

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Emotional eating is well defined in Bruch’s psychosomatic theory, which posits that negative emotions can trigger eating disorders [1]. Emotional eating is also referred to as “the tendency to overeat in response to negative emotions, such as anxiety or irritability” in other theory [2]. Emotional eating occurs not because of hunger cues but because of emotions and is more common in women than men [34]. For women, there might be psychological and physical factors that frequently lead to emotional eating. Nguyen-Rodriguez et al. [5] found an association between perceived stress and emotional eating, while Costa et al. [6] revealed that women have higher perceived stress scores than men, which are particularly significant in the age group from 19–39 yrs. Klump et al. [7] found an association between emotional eating scores and each phase of the menstrual cycle. Klump et al. [8] also found the highest emotional eating scores during the mid-luteal phase.
Women experience menstruation for almost 40 yrs during their lifetimes [910]. The average length of the menstrual cycle from the first day of menstrual bleeding to the first day of the next cycle is approximately 28 days [11]. The menstrual cycle consists of 4 stages involving interactions of various hormones: the menstrual phase, the follicular phase, ovulation, and the luteal phase [12]. During the luteal phase, many women experience premenstrual syndrome (PMS) and PMS-related physical, emotional, and behavioral symptoms. These symptoms may impair the daily lives of women [13]. Approximately 50–80% of childbearing-aged women have one or more premenstrual symptoms, but very few recognize the need to manage or treat these symptoms. Ryu and Kim [14] also reported improper management of PMS. Some women who experience severe symptoms of PMS that meet the criteria of the Diagnostic and Statistical Manual of Mental Disorder can be diagnosed with the premenstrual dysphoric disorder (PMDD). The symptoms of PMDD vary widely but can include affective lability and physical symptoms such as mood swings, depression, anxiety, bloating, breast tenderness, and changes in appetite, especially overeating [15]. These various symptoms of PMDD can interfere with women’s daily lives.
Previous studies with similar topics have investigated the association among psychological factors, PMS/PMDD, and eating behaviors. Yen et al. [16] studied 2 groups of a PMDD and a control divided according to the scores of a PMDD severity questionnaire. According to Yen et al.’s study [16], in the PMDD group, the desire to eat and food cravings were greater in the late-luteal phase, and impulsivity and irritability were associated with the desire to eat. Ha et al. [17] also conducted a study on 2 groups including a PMDD and a control group. The study by Ha et al. [17] found higher trait anxiety, depression, and restrained eating symptoms in the PMDD group than in the control group, in particular, trait anxiety was associated with increased and unrestrained eating symptoms during the premenstrual and chronic processes of PMDD. These studies found similar findings that there may be a negative impact on emotional states and eating habits in groups with relatively high PMS scores during certain menstrual cycle stages.
The menstrual cycle occupies a significant proportion of a woman’s life making it important to manage and relieve PMS/PMDD symptoms for women’s quality of life. Fluctuations in various hormone levels during the menstrual cycle may cause psychological and physical changes that can increase stress and lead to unhealthy eating habits [818]. The objective of this study was to investigate the relationship of how emotional eating is related to PMS and negative perceived stress by comparing a PMDD group and a non-PMDD group. The research questions of this study are presented below.
• Does negative perceived stress mediate the effect of PMS on emotional eating?
• If negative perceived stress mediates the effect of PMS on emotional eating, is there a difference in the mediating model between the PMDD group and the non-PMDD group?
• Is an affective factor of PMS the most important factor in emotional eating?
Go to : 
SUBJECTS AND METHODS
Participants and data collection
A survey was conducted involving 409 women aged 20 to 39 yrs residing in Seoul and Gyeonggi-do, South Korea. To minimize the differences caused by body mass index (BMI) range, the study was limited to participants with a BMI ranging from 18.5 to 29.9 kg/m2, which is defined as normal to obese. BMI is an objective index of body weight determined by the ratio between weight in kilograms and height in meters. In addition, all participants were recruited as an allocation sample according to age and marital status to avoid biased results. A total of 25 questionnaires that excluded descriptive information from 409 women were statistically analyzed, with the exception of 15 outliers. Then, participants were divided into a PMDD and a non-PMDD group according to the scoring system to conduct comparative analyses [19]. This study was approved by the Institutional Review Board of Kookmin University (KMU-202012-HR-251) and was conducted via a web-based survey.
Measurements
Emotional eating
The Emotional Eater Questionnaire (EEQ) is an emotional eating behavior measurement tool. The EEQ is a 10-item questionnaire proposed by Garaulet et al. [20] that uses a scale range from 0 (not at all) to 3 (very much). Higher scores indicate that respondents have unhealthier eating behaviors and are more likely to be emotional eaters. The validity and reliability of the EEQ were confirmed in a previous study. The EEQ has a good enough agreement with the Mindful Eater Questionnaire, which measures mindful eating with good internal consistency reliability [2021]. Although the EEQ was originally developed for overweight and obese individuals, researchers have used this tool for individuals in the normal to the obese range with appropriate reliability and validity [2223]. This study adopted the EEQ to assess the emotional eating behavior status since it is a compact questionnaire suitable for online surveys. Emotional eating was expected to be a result variable affected by PMS and negative perceived stress in this study.
PMS/PMDD
The Shortened Premenstrual Assessment Form (SPAF) is a questionnaire that measures the degree of PMS using self-reported symptoms for the week before menstruation. The SPAF includes 10 questions from the Premenstrual Assessment Form, which is a PMS measurement scale developed by Allen et al. [24] that is more convenient and practical in clinical use. This study used the Korean version of the SPAF as translated and verified by Lee et al. [19]. The SPAF uses a scale from 1 (no present at all or no change at the usual level) to 6 (extreme change) and consists of 3 factors: water retention, pain, and affective factors. Water retention and pain refer to physical symptoms, while affective factors refer to the emotional symptoms caused by PMS. The study also demonstrated that 4 items (SPAF items 1–4) were affective factors, 3 items (SPAF items 5–7) were pain factors, and the other 3 items (SPAF items 8–10) were water retention factors. They suggested that the diagnosis of PMDD be made based on a score of 27 points, and found that affective factors were the best predictor of distinguishing between individuals with and those without PMDD based on sensitivity and specificity. This study divided its participants into PMDD and non-PMDD groups. Afterward, mediation analysis was performed with each item from the 10-item survey and PMS affective factors. PMS was established as a causal variable for negative perceived stress and emotional eating in this study.
Negative perceived stress
The Perceived Stress Scale (PSS) is a simple scale for measuring an individual’s recent stress that focuses on subjective experiences that have occurred over the past month [25]. The PSS, which many studies have revealed to have a 2-factor model with negative and positive factors, is widely used to assess an individual’s stress level [26]. Park and Seo [27] translated and validated the PSS in Korean. Their findings supported the 2-factor model with negative and positive perceptions. They suggested using each factor of the Korean PSS version independently since negative perception-related measures assess negative emotion and positive perception-related measures assess positive emotions. The current study was conducted using only negative perception-related questions to evaluate the degree of negative perceived stress. These questions referred to the Negative Perceived Stress Scale (NPSS) in this study, which consisted of 5 items on a scale of 0 (not at all) to 4 (very often). The NPSS was used to measure negative perceived stress, which was hypothesized to mediate the relationship between PMS and emotional eating.
The measurement items used in this study are presented in Table 1.
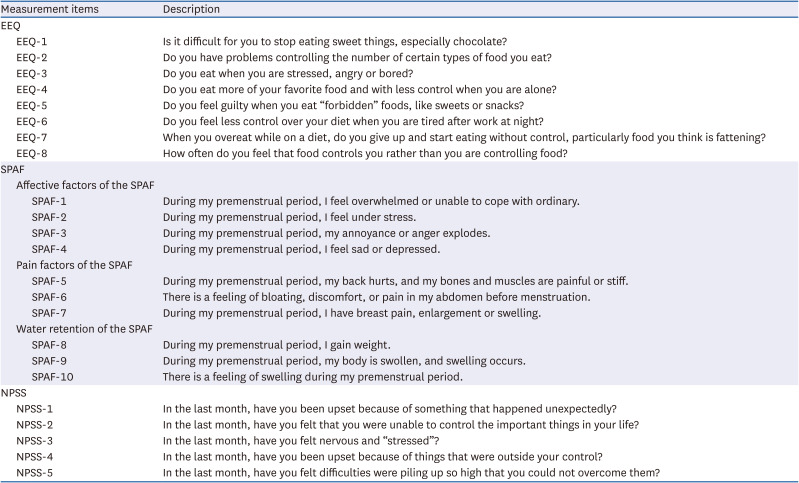
Table 1
Measurement items
The EEQ was used to measure the degree of emotional eating as a dependent variable. The SPAF was used to measure the degree of premenstrual syndrome/premenstrual dysphoric disorder as an independent variable. The NPSS was used to measure the degree of negative perceived stress as a mediator.
EEQ, Emotional Eater Questionnaire; SPAF, Shortened Premenstrual Assessment Form; NPSS, Negative Perceived Stress Scale.
![]()
Statistical analysis
Data analysis was performed using the responses from 409 participants who answered all questions on the EEQ, SPAF, and NPSS. Data analyses were conducted using SPSS version 28.0 (IBM, Inc., Armonk, NY, USA) and SPSS AMOS version 26.0 (IBM, Inc.) at a significance level of 0.05. Descriptive analysis was used to demonstrate the demographic characteristics of respondents. Independent t-tests were used to compare BMI, the degree of emotional eating, PMS, and negative perceived stress between the PMDD and non-PMDD groups. In addition, to assess the reliability and validity of each item and their measurements, confirmatory factor analysis using AMOS version 26.0 was performed. Furthermore, mediation analysis was used to test the relationships among emotional eating, PMS, and negative perceived stress using the PROCESS macro for SPSS developed by Andrew F. Hayes.
Go to :
RESULTS
Respondent characteristics
The demographic information from 409 respondents is shown in Table 2. The average age of the respondents was 30.55 yrs. Using quota sampling, an evenly distributed number of respondents were recruited for the age and marital status categories. With regard to the distribution by age group, 49.4% of respondents were aged 20–29 yrs, and 50.6% were aged 30–39 yrs. In terms of marital status, 49.6% were married, and 50.4% were single. The average BMI was 21.97, which is in the normal weight range. In total, 68.5% were in the normal range, 16.9% were overweight, and 14.7% were obese. In addition, 72.4% (296 respondents) of the respondents were included in the PMDD group, and 27.6% (113 respondents) were included in the non-PMDD group. The PMDD and the non-PMDD groups had average scores of 10.58 (standard deviation [SD] = 4.59) and 8.19 (SD = 5.40), respectively, for emotional eating.
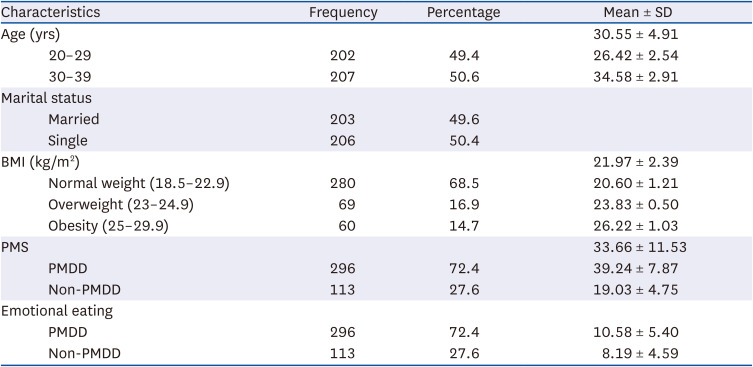
Table 2
Participant characteristics (n = 409)
Emotional eating was measured by the Emotional Eater Questionnaire. PMS was measured by the Shortened Premenstrual Assessment Form, and the group was divided according to the cut-off score of 27.
BMI, body mass index; PMS, premenstrual syndrome; PMDD, premenstrual dysphoric disorder; SD, standard deviation.
![]()
Measurement validation
The results of the confirmatory factor analysis are presented in Table 3. All factor loading values exceeded 0.5, and the 2 items of the EEQ that had values less than 0.5 were deleted. The estimates of average variance extracted (AVE) from the EEQ, SPAF, and NPSS questionnaires were 0.45, 0.51, and 0.60, respectively. Although the AVE value of the EEQ did not exceed the minimum threshold of 0.5, the convergent validity of the construct was still sufficient because the composite reliability (CR) and Cronbach’s α were sufficiently high [28]. All 3 questionnaires’ CR exceeded the threshold of 0.7 (EEQ = 0.87; SPAF = 0.91; NPSS = 0.88), and Cronbach’s α values were high enough (EEQ = 0.87; SPAF = 0.93; NPSS = 0.89). As a result of performing the exploratory factor analysis on the SPAF, all internal validity criteria were met, and the cumulative percentage of the total variance explained was 82.66%. The internal structure included 3 subfactors (pain, water retention, and affective factors) similar to the results by Lee et al. [19].
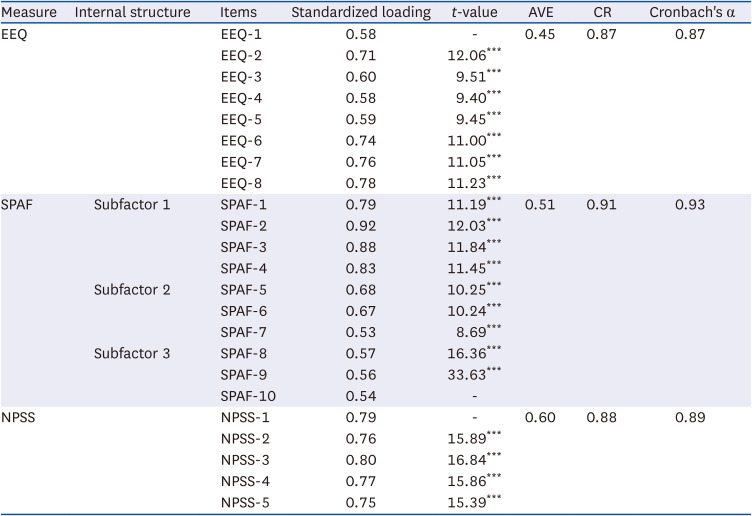
Table 3
Confirmatory factor analysis of measurements
The EEQ was used to measure the degree of emotional eating as a dependent variable. The SPAF was used to measure the degree of premenstrual syndrome/premenstrual dysphoric disorder as an independent variable. The NPSS was used to measure the degree of negative perceived stress as a mediator. Principal component analysis of the SPAF was implemented in the method of varimax rotation with Kaiser normalization: Kaiser-Meyer-Olkin = 0.89, chi-square approximation = 3,754, df = 45, P = 0.000.
AVE, average variance extracted; CR, composite reliability; EEQ, Emotional Eater Questionnaire; SPAF, Shortened Premenstrual Assessment Form; NPSS, Negative Perceived Stress Scale.
***P < 0.001.
![]()
Analysis of differences between groups
Comparative data between the PMDD group and the non-PMDD group are presented in Table 4. The average of each variable (emotional eating, PMS, and negative perceived stress) was statistically significantly higher in the PMDD group than in the non-PMDD group (P < 0.001) except for BMI.

Table 4
Statistical analysis with independent t-tests to compare the average of BMI, emotional eating, PMS, and negative perceived stress between the 2 groups
The values are presented as mean ± standard deviations. The Emotional Eater Questionnaire was used to measure the degree of emotional eating as a dependent variable. The Shortened Premenstrual Assessment Form was used to measure the degree of PMS/PMDD as an independent variable. The Negative Perceived Stress Scale was used to measure the degree of negative perceived stress as a mediator; The values of all 3 measurements are scores.
PMDD, premenstrual dysphoric disorder; BMI, body mass index; PMS, premenstrual syndrome.
***P < 0.001.
![]()
Mediation analysis
The mediating effect of negative perceived stress on the relationship between PMS and emotional eating was analyzed. Bias-corrected bootstrapping using PROCESS macro version 4.0 yielded 5,000 bootstrap estimates, which does not rely on the assumption of normal sample distribution [29].
In the mediation analysis in which 10 items for PMS (PMS-10) were considered independent variables, the effect of negative perceived stress on emotional eating in the PMDD group was statistically significant (β = 0.33; standard error [SE] = 0.07; 95% confidence interval [CI], 0.18–0.47; P < 0.001). The effects of PMS on negative perceived stress (β = 0.15; SE = 0.03; 95% CI, 0.09–0.21; P < 0.001) and PMS on emotional eating (β = 0.11; SE = 0.04; 95% CI, 0.03–0.19; P < 0.01) were significant in the PMDD group. In addition, the indirect effect of PMS on emotional eating, which was mediated by negative perceived stress, was significant in the PMDD group (β = 0.05; Boot SE = 0.02; 95% CI, 0.02–0.09).
For the non-PMDD group, when PMS-10 was an independent variable, although negative perceived stress was a significant factor in emotional eating (β = 0.33; SE = 0.11; 95% CI, 0.11–0.55; P < 0.01), PMS was not a significant factor for both negative perceived stress and emotional eating. In addition, there was zero (0) between the lower level of the confidence interval and the upper level of the confidence interval, indicating no significant indirect effect of negative perceived stress on the relationship between PMS and emotional eating according to Hayes [29]. The results of the mediation analysis are presented in Table 5.
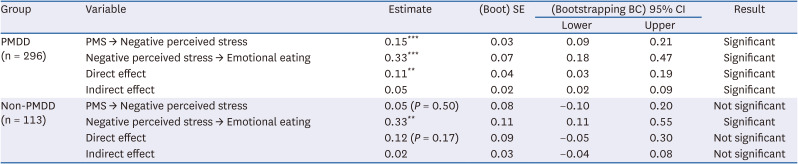
Table 5
Mediation effect of PMS on emotional eating via negative perceived stress (PMS as an independent variable)
Emotional eating was measured by the Emotional Eater Questionnaire. PMS was measured by the SPAF. Negative perceived stress was measured by the Negative Perceived Stress Scale. The groups were divided according to a cut-off score of 27 on the SPAF.
PMS, premenstrual syndrome; PMDD, premenstrual dysphoric disorder; SE, standard error; BC, bias-corrected; CI, confidence interval; SPAF, Shortened Premenstrual Assessment Form.
**P < 0.01; ***P < 0.001.
![]()
With regard to the results of the mediation analysis with affective factors of PMS (PMS-4) as an independent variable, the effects of PMS on negative perceived stress (β = 0.43; Boot SE = 0.05; 95% CI, 0.33–0.54; P < 0.001), and those of negative perceived stress on emotional eating (β = 0.33; Boot SE = 0.08; 95% CI, 0.17–0.48; P < 0.001) were significant, but a direct effect of PMS on emotional eating was not significant in the PMDD group (Table 6). In the non-PMDD group, when PMS-4 was the independent variable, the relationship model among PMS, negative perceived stress, and emotional eating was the same as the model when the independent variable was PMS-10 which only negative perceived stress affected emotional eating (β = 0.34; Boot SE = 0.11; 95% CI, 0.12–0.55; P < 0.01).
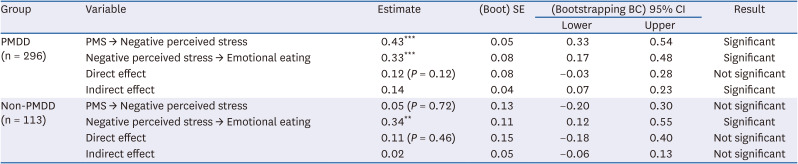
Table 6
Mediation effect of PMS on emotional eating via negative perceived stress (affective factors of PMS as an independent variable)
Emotional eating was measured by the Emotional Eater Questionnaire. PMS was measured by the SPAF. Negative perceived stress was measured by the Negative Perceived Stress Scale. The groups were divided according to cut-off scores of 27 on the SPAF.
PMS, premenstrual syndrome; PMDD, premenstrual dysphoric disorder; SE, standard error; BC, bias-corrected; CI, confidence interval; SPAF, Shortened Premenstrual Assessment Form.
**P < 0.01; ***P < 0.001.
![]()
Consequently, in the mediation analyses in the PMDD group, there was an indirect effect for both occasions in which PMS-10 and PMS-4 were established as independent variables. However, there was a partial mediating effect on PMS-10 and a complete mediating effect on PMS-4. Furthermore, the estimates analyzed by PMS-4 showed higher values than the estimates when PMS-10 was used as an independent variable. The comparison results of the mediation analysis are shown in Fig. 1.
 | Fig. 1Models of the relationship among emotional eating, PMS, and negative perceived stress depending on independent variables between the 2 groups.PMS-10 contains 10 items of the SPAF covering overall symptoms of PMS; PMS-4 contains 4 items (affective factors) of the SPAF covering only affective factor of PMS. The groups were divided according to a cut-off score of 27 on the SPAF.
→: Significant; --->: Not significant.
PMDD, premenstrual dysphoric disorder; SPAF, Shortened Premenstrual Assessment Form; PMS, premenstrual syndrome; ns, not significant.
**P < 0.01; ***P < 0.001.
|
Go to :
DISCUSSION
In the measurement of the SPAF, item SPAF-7 (“during the premenstrual period, breast pain, enlargement or swelling are present”) belonged to the water retention subfactor in the study by Allen et al. [24], but in the study Lee et al. [19], it belonged to the pain subfactor, which was maintained in this study. This can be explained because item SPAF-7 has both pain and water retention characteristics.
The PMDD group, which included individuals who suffered from PMS, had higher PMS scores and greater average scores for negative perceived stress and emotional eating than the non-PMDD group. The statistically significant difference in emotional eating and negative perceived stress between the PMDD and non-PMDD groups can be interpreted as follows: PMS has an impact on women’s psychological and physical wellbeing in a negative way. The fact that there was no significant difference in BMI between the 2 groups implies that women in any BMI range can go through PMS and might consider managing it if it appears.
As is already well known from previous studies, stress is a cause of emotional eating [30]. The results of this study verified this theory, as the effect of negative perceived stress (mediator) on emotional eating (dependent variable) was significant for both groups. However, the effect of PMS on negative perceived stress was only significant for the PMDD group in this study. This could be because the non-PMDD group had no, mild, or less PMS symptoms than the PMDD group, which might not have caused significantly meaningful stress. PMS had a relationship with emotional eating only in the PMDD group. An indirect effect was also significant only for the PMDD group. Moreover, the fact that there was full mediation when PMS-4 was the independent variable but partial mediation when PMS-10 was the independent variable supports the findings of a previous study that affective factors of PMS best explain PMS and suggests how important it is to manage affective factors to avoid causing emotional eating.
PMS occurs for some women in the luteal phase of the menstrual cycle and has a negative effect on emotional status and eating behavior. The reason PMS did not affect emotional status and eating behavior in the non-PMDD group could be because these individuals do not consider PMS to be intense stress. On the other hand, for the PMDD group, the reason PMS may affect emotional status and eating behavior is that these individuals consider PMS to be stressful. The fact that the effect of affective factors of PMS on emotional eating was fully mediated by negative perceived stress supports the importance of strategies to minimize the stress caused by PMS. Therefore, both strategies are needed to prevent PMS from becoming a severe state and to minimize the acceptance of PMS as stress even if it occurs. In summary, PMS might be regarded as a risk factor for stress and emotional eating, which further disturbs women’s healthy lives.
This study found that emotional eating was affected by PMS in the PMDD group. The PMDD and non-PMDD groups had a different relationship models for the 3 variables. Our study evaluated overall eating behaviors (i.e., emotional eating) and stress (i.e., negative emotions), unlike previous studies that considered highly sweet or fatty foods, irritability, or anxiety [1617]. Thus, it has the advantage of being able to grasp the relationship between variables from a significant perspective. However, because emotional eating is affected by various factors, further study to find covariates is needed. Furthermore, future studies should examine the relationship between specific factors constituting each measurement as it is important to understand the population’s eating behavior in more detail.
In conclusion, the main research topic of this study was to investigate the association among emotional eating, PMS, and negative perceived stress and the differences between a PMDD and non-PMDD group. PMS and negative perceived stress had a significant effect on emotional eating only in the PMDD group. Furthermore, in the PMDD group, emotional eating was fully mediated by negative perceived stress among affective factors of PMS. Women experiencing decades of menstrual cycles will be able to address emotional eating behavior by efficiently coping with the negative cognitive stress caused by PMS as well as PMS during the menstrual cycle. Further studies about ways of controlling eating behavior during PMS may be beneficial.
Go to :
 XML Download
XML Download