2nd year treatment demand, raising the need for further studies on this matter. In addition, it is important to compare the number of prescriptions needed in mCNV with other retina diseases that require anti-VEGF drugs, such as exudative AMD, DME, and RVO. In patients with exudative AMD and DME, it is usually necessary to have loading doses (at least 3 injections) since diagnosis.3334 On the other hand, patients with mCNV tend to receive less frequent injections thanks to the omission of loading doses.6 In a CDM-based real world study examining the treatment intensities of macular edema following RVO, the mean number of injections in the first year of treatment was from 2.45 to 3.12 (depending on the era),23 which is approximately one injection higher than our results. In addition, the findings from the present study is quite similar to those from the two landmark trials, the RADIANCE12 and MYRROR.13 Interestingly, there was a decrease in the mean number of injections in the first year of treatment between the 2nd era and 3rd era. It might be the results of the increasing use of aflibercept which might have probable superiority in mCNV treatment: aflibercept is superior to ranibizumab in terms of better final visual outcomes,35 and to bevacizumab in terms of less treatment intensity during 12-month period.36
In our study, bevacizumab was indicated to be the most frequently applied treatment for mCNV both in first and second line of treatment, which has an affordable price as well as non-inferior efficacy compared to ranibizumab in the mCNV treatment.37 It allows individualized and sufficient treatments without any restriction from the NHIS in Korea, and therefore, physicians prefer bevacizumab in case of patients who require repetitive treatments or who do not meet reimbursement criteria. Most of the included patients (86.2%) were sufficient for non-switching monotherapy, which revealed the effectiveness of anti-VEGF drugs in treatment of mCNV, especially in comparison with other diseases treated with anti-VEGF drugs.3038 The drugs conversion, whose literature has been still in its infancy, has been well described in our study.
Our study obviously has certain limitations. First, pristinely-mapped CDM may result in some information biases. For example, the disease laterality (left or right eye) was frequently neglected; however, the fellow eye does not always share the same problem with the affected eye. In addition, the incompleteness of visual acuity mapping refrain us to answer the question whether under-treatment may drive the underestimation of treatment intensity as there was an association between poor outcomes and less-than-needed treatment frequency.39 Third, the lost-to-follow-up issue could lead to the ignorance of mCNV relapse events (though recurrence episodes occurs mostly within first year in treatment naïve patients40), meaning ignoring additional injections in those patients. Forth, although one year of wash-out period is sufficiently long to ensure the treatment-naïve profile, it may be still biased by the inability of our database to capture patient’s history of treatment across other healthcare facilities. Finally, this study had the drawbacks of inadequate heterogeneity due to single center sampling, leading to the limited generalization of the findings.
Despite those limitations, our study had strengths that are unique in addressing our research question. First, our study is among pioneers in terms of visualizing the pathways of mCNV treatment, including a switch of drugs and procedures in different eras of 18-year period. Second, using CDM results in a much less time-consuming, labor-intensive and human error-prone process in dealing with real-world data. CDM allows the very flexible searching, dealing with the queries, and extending to multiple CDM databases.20 Also, concepts, cohorts, and analysis in a CDM-based study could be reused later in each single step of another research. Third, our advantage of using electronic medical record compared with claim data is that we can assess off-label use and non-reimbursement options.
In conclusion, there has been a shift to anti-VEGF drugs as a treatment of choice in mCNV over the last decades, both first and second-line treatment. Anti-VEGF drugs have also proved their effectiveness in real-world settings: non-switching prorenata monotherapy is the main treatment regimen in most cases and there is a sharp decrease in treatment intensity from the second year of treatment.
 XML Download
XML Download