

 PDF
PDF Citation
Citation Print
Print



INTRUDUCTION
Generally, a healthy person has trillions of gut microbes, the composition of which may be affected by numerous factors, such as diet, drugs, breastfeeding, stress, age, and so on [1]. The gut microbiota is important in maintaining optimal health [1]. One of the most important roles of the gut microbiota is to strengthen the host’s resistance to infection [2]. The gut microbiota not only excludes endogenous and exogenous pathogens, but also stimulates local immune cells, therefore, maintaining systemic immunity [2].
The composition of the gut microbiota can be changed after colorectal surgery due to several factors, such as stress and alteration of homeostasis, mechanical bowel preparation, use of antibiotics, exposure to oxygen, tissue ischemia, and so on [34]. As a result, the abundance and function of microbiota would decrease during admission [2], which could affect the outcomes of colorectal surgery. Previous studies reported that the incidence of postoperative complications, such as postoperative ileus, adhesions, surgical site infections, and anastomotic leakage, is affected by the gut microbiota [345]. Therefore, maintaining microbial homeostasis is extremely important during colorectal surgery.
A recent study reported that dietary pre-habilitation may alter the gut microbiota and improve the postoperative outcomes [6]. Several previous studies also reported that preoperative use of probiotics may help maintain a balanced gut microbiota and decrease the risk of postoperative infectious complications [78]. Theoretically, perioperative nutritional therapy can also influence the preservation of microbial homeostasis [9]. Preoperative immunonutrition may improve nutritional status, helping the patient recover from the surgical stress [10]. Many previous studies have reported that adequate nutritional treatment may reduce the mortality and morbidity of gastrointestinal surgery [1112]. However, a very few studies have reported the impact of preoperative immunonutrition on the composition of the gut microbiota. Previously, we conducted a randomized clinical trial (RCT), which aimed to assess the impact of preoperative immunonutrition on the incidence of postoperative infectious complications related to colon cancer surgery [10]. We also hypothesized that a change in the composition of the gut microbiota may be a possible mechanism of the association between immunonutrition and infectious complications.
Therefore, as a secondary analysis of a previously conducted RCT, the present study aimed to evaluate the effect of preoperative immunonutrition on the composition of fecal microbiota following a colon cancer surgery.
MATERIALS AND METHODS
The present study was a secondary analysis of an RCT aimed at assessing the impact of preoperative immunonutrition on the postoperative outcomes of colon cancer surgery [1013]. The study was approved by the Institutional Review Board (IRB) of Chonnam National University Hwasun Hospital (IRB No. CNUHH-2019-062). All enrolled patients were fully informed about the study protocol and signed an informed consent form. The study was performed according to CONSORT criteria and was registered with the Clinical Research Information Service (CRIS registration No. KCT0003770; https://cris.nih.go.kr/cris/search/detailSearch.do/15536). The detailed study protocol and the primary study outcomes have been previously published elsewhere [1013].
Participants and study design
Patients aged 20–80 yrs with primary colon cancer who were scheduled to undergo radical resection were screened and enrolled in this study. Those who underwent emergency surgery, with oral intake problems, who were pregnant, and were scheduled to undergo ostomy surgery were excluded. The patients were randomly assigned to either the experimental arm (immunonutrition + normal diet) or the control arm (normal diet only), in a 1:1 ratio according to computer-generated random numbers using the maximal procedure for random allocation. Except for one researcher who had to prescribe immunonutrition, all investigators were blinded. Due to the nature of the study, the participants could not be blinded.
Immunonutrition and perioperative care
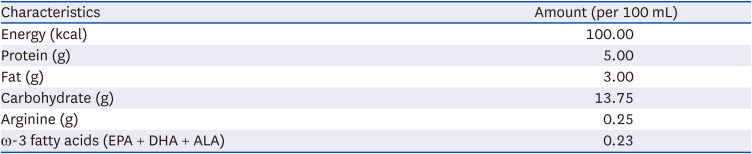
Patients in the experimental arm were prescribed with 400 mL/day of immunonutrition (Newcare Omega®; Daesang Life Science, Seoul, Korea) for 7 consecutive days prior to surgery. The oral nutritional supplement contained arginine and ω-3 fatty acids, and a high level of protein (Table 1). Using nutritional risk screening score developed by our institution [14], all patients were screened for the risk of malnutrition prior to the study enrolment. Colorectal surgical experts performed the surgical resection. Oral intake was resumed the day after surgery, and patients with no problems with diet, ambulation, and pain control were eventually discharged.
Endpoints and assessment
With the primary end point of postoperative infectious complications, sample size was calculated as 176 patients [1013]. The secondary endpoints were postoperative complication rate, changes in body weight, length of hospital stay, and composition of the fecal microbiota, of which the last was the main outcome of the present study. A fecal microbiota test was performed in 32 consecutive patients, and the samples for fecal microbiota was collected during hospital admission a day prior to surgery.
Fecal microbiota
From 16 patients in each group, 32 fecal samples were collected. The genomic DNA from the bacteria in the feces were extracted using the QIAamp DNA Stool MiniKit (Qiagen®, Hilden, Germany), in accordance with the manufacturer’s instructions. The samples were mixed with 1.4 mL ASL buffer in a 2-mL microcentrifuge tube and were vortexed. After centrifuging, a 1.2 mL aliquot of the supernatant was transferred to a new tube, vortexed with an InhibitEX tablet, and centrifuged. The supernatant was transferred to a new microcentrifuge tube, mixed with 200 μL AL buffer and 15 μL proteinase K and vortexed, and then centrifuged.
The library preparation was performed according to the 16S Metagenomic Sequencing Library Preparation Illumina Protocol. The V3–V4 region of the 16S rRNA was amplified. Polymerase chain reaction (PCR) was performed in a total volume of 25 μL containing 2.5 μL of genomic DNA, 5 μL of each primer, and 12.5 μL of KAPA HiFi Hotstart ReadyMix. The PCR consisted of 25 cycles of denaturing at 95°C for 30 s, annealing at 55°C for 30 s, and elongation at 72°C for 30 s. After the first PCR, DNA electrophoresis was performed, and a single amplification product was determined to verify the correct amplification of V4 of 16S rRNA; subsequently, the first clean-up was performed using AMPure XP beads. The index PCR was conducted by 8 cycles of denaturing at 95°C for 30 s, annealing at 55°C for 30 s, and elongation at 72°C for 30 s. After the clean-up procedure, the quality of the final library was assessed, and the amount of DNA was quantified using Agilent Bioanalyzer 1000 and Qbit. Metagenome was analyzed using EzBioCloud (ChunLab, Inc., Seoul, Korea) and BaseSpace (Illumina, San Diego, CA, USA) platform. Differences in the within-sample richness and evenness (alpha diversity) and dissimilarities between samples (beta diversity) were analyzed.
Statistical analysis
Categorical variables were compared using the χ2 test or Fisher’s exact test, while continuous variables were compared using the Student’s t-test. All results were considered significant at a P-value of < 0.05. Statistical analyses were conducted using SPSS version 26.0 (IBM Inc., Armonk, NY, USA).
RESULTS
Baseline characteristics
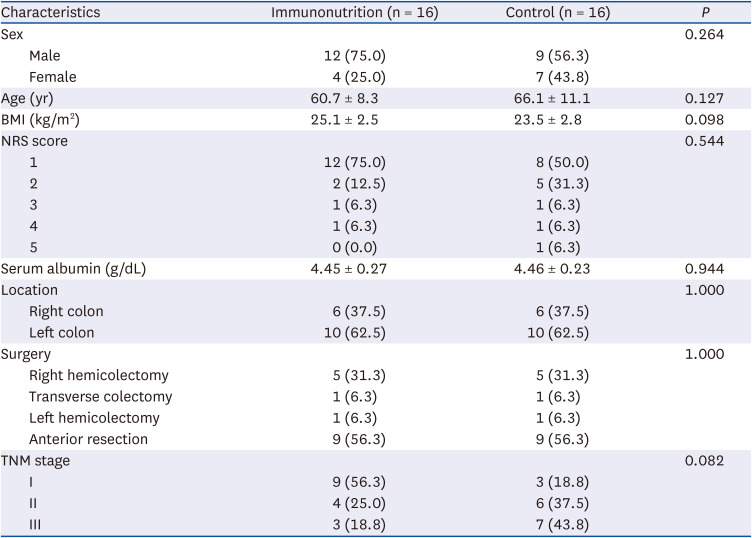
Between April 2019 and October 2020, 161 participants (experimental arm 79, control arm 82) were enrolled. As we previously described elsewhere [10], no significant differences were observed in the incidence of infectious (17.7% vs. 15.9%, P = 0.751) and total (31.6% vs. 29.3%, P = 0.743) complications, the length of hospital stay (7.6 ± 2.5 vs. 7.4 ± 2.3 days, P = 0.635), and overall change in body weight (P = 0.379) between the 2 groups. Notably, no difference was also found in the incidence of Clostridium difficile infection (3.8% vs. 3.7%, P = 0.999). For the secondary analysis, 16 patients in each arm underwent fecal microbiota test and were included in the present study. Fig. 1 shows the CONSORT flow diagram. The 2 groups showed similar clinicopathological characteristics (Table 2).

Table 2
Baseline characteristics
Diversity analysis
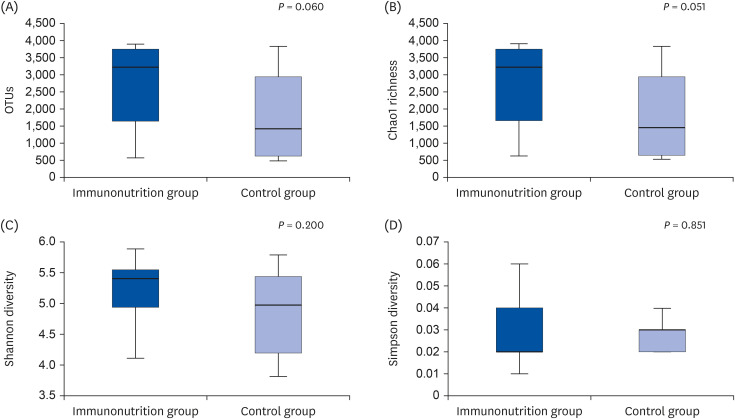
The diversity analysis revealed no significant differences in the complexity within samples in terms of observed operational taxonomic units (P = 0.060), Chao1 richness (P = 0.051), and Shannon (P = 0.200) and Simpson (P = 0.851) indices between the 2 groups (Fig. 2). Beta diversity showed no significant dissimilarities (Bray-Curtis, P = 0.124; generalized Unifrac, P = 0.210) between immunonutrition and control groups (Fig. 3).

Composition of fecal microbiota at the phylum level
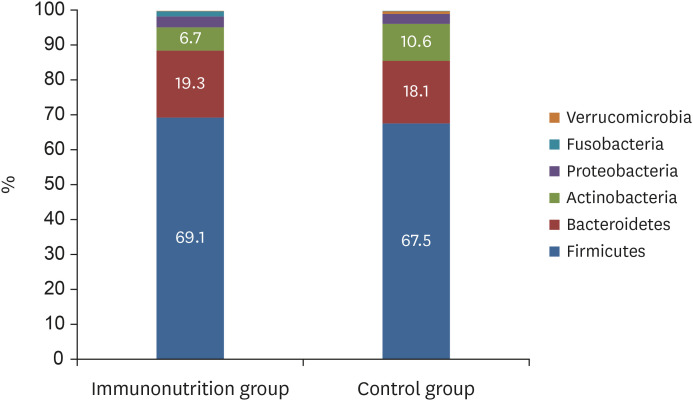
At the phylum level, no difference was found in the composition of the microbiota between the 2 groups (Firmicutes, 69.1% vs. 67.5%, P = 0.624; Bacteroidetes, 19.3% vs. 18.1%, P = 0.663; Actinobacteria, 6.7% vs. 10.6%, P = 0.080) (Fig. 4). The Firmicutes/Bacteroidetes ratio (4.43 ± 2.32 vs. 4.55 ± 2.51, P = 0.897) was also similar between the 2 groups. The detailed abundance of bacterial 16S rRNA at the phylum level is depicted in Fig. 5.

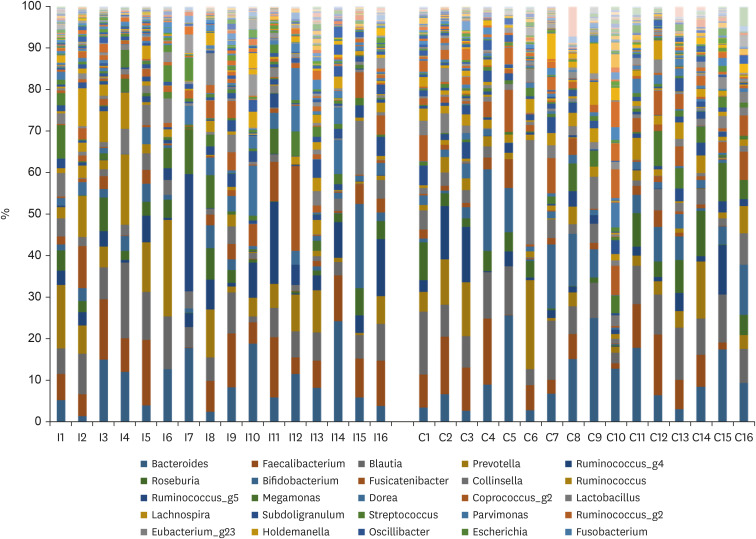
Composition of fecal microbiota at the genus level
At the genus level, the proportions of beneficial bacteria such as Faecalibacterium spp. (8.1% vs. 6.4%, P = 0.328) and Prevotella spp. (6.9% vs. 4.8%, P = 0.331) were higher, while that of Clostridium spp. was lower (0.5% vs. 1.2%, P = 0.121) in the immunonutrition group, but the difference was not statistically significant. Fig. 6 shows the abundance of bacterial 16S rRNA at the genus level. At the species level, the proportion of F. prausnitzii (3.47% vs. 2.82%, P = 0.531) was higher in the immunonutrition group, although it was not statistically significant. Only 2 patients in the control group showed presence of C. difficile (0.000% vs. 0.004%, P = 0.287). The relative abundance of bacterial 16S rRNA based on the class, order, family, and species is depicted in Supplementary Figs. 1, 2, 3, 4.
DISCUSSION
The present study showed possible association between preoperative immunonutrition and fecal microbiota composition. Immunonutrition tended to be associated with increase of beneficial bacteria and decrease of pathogenic bacteria, although the results were not statistically significant.
We initially designed an RCT based on the hypothesis that preoperative immunonutrition may be associated with the decrease in the incidence of postoperative infectious complications. The present study aimed to explain how preoperative immunonutrition can reduce infectious complications. We hypothesized that the change in the composition of fecal microbiota can be a plausible explanation of the association between preoperative immunonutrition and postoperative outcomes. However, as reported previously, the results of the RCT showed that preoperative immunonutrition was not associated with the incidence of postoperative infectious and non-infectious complications [10]. One of the most reasonable explanations of the unrelatedness is that we included normo-nourished patients; therefore, the effect of immunonutrition might have been masked. Therefore, we had concluded that the routine administration of immunonutrition prior to colorectal surgery cannot be justified [10].
Similarly, the composition of fecal microbiota did not show a significant difference according to preoperative immunonutrition, although the results showed a tendency of an increase of beneficial bacteria and a decrease of pathogenic bacteria in the immunonutrition group. One of the possible reasons is that the number of samples was too small (n = 32) to show a statistical difference. For example, the ratio of Actinobacteria did not show statistical significance even though it differed by more than 1.5 times (6.7% vs. 10.6%, P = 0.080). Another plausible explanation is that because fecal microbiota tests were only performed after administering immunonutrition, the baseline difference cannot be determined. It would have been more accurate to compare the changes in the composition of the fecal microbiota before and after immunonutrition. However, due to funding limitations, the test could only be performed after administering immunonutrition, which may have masked the actual difference. In addition, the measurement of fecal microbiota at a single point may not accurately reflect the changes in the intestinal microbiota [6]. Finally, compliance with immunonutrition may also have affected the non-significant results. As previously stated, it was difficult to determine whether the participants actually received the prescribed doses [10].
Nevertheless, the results of this study present several important perspectives. The most important point is that the proportion of beneficial bacteria such as Faecalibacterium and Prevotella was higher, while that of pathogenic bacteria such as Clostridium was lower in the immunonutrition group compared with the control group. Especially, the proportion of F. prausnitzii was higher in the immunonutrition group (3.47% vs. 2.82%, P = 0.531), although it was not statistically significant. F. prausnitzii is one of the most abundant bacteria in the human gut, which is considered as a biomarker of gut homeostasis and intestinal health [15]. Previous studies reported that the proportion of F. prausnitzii changed in several types of diseases, such as inflammatory bowel disease, colorectal cancer, type 2 diabetes, and so on [1516]. F. prausnitzii is known to play a role in maintaining immune response and metabolism, and therefore, have a potential to be used as a therapeutic agent to modulate inflammatory response [151617]. Therefore, the results of the present study show the possibility that preoperative immunonutrition may control the anti-inflammatory response by inducing changes in the intestinal microbiota such as F. prausnitzii.
Clinically, C. difficile infection is one of the most common hospital-acquired infections, which can cause severe colitis and death [18]. In our institution, C. difficile infection occurred in 0.4% and 2.3% of patients who underwent colon and rectal cancer surgeries, respectively, and delayed diagnosis may be fatal [19]. The present study showed that the proportion of Clostridium spp. was lower in the immunonutrition group (0.5% vs. 1.2%, P = 0.121), although the incidence of C. difficile infection showed no difference between the 2 groups (3.8% vs. 3.7%, P = 0.999). These results also suggest the possibility that preoperative immunonutrition can have a positive effect on the outcomes of colon cancer surgery by decreasing pathogenic bacteria.
Several immunonutrients such as glutamine, arginine, and ω-3 fatty acids are known to affect the patient's immune status after surgery [12]. Arginine maintains microcirculation and promotes wound healing by stimulating the secretion of growth hormone [12]. ω-3 fatty acids are known to prevent excessive inflammatory responses, acting as anti-inflammatory mediators [12]. Foods rich in ω-3 fatty acids may increase the diversity of the gut microbiota and modulate inflammatory status [20]. The type and amount of protein may also be associated with the composition of the gut microbiota [21]. A recent RCT reported impact of long-term protein supply on gut microbiota [22]. Hence, immunonutrition used in the present study, which contains arginine, ω-3 fatty acids, and a high level of protein, may influence the composition of gut microbiota after colon cancer surgery. However, we only showed a tendency of association between immunonutrition and changes in fecal microbiota, and failed to prove statistical significance.
Although we did not show any statistical significance, some previous studies reported important changes in the composition of the intestinal microbiota after undergoing colorectal surgery [5]. A previous study showed that reduced alpha diversity was associated with the incidence of postoperative complications [23]. A higher abundance of specific bacteria, such as Bacteroidaceae, Bifidobacterium genus, and Enterococcus faecalis, may be associated with an increased risk of anastomotic leakage [2524]. In addition, the Firmicutes/Bacteroidetes ratio can be altered during colorectal cancer surgery, which may represent dysbiosis of the intestinal microbiota and can be associated with poor outcomes [5]. Hence, further large-scale studies are warranted to investigate the effect of immunonutrition on the outcomes of colorectal cancer surgery.
In conclusion, we showed a tendency of association between immunonutrition and changes in fecal microbiota, which was an increase of beneficial bacteria and a decrease of pathogenic bacteria. The relationship between immunonutrition and the fecal microbiota should be investigated further in large-scale studies.
 XML Download
XML Download