

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
While traditionally occupational health has focused on exposure to hazardous materials (chemical, biological, or physical), mental health is gaining increasing interest in the field.1 Numerous studies have identified working conditions, such as job stress,2 shift work,3 and exposure to physical or chemical hazards,45 as risk factors for mental health problems. Moreover, there is a bidirectional relationship in that mental health also affects occupational experience. In the United Kingdom, approximately 40% of sick leaves in the workplace are attributed to mild mental disorders, such as depression and anxiety.6 Moreover, mental disorders cause a major disease burden among individuals of working age,7 underlining the need to promote mental health in occupational settings.
Although increased attention on mental health promotion in workplaces has encouraged governments to implement legislation, gaps exist between laws and their enforcement, even in industrialized countries. Jain and colleagues8 have divided the gap into three categories: infrastructure and human resources (implementation gap), qualitative comprehensiveness (capacity gap), and inclusion of all employees (coverage gap). In South Korea, occupational health management is similarly challenged in that tasks of mandatory occupational health managers within companies are often limited to managing work-related injuries and chronic diseases, such as hypertension and diabetes.9 Challenges and barrier to implementing mental health strategies are multifactorial in nature, including a lack of professionals and of comprehensive systems for screening and treatment of at-risk populations, as well as a lack of concern among employers.9 Therefore, there is a need for an easy-to-implement intervention for occupational mental health to provide a universal management approach, regardless of the specialization of occupational health managers in workplaces.
Digital technology has been employed in occupational mental health management10 to provide greater accessibility and reduced professional requirements, and thus can enhance coverage and improve implementation gaps.1112 However, digital interventions do have limitations. As an example, a study using a web-based approach found that while the intervention was effective in accelerating the rate of return to work, low adherence of both occupational physicians and participants and a high rate of loss to follow-up were identified.13 Low adherence was also identified in another study conducted among nurses, in which more than half of the participants assigned to an e-mental health intervention dropped out.14 In addition to adherence problems, insufficient maintenance of benefits for employees underlined the need for a continuous approach to the management of occupational mental health.12
A novel approach can be adopted from Screening, Brief Intervention, and Referral to Treatment (SBIRT) model. Intended to be implemented by non-professionals (such as in primary care or by nursing staff),15 the model could improve universal access to effective mental health management in the workplace. The SBIRT model was initially developed to identify and provide treatment for substance use disorders.15 Between the steps of screening and referral, the practitioner delivers brief interventions that focus on enhancing an individual’s insight and awareness on their disorder.15 Evidence of the effectiveness and feasibility of the SBIRT model in the workplace is accumulating.1617 It has been found to be effective for other mental health problems in community samples.18 Considering that the importance of worker health surveillance programs has long been emphasized in occupational medicine,19 the SBIRT model has the potential to provide cost-effective benefits to employees.
Based on this evidence and the identified need for effective management of occupational mental health surveillance, we developed a SBIRT model-based intervention that uses a smartphone application to guide occupational health managers and employees in promoting mental health surveillance, education, and treatment in the workplace. The SBIRT-based approach was designed to fulfill the following three criteria: easy implementation, good adherence, and continuous management.
METHODS
The new SBIRT model based occupational mental health management system we present herein was included as part of a larger occupational health promotion system. The system is designed to help occupational health managers provide better management of their employees’ mental health issues. The system integrates participants’ basic demographic data, medical information, and lifestyle factors, with an evaluation of job stress.
Preparation phase
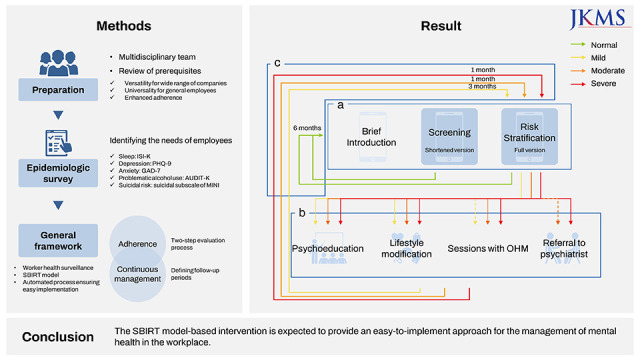
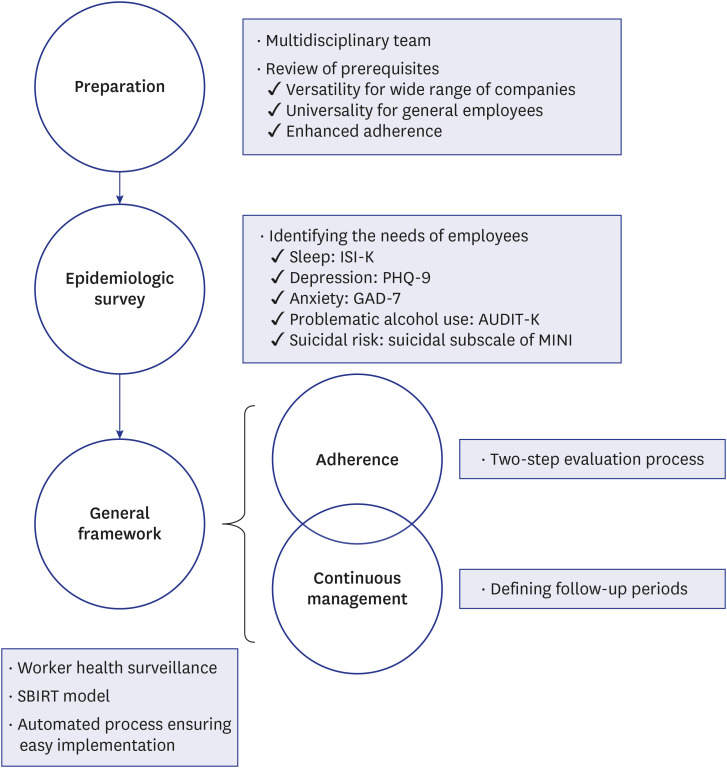
The flow diagram of the development process for our model is illustrated in Fig. 1. The model was developed by a multidisciplinary team, including occupational health physicians, nurses, psychiatrists, and software developers. Opinions from occupational health managers were also gathered on several occasions with the goal of providing a better user experience with our digital intervention. Prerequisites for the implementation, such as occupational health management settings and implications from previous studies, were reviewed (Fig. 1).
Fig. 1
General flow of the development of the SBIRT-based occupational health intervention.
ISI-K = Korean version of the Insomnia Severity Index, PHQ = Patient Health Questionnaire, GAD = Generalized Anxiety Disorder, AUDIT-K = Korean version of the Alcohol Use Disorders Identification Test, MINI = Mini International Neuropsychiatric Interview, SBIRT = Screening, Brief Intervention, and Referral to Treatment.
Epidemiological survey
We conducted an epidemiological survey to examine the need for mental health management among employees by evaluating the prevalence of mental health problems. Participants were recruited through advertisements and announcements to companies in Gangwon Province, South Korea, who were included in the occupational management service provided by Wonju Severance Christian Hospital. The study included all participants who consented, except for those who had difficulties using a smartphone, as the survey was conducted using a smartphone application. Through a smartphone application, participants completed the Korean version of the Insomnia Severity Index (ISI-K),20 Patient Health Questionnaire (PHQ)-9,21 Generalized Anxiety Disorder (GAD)-7,22 Korean version of the Alcohol Use Disorder Identification Test (AUDIT-K),23 and suicidality subscale of the Mini International Neuropsychiatric Interview (MINI).24 The reported cut-off values for each scale were used to determine the prevalence of each mental health disorder, as follows: insomnia, 10; depression, 10; anxiety, 10; alcohol use disorder, 20 for men and 10 for women; and suicidal risk, 6. The proportion of participants for previously determined severity criteria was also reviewed.
Development of the general framework
Following the epidemiological survey, the general SBIRT framework was developed. The SBIRT model includes regular screening, using self-administered questionnaires; brief interventions, based on psychoeducation delivered through mobile applications and sessions with occupational health managers; and referral to psychiatric treatment for employees with clinically relevant symptoms. The model was developed on a web-platform and included a smartphone application to guarantee accessibility to occupational health managers and employees. The model ensures that screening and access to psychoeducational materials is universally accessible, via smartphone applications, to employees, as needed, under supervision of occupational health managers in the workplace.
Measures to enhance program adherence
To enhance adherence, a two-step evaluation process was designed to simplify regular screening of mental health problems (Fig. 2A). This included the use of the short-form version of tools used to screen participants to reduce the burden of surveys. Those meeting the cut-off scores for a mental health problem are then asked to complete the appropriate long-form version of mental health scales used. The following short-form scales, in Korean, were selected for the first-step screening: ISI-3,25 PHQ-2,26 GAD-2,27 and brief AUDIT28 for insomnia, depression, anxiety, and problematic alcohol use, respectively. In the absence of a brief version of the suicidality subscale of the MINI, the suicide item (item 9) of the PHQ-9 was used.
Fig. 2
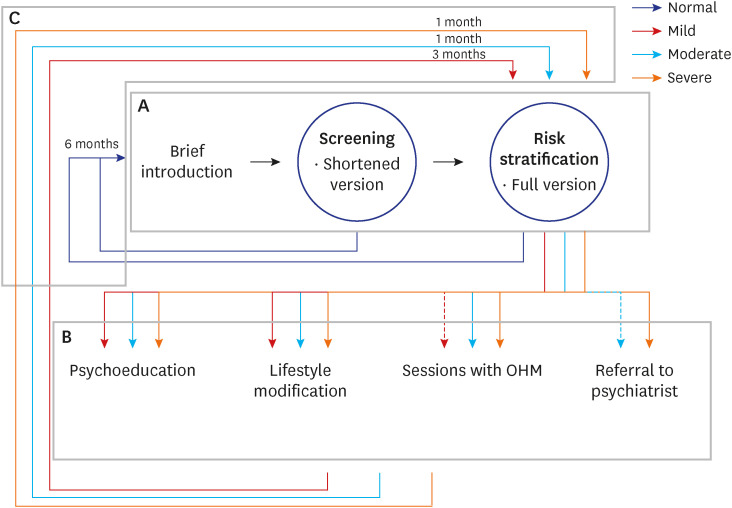
The outline of the intervention. Each square represents parts of the intervention. (A) Screening and risk stratification; (B) Recommendations; (C) Follow-up and continuous surveillance. Colors of lines indicate the severity of symptoms for a mental health problem. Dashed line indicate that the strategy is offered on condition.
OHM = occupational health manager.
To confirm that the two-step process did not alter the clinical validity of results, the two-step process was simulated using the results of the epidemiological survey. Kappa statistics and McNemar’s test were used to compare the differences between the one- and two-step processes. The ordinary kappa coefficient was calculated to examine the agreement between the two processes and McNemar’s test was used to identify differences in dichotomous diagnostic variables between the two processes. The quadratic weighted kappa coefficient was calculated for severity variables. Landis and Koch criteria used to interpret kappa coefficients.29 The cut-off values for the first step were adjusted according to the results of statistical analyses combined with experts’ opinions.
All statistical analyses were two-sided with a significance threshold of 0.05. Statistical Package for the Social Sciences (SPSS) version 23 (SPSS, Chicago, IL, USA) was used to perform the analyses.
Measures for continuous management
Regular surveillance was planned for the continuous management of employees’ mental health. In particular, the schedule for follow-up surveillance differed according to the risk stratification by severity for each mental health problem evaluated. This schedule of follow-up was determined based on expert opinions during multidisciplinary team meetings. Follow-up surveillance was automated, with reminders sent directly to employees and to occupational health managers, who could provide additional notification and follow-up for employees who do not complete their regular surveillance.
RESULTS
Results from the epidemiological survey
A total of 346 employees completed the epidemiological survey, with the prevalence of each mental health problem presented in Table 1, and with the severity criteria for each scale presented in Supplementary Tables 1, 2, 3. The distribution of prevalence for each mental health problem screened for was as follows: insomnia, 10.7%; depression, 4.3%; anxiety, 3.5%; problematic alcohol use, 13.3%; and suicidal risk, 2.9%.
Table 1
Mental health problems among employees by diagnosis (N = 346)
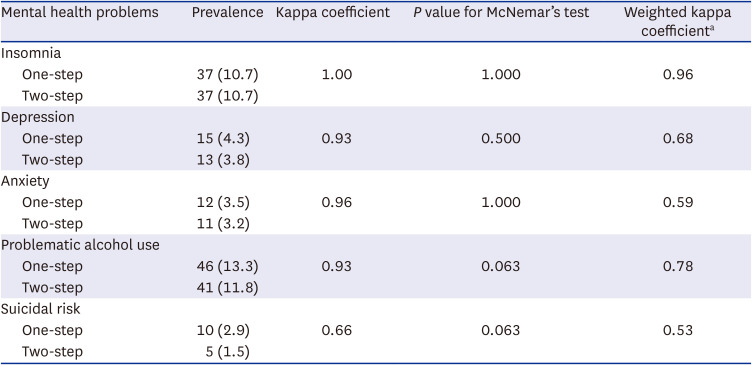
The ordinary kappa coefficient values for the one- and two-step evaluation processes were 1.00, 0.93, 0.96, 0.93, and 0.66 for insomnia, depression, anxiety, problematic alcohol use, and suicidal risk, respectively (Table 1). The kappa coefficients for diagnosis were within the ‘almost perfect’ range for insomnia, depression, anxiety, and problematic alcohol use, with ‘substantial’ agreement for suicidal risk. McNemar’s test revealed that there was a statistically significant difference in prevalence between the one-step and two-step processes for insomnia (P = 0.008). This result indicates that the widely accepted cut-off value of ‘7’ for the ISI-3 is too high for the two-step process, resulting in some participants with sufficient symptoms of insomnia on the ISI-K being classified as normal on the ISI-3. Therefore, the cut-off value for ISI-3 was adjusted to ‘4,’ as suggested in a recent study for use of the ISI-3 in a two-step screening procedure.30 After adjustment, the results for the two evaluation processes showed a perfect match (Table 1).
The new SBIRT-based model
Our model includes three-steps: screening and risk stratification; mental health management, consisting of brief intervention and referral for treatment, as appropriate; and follow-up and continuous surveillance (Fig. 2). Screening and risk stratification were based on the two-step process. The brief interventions for mental health management included psychoeducation, lifestyle modification, self-help methods, referrals to medical services, and recommendations for follow-up. A detailed description of each step is provided below.
Screening and risk stratification
Employees will complete the screening mental health scales, via a mobile application, for the five areas of mental health assessed: insomnia, depression, anxiety, problematic alcohol use, and suicidal risk. Employees are required to complete the scales regularly for surveillance purposes. Prior to each scale, a short script is provided to explain the mental health area being evaluated. As previously mentioned, to enhance the completion rate, a two-step process was used: screening and risk stratification (Fig. 2A). Short-form versions of the scales are first completed for screening. In the case of a positive screen, the participant is asked to complete the long-form version of the scale for a more precise evaluation and risk stratification.
For risk stratification, participants are classified into one of the following four severity groups, based on the scale score obtained: normal, mild, moderate, or severe. For easier and more intuitive communication of the severity classification, we used green, yellow, orange, and red lights for the normal, mild, moderate, and severe classifications. A negative screen is considered a ‘normal’ classification. Risk classification of a positive screen was based on established severity scores, but with the multidisciplinary team making some adjustments for the evaluation of depression, problematic alcohol use, and suicidal risk. The original developers of the scales used for depression and problematic alcohol use recommended ‘five’ and ‘three’ categories of severity, respectively. To align with the universal classification used for risk stratification in our systems (mild severity/yellow light, moderate/orange light, and severe/red light), ‘moderately severe’ and ‘severe’ classifications of depression were grouped as severe (red light), while for alcohol consumption, hazardous drinking was classified as mild (yellow light) and alcohol dependence as ‘moderate’ (orange light). For suicidality, experts on our team agreed that any participants who scored higher than the normal group would be classified as being at a ‘severe’ risk (red light), ensuring that these participants receive the highest attention and are referred to psychiatric specialists. Table 2 summarizes the scales used in the first and second steps and the adjusted cut-off values for each scale.
Table 2
Name of scales used for the two-step evaluation process of mental health problems and their cut-off values

Brief intervention and referral to treatment
For each participant, recommendations for management are distributed in a stepped-wise manner according to the severity classification of mental health problems identified. Recommendations consists of brief interventions and referrals to psychiatrists. Brief interventions included psychoeducation to increase participants’ insight and awareness of the mental health issue and self-help methods and lifestyle modifications. Educational materials are primarily distributed automatically through mobile applications, with sessions scheduled with an occupational health manager for discussion. The recommended process for brief interventions and referrals to treatment for each severity classification is shown in Fig. 2B for each mental health problem. Briefly, more comprehensive psychoeducational materials and sessions with an occupational health manager are provided to individuals with a higher severity classification. Referral to treatment is recommended for the orange light (moderate) or red light (severe) classification groups, as the lower cut-off values for the orange group match the cut-off values for the diagnosis of disorders. A detailed description of these recommendations is provided in Table 3.
Table 3
Summary of recommendations provided for each severity group
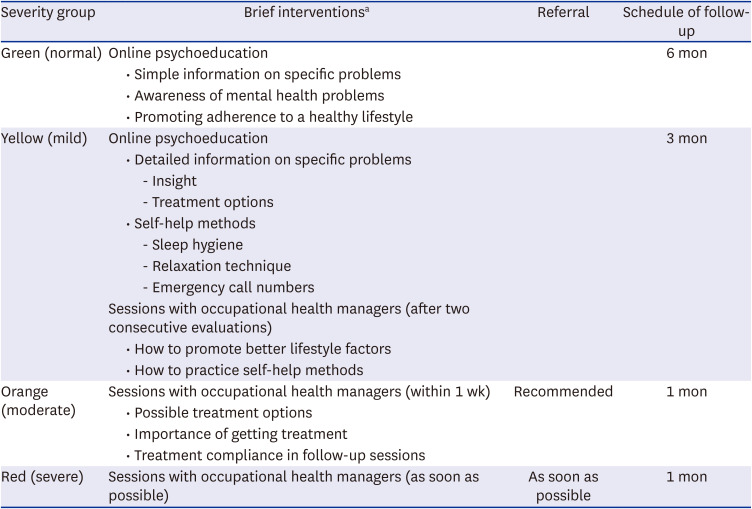
Recommendations for follow-up
The schedule of follow-up was also determined according to the severity of mental health problems, with a follow-up recommended at six months for the green light classification, three months for the yellow light classification, and one month for the orange and red light classifications (Fig. 2, Table 3). At the pre-specified follow-up schedule, the mobile application automatically notifies the employee to complete the full version of the scale for the specific mental health problem. For example, when a participant was classified into the orange light (moderate) group for a sleep problem, the participant is asked to complete the ISI-K after one month. The intervention is repeated according to the results of the follow-up evaluation.
DISCUSSION
Herein, we described a new SBIRT-based occupational mental health management system to screen for mental health problems among employees, combined with risk stratification, intervention, and follow-up. The system was based on results from an epidemiological survey which provided an overview of the prevalence of insomnia, depression, anxiety, problematic alcohol use, and suicidal risk in a group of 346 employees. For ease-of-application, accessibility and enhanced adherence, the system was implemented on a web platform with a smartphone application.
Our epidemiological survey did identify that mental health problems are prevalent among employees within workplaces under the occupational management service of Wonju Severance Christian Hospital. Our findings are consistent with the prevalence previously reported for a general population in South Korea, using the same measures and cut-off points as in our study: a prevalence of 10.7% for insomnia and 4.3–6.1% for depression.3132 Although we were not able to find studies using same measures, a prevalence of 12.2% for alcohol use disorder and 9.3% for anxiety has been reported.33 Our lower prevalence of anxiety (4.3%) compared to the 9.3% prevalence previously reported33 might reflect differences in criteria used for the diagnosis,34 indicating the need for further attention to identify whether the cut-off value for anxiety needs to be adjusted. Overall, the prevalence of mental health problems identified in our epidemiological survey and previous studies underline the need for management of mental health in workplaces to avoid the decrease in productivity and other social consequences of mental health problems.
Our epidemiological survey also showed that the two-step evaluation process we used, namely screening first using short-form of selected scales and the use of long-form versions based on risk stratification enhances employee adherence while ensuring diagnostic value. While research on the two-step process is scarce, a recent meta-analysis did report that using the short-form PHQ-2 and long-form PHQ-9 in combination resulted in better accuracy while significantly reducing the need to answer the long-form.35 In our study, the two-step process significantly reduced the number of items employees needed to answer, with only 12 items for the first screening step, while also maintaining its diagnostic value. Moreover, the risk stratification by severity remained relatively stable when using the two-step process, compared to the one-step process. We do note that most disagreements between two processes occurred between the lowest and second lowest severity groups (green and yellow light classification), identifying the need for further research to determine optimal cut-off values for short-form versions of scales and the clinical significance of these cut-offs. Although digital psychiatric interventions do have certain beneficial characteristics with promising results having been shown, adherence to recommendations on a digital platform is an obstacle.3637 As screening is the first step for an individual to engage with the SBIRT model, it is crucial that employees complete their regular surveillance. Although further research is warranted, we postulate that reducing the burden of answering unnecessary items by using short-form versions of selected scales in the two-step evaluation process can enhance adherence to regular surveillance.
We expect that our new SBIRT-based intervention will be beneficial to employees. Although more evidence is needed for areas other than problematic substance use, the SBIRT model include several components that can help manage mental health problems. First, through regular surveillance, the model enables early detection of mental health problems, a benefit that has long been emphasized.38 Studies have shown that the duration of untreated illness is related to the clinical outcomes of psychiatric diseases.3940 In line with these studies, a model intended for early detection and feedback has also shown positive results in occupational health.19 Second, brief interventions, including psychoeducation, can help employees manage their mental health problems. Our intervention provided various psychoeducational materials that targeted improving insight, awareness of symptoms, and better management of mental health problems. Although psychoeducation is a simple and cost-effective option, it is often deemed ineffective. However, meta-analyses have shown psychoeducation to be an effective treatment option, even when limited to passive and not adjunctive to other treatments.4142 Moreover, brief interventions included in our model included improving employees’ mental health literacy. Presenting information on mental health problems before answering scales for the surveillance improves employees’ mental health literacy to facilitate help-seeking behavior and enables recognition of coworkers’ symptoms, leading to early identification and intervention,43 even for those who do not have a positive screen. Third, our model includes referral to treatment based on risk stratification, intended to decrease the chance of delaying comprehensive care by promptly recommending a referral to a psychiatrist for employees with significant symptoms. Finally, the pre-defined schedule of follow-up for regular screening of mental health symptoms provides continuous management. To our knowledge, most studies focused on a single administration of the intervention and did not consider how the follow-up should be performed. Insufficient maintenance of treatment effects has been reported in previous studies.12 Considering that common mental disorders relapse, employees can benefit from the continuous surveillance and management of mental health problems.
Easy implementation is an important characteristic of our intervention. Mental health interventions that require additional staff can increase the cost to a company, which can be a barrier to implementation. Through automatic screening of at-risk populations and the management of mild symptoms with psychoeducational materials, human resources can be efficiently allocated to employees with severe symptoms. Therefore, our proposed intervention is intended to be run by a minimal number of staff members. For countries where appointing occupational health managers is mandated by law for most types of businesses, we expect that our intervention can be implemented by occupational health managers, regardless of their specialties. Moreover, automation of the screening process and distribution of psychoeducational materials using digital technologies brings additional benefits to employees, such as improved accessibility and reduced feelings of stigmatization, as previously reported.44 Therefore, by using personal electronic devices, employees can easily access mental health scales and review psychoeducational materials while feeling less stigmatized regarding their mental health problems.
In addition to the two-step evaluation process, human contact embedded in the intervention is also expected to enhance adherence to the intervention. Although there are conflicting reports and further studies are needed,45 some studies have demonstrated the beneficial effect of human support on adherence.4647 Therefore, by scheduling frequent sessions with occupational health managers for employees with higher severity of mental health problems, adherence to recommendations and possibly referral to psychiatric treatment can be enhanced.
Currently, recruitment for a short-term pilot study to evaluate the feasibility and preliminary effectiveness of our intervention system has begun. Following completion of the pilot study, a pragmatic trial is planned to evaluate the effectiveness and feasibility of the intervention. In contrast to a general explanatory study, a pragmatic study is a useful method to measure benefits in real-life clinical settings.48 Considering that adherence and real-life application are known limitations of digital mental health interventions,12 the authors expect that examining the effectiveness rather than efficacy of the intervention will provide more useful evidence regarding its real-life application.
For the pragmatic trial, a large population of workers residing in Gangwon Province, South Korea, will be recruited. Eligible participants will be the nearly 12,000 workers across the 150 companies participating in the occupational health management service of Wonju Severance Christian Hospital. Participants who agree to participate in the trial will be randomly assigned to either the intervention or the control group. Outcomes evaluated will include mental health scores on scales used, as well as assessment of quality of life and overall distress and of adherence, and satisfaction with the intervention.
The limitations of our study should also be considered. First, although digital therapeutics generally provides greater accessibility, those who are not familiar with digital devices might have trouble using the intervention. Surveillance and brief psychoeducation, which are core features of our intervention, were accessed through smartphone applications. Therefore, sufficient time should be spent on educating employees to familiarize themselves with the smartphone application. Second, the results of the two-step evaluation process were derived from the responses to long forms of the mental health scales used. The possibility that individuals might respond differently according to the order of the items cannot be ruled out. Therefore, these results should be cautiously interpreted.
In conclusion, we present a new model for the management of occupational mental health. The model, developed by a multidisciplinary team, is expected to provide an effective management of employees’ mental health. The intervention was designed for convenient implementation and to enhance employee adherence and assist occupational health managers in providing continuous management. Further studies are needed to examine the effectiveness and feasibility of the proposed intervention. Trials should also include outcome parameters evaluating adherence, quality of life, and client satisfaction with the intervention.
 XML Download
XML Download