

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Identifying reinfection or reactivation of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) cases is challenging even though deep sequencing and viral kinetics of SARS-CoV-2 have been unveiled since December 2019. Reinfection cases after a few months have been reported in young and immunocompetent patients.123 Prolonged viral shedding was noted in patients with severe immunosuppression, such as patients with a hematologic malignancy undergoing anti-cancer therapy or acquired immune deficiency syndrome.45 In addition, within-host genomic evolution of SARS-CoV-2 has been discovered in some immunocompromised patients,678 which raised a concern for treatment and emergence of new variants. In this study, we report a patient who underwent rituximab and bendamustine chemotherapy for the treatment of follicular lymphoma, followed by steroids for drug-induced interstitial lung disease. She harbored SARS-CoV-2 for over 2 months, which was reactivated with genetic variation, but she recovered successfully after receiving passive antibodies.
CASE DESCRIPTION
A 48-year-old woman diagnosed with follicular lymphoma first underwent chemotherapy with rituximab and bendamustine on May 12th, 2020. One month after the chemotherapy, she developed dyspnea and her chest computed tomography (CT) showed multi-focal ground-glass opacities suspicious for drug-induced interstitial lung disease (Fig. 1A). She started high-dose steroid therapy, followed by being discharged on 30 mg oral prednisolone along with minimal home oxygen supply. However, three days later, she was tested for SARS-CoV-2 reverse transcription polymerase chain reaction (RT-PCR) under contact tracing on September 13th (day 0) and was found to test positive. She was readmitted for coronavirus disease 2019 (COVID-19) infection. She had mild fever and her oxygen demand increased from 2 L/min to 3 L/min on nasal cannula at first. However, since she was stable and the inflammatory markers decreased to normal during hospitalization, she did not receive anti-viral agents including remdesivir and was discharged on day 14. She then visited the out-patient clinic on November 10th and newly developed pneumonia was found on her chest X-ray film. A positive SARS-CoV-2 test with dyspnea, fever, and tachypnea was noted on November 20th (day 68); hence, she was admitted to the isolation ward. Chest CT showed peripheral and subpleural consolidation consistent with viral pneumonia (Fig. 1B). Six days later, her symptoms aggravated with increased oxygen demand from 3 L/min to 6 L/min on nasal cannula with sustained high fever. We assessed the patient’s lymphocyte counts and humoral immunity (Supplementary Tables 1 and 2). Peripheral B cell was 0%, IgG level was 400 mg/dL, and CD4 T-lymphocyte count was 55/μL (11.9%), indicating severe immunodeficiency. In this deteriorated condition, all pharmacologic therapies were initiated: high dose steroid, empirical antibiotics, COVID-19 convalescent plasma (CCP), and intravenous immunoglobulin (IVIG). The timeline of medical treatment and test results are described in Fig. 2 and serial chest X-ray films, cycle threshold (Ct) values of SARS-CoV-2 and clinical course including are presented in Supplementary Fig. 1. At the same time, Ct value of RT-PCR by Allplex 2019-nCoV Assay kit (Seegene, Seoul, Korea) collected from the nasopharyngeal specimens was reviewed and the samples were delivered to the laboratory of Korea Disease Control and Prevention Agency for virus culture and genomic analysis. In addition, blood samples were collected for the titer of antibodies against SARS-CoV-2 spike (S-) protein using the Elecsys immunoassay (Roche Diagnostics, Mannheim, Germany).
Fig. 1
Chest computed tomography scan of the immunocompromised patient at diagnosis of (A) drug-induced pneumonitis and (B) reactivation of severe acute respiratory syndrome coronavirus 2.
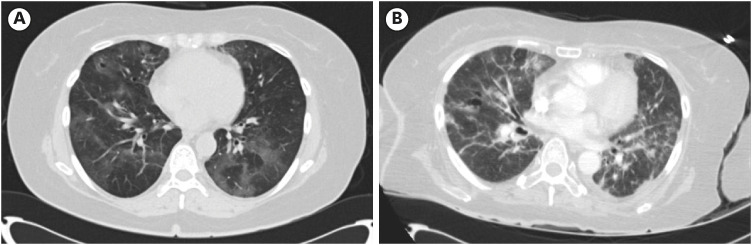
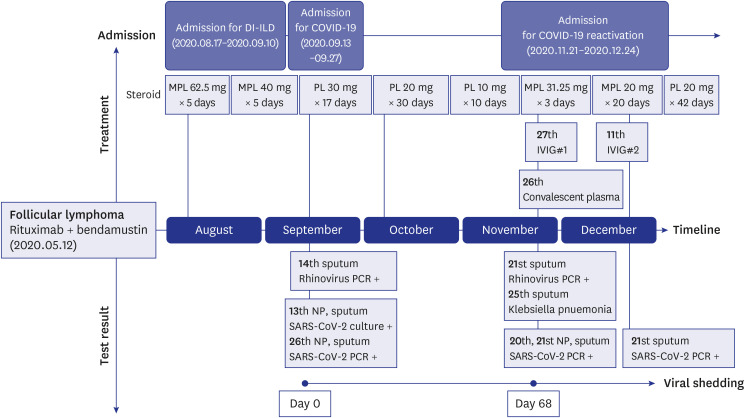
Fig. 2
Timeline of treatments and test results of the patient who underwent treatment for lymphoma, drug-induced pneumonitis, and COVID-19 infection.
DI-ILD = drug-induced interstitial lung disease, COVID-19 = coronavirus disease 2019, MPL = methylprednisolone, PL = prednisolone, IVIG = intravenous immunoglobulin, PCR = polymerase chain reaction, NP = nasopharyngeal, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
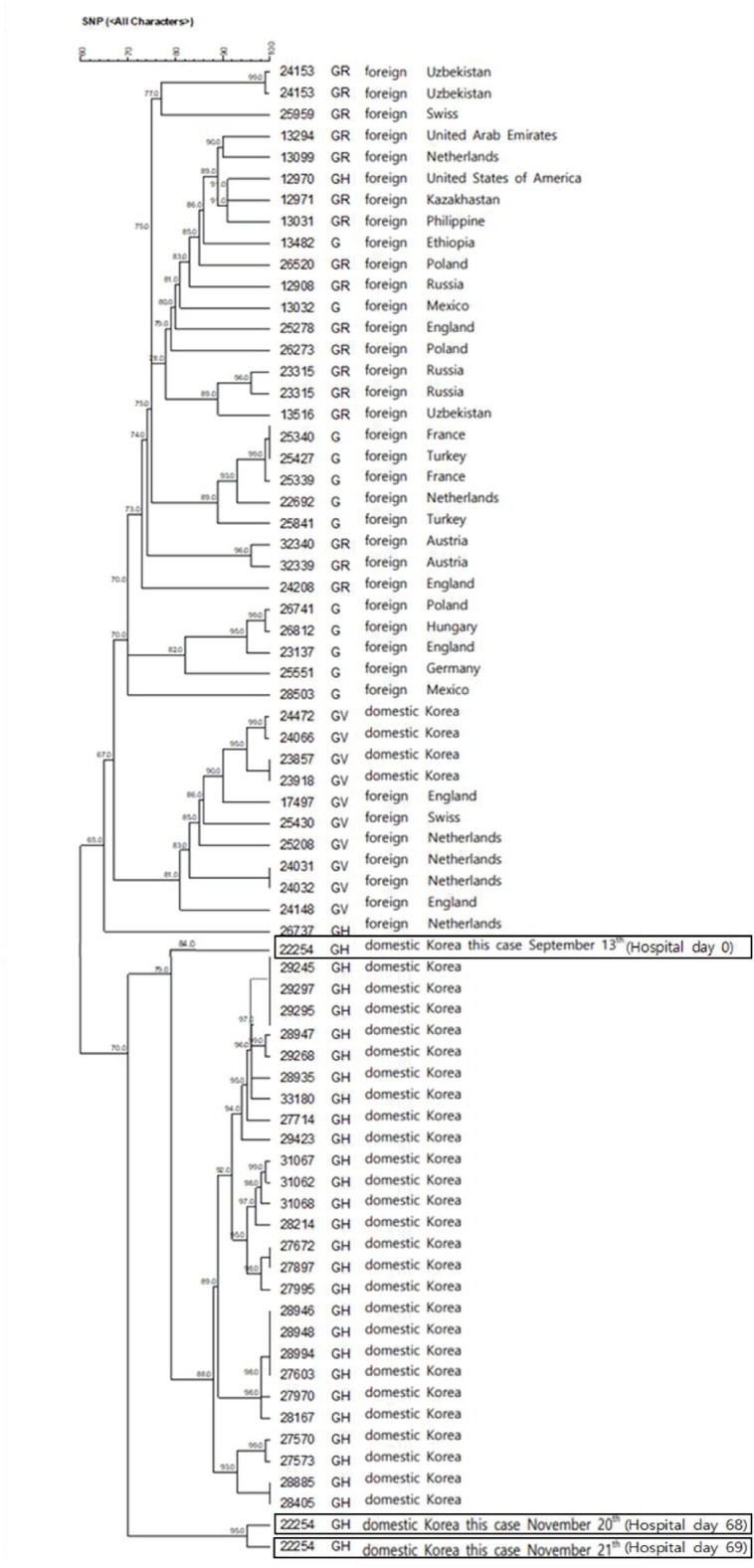
We administered CCP after 6 days of hospitalization. The donor of the CCP was 35-year-old male diagnosed with mild COVID-19 on August 28th, 2020. The plasma was collected on October 28th, 61 days after the diagnosis. The CCP had 238 U/mL of S-specific antibodies. Recipients were transfused 300 mL of CCP twice between 12 hours, but our patient had chills and chest discomfort after the first CCP; therefore, administration of second CCP was suspended. The patient’s antibody titer was < 0.04 U/mL, but after the transfusion the titer rose to 17.9 U/mL. The S-spike antibody titer decreased to 8.37 U/mL over time but it persisted for at least a week (Supplementary Fig. 2). She also received IVIG at a dose of 400 mg/kg and high dose steroid. After the treatment, her clinical course improved. The Ct value in nucleoprotein (N) gene for the initial infection was 28.1, while that for second episode was 18.6 (Supplementary Table 3). The Ct values increased after the treatment as symptoms relieved. Next Generation Sequencing analysis was performed on the nasopharyngeal specimens collected at day 0, day 68, and day 69 to confirm reinfection. All viruses were identified as GH-type by Global Initiative on Sharing All Influenza Data clade,9 which was the circulating virus type in Korea in late 2020, but the genome sequence of day 0 and day 68 revealed 18 different nucleotides, and the association of single nucleotide polymorphisms (SNPs) was 79%. The genome sequence of day 68 and day 69 was similar. The phylogenetic analysis of SARS-CoV-2 collected has been described in Fig. 3. She was successfully discharged to home on December 24th (day 103), and she has since been stable on room air in the outpatient clinic.
DISCUSSION
Rituximab, a monoclonal antibody against the CD20 antigen on B cells, compromises humoral immunity, and the prevalence of hypogammaglobulinemia is as high as 39–42.9% in lymphoma treatment cohorts.10 Bendamustine, an alkylating agent, could induce myelosuppression, preferentially inhibiting CD4+ lymphocyte.11 Besides, prolonged high-dose steroid administration induces reduction of T cells as well as B cells.12 Therefore, persistent hypogammaglobulinemia and lymphocyte depletion could affect the host vulnerability to prolonged viral infection. Severely immunocompromised patients who have impaired immunity for viral clearance were found to be susceptible to chronic infection of SARS-CoV-2 like other noted viruses.13 As the SNP association was over 5%, the patient was suspected to have reinfection at first.14 According to the Infectious Disease Control and Prevention Act, epidemiologic investigation was conducted through Epidemiologic Investigation Support System (EISS) and in-depth interviews.. EISS provided the tracking information of confirmed cases of COVID-19 based on credit card usage data and Cell Positioning System information,15 and it was confirmed that she stayed only at home and no other COVID-19 patients visited her house. Any history of contacting COVID-19 patients was not identified in the in-depth interviews. The family members of the case tested negative three times with SARS-CoV-2 RT-PCR. Since there were no epidemiological findings that implied the potential risk of reinfection, in-host viral evolution was been shown in this immunocompromised patient.
During late 2020 when our patient was treated, the effect of CCP therapy was equivocal. Many studies have revealed that CCP from donors after natural infection does not improve outcomes for patients with SARS-CoV-2.1617 However, there were case reports that symptoms improved notably after the therapy, particularly in patients with immunodeficiency.1819 In a cohort study of patients with hematologic malignancy, the survival benefit was proved after administering CCP.20 In a randomized clinical trial, sub-analysis showed that CCP demonstrated potential benefit for organ support-free days in participants with immunodeficiency at baseline.21 CCP was authorized for the treatment of COVID-19 in patients who have immunosuppressive disease or are receiving immunosuppressive treatment.22 Since patients with immunodeficiency were unable to elicit and obtain effective humoral responses, dose and timing of antibody-based treatment could be less critical and beneficial. Therefore, two passive antibodies which our patient received are assumed to promote viral clearance and clinical improvement.
The reason the reactivation was more severe than the first infection is unknown but potentially may be owing to higher viral load. Compared to the first nasopharyngeal sample, the Ct value of the second sample was low, indicating higher concentration of viral genetic material associated with infectivity and severity. Genome mutations which had no effect on viral fitness and immune escape variants were demonstrated within a transplanted patient, suggesting that immunocompromised individuals could be a trigger for the potential SARS-CoV-2 variants.23 An elevated within-host genomic diversity positively correlated with lower viral load over time and the direct transmission of the virus in healthcare settings was documented.24 Therefore, isolation for the reactivation of SARS-CoV-2 in severely immunocompromised patient should be considered.
In conclusion, a severely immunocompromised host who is susceptible to chronic infection of SARS-CoV-2 should be carefully monitored because of the risk of within-host evolution. To our knowledge, this is the first described case of prolonged viral shedding of SARS-CoV-2 in an immunocompromised patient due to within-host viral evolution which was verified by genomic analysis in Korea.
 XML Download
XML Download