

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Malnutrition represents the nutritional status which includes both overnutrition and undernutrition, although in literature it is frequently used to describe undernutrition [1]. Malnutrition occurs due to complex processes in health conditions and impacts changes in the composition and function of the body [12]. A patient may suffer from malnutrition before or during hospitalization, which is related to increased cost of care, increased morbidity (including increased rates of infections and complications), impaired wound healing, decreased function and quality of life, and prolonged hospitalization [234]. A previous study by Hill [5] found a decrease in muscle strength and respiratory function in patients who had lost 15% of body weight during hospitalization. Furthermore, a meta-analysis by De Stefani et al. [6] showed increased all-cause mortality in patients with unintentional weight loss. These findings highlight the importance of early screening of malnutrition risk in hospitalized patients [2].
The prevalence of in-hospital malnutrition in Indonesia varies between 23.9% to 60.5% [78910]. These might be due to variability in the patient population as well as the parameters used. In-hospital malnutrition might be caused by individual and/or institutional factors. Individual factors are preexisting factors of the patient, while institutional factors are factors attained from the healthcare facility. Malnutrition due to institutional factors is also known as iatrogenic malnutrition [111]. Deficiency in daily intake, impaired absorption-metabolism, increased nutritional demands, and increased expenditure of nutrients are the main factors associated with in-hospital malnutrition [12].
To the best of our knowledge, there is no sufficient study involving in-hospital malnutrition in Indonesia. Most available studies are restricted to a limited part of nutritional status [81314] and lack the overall clinical aspects that might be causing in-hospital malnutrition [71015]. While our previous study focused on assessing risk factors contributing to undernutrition at admission [16], the purpose of this study is to determine the impact of various clinical factors to in-hospital malnutrition, measured by weight loss during hospitalization in adult patients, that had not been assessed in previous studies (such as malnutrition at admission, immobilization, depression, polypharmacy, inflammation, comorbidity, and length of hospitalization). Outcomes from this study will provide insights on which clinical factors need to be evaluated in hospitalized patients to screen in-hospital malnutrition risk, thereby eventually preventing unintentional weight loss and better clinical outcomes.
SUBJECTS AND METHODS
Data collection and study participants
This study was an advanced study in continuation to our previous published study [16]. This was a prospective study conducted by enrolling newly hospitalized patients at the Dr. Cipto Mangunkusumo National General Hospital, Indonesia. All patients aged 18–59 yrs were eligible for the study. The exclusion criteria were unconscious patients, patients with clinical or radiological excess fluid problems, patients hospitalized for elective procedures, patients with a history of corticosteroid and immunosuppressant use, patients with HIV/AIDS and hematological malignancies, post-chemoradiation patients, and febrile neutropenia. The drop out criteria were patients who had clinical fluid accumulation during hospitalization as well as patients who did not complete the entire study. This study was approved by the Clinical Research Ethics Committee of the Faculty of Medicine Universitas Indonesia (IRB approval number KET-389/UN2.F1/ETIK/PPM.00.02/2019). All participants signed a written informed consent before participating in the study.
Measurements
Body weight was measured on admission and before being discharged using the Electronic Bed Scale Sung Sim® E543-040 series. Knee-height was measured on admission using the knee-height caliper and was converted to body height using the Paramita knee-height conversion formula [17]. Food intake during hospitalization was monitored daily using the food weighing method for hospital meals and food record for out-hospital meals. Food intake was translated into energy intake by applying the Nutrisurvey® 2007. In this study, malnutrition at admission was defined as body mass index (BMI) < 18.5 kg/m2. Depression was assessed using the Beck Depression Inventory (BDI)-II Indonesia [18], and polypharmacy was defined as ≥ 5 drugs prescribed during hospitalization. The inflammatory status was classified using the neutrophil-lymphocyte ratio (NLR), which was calculated by dividing neutrophil count with lymphocyte count from the white blood cell differential count. Comorbidity status was determined using the Charlson Comorbidity Index (CCI).
Statistical analysis
Sample size was calculated by applying the formula for mean difference between two groups with significance level α = 0.05, power 80%, and mean difference of 2.5 kg weight change. The minimum sample size calculated for this study was 30. Statistical analysis was carried out using the Statistical Product for Social Science (SPSS) version 20.0 (IBM Corp., Armonk, NY, USA). Multivariate analysis with multiple linear regression was performed on variables with P < 0.25 in the bivariate analysis using the enter method. The results are considered statistically significant if P < 0.05.
RESULTS
Subject characteristics
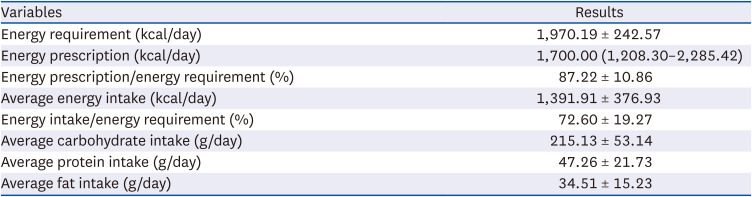
There were 60 study participants recruited between July and September 2019. Of these, 5 study participants dropped out of the study and the remaining 55 subjects were included in the final analysis. The median age of subjects was 39 (18–59) yrs with a median length of stay of 6 (3–14) days. Table 1 shows the characteristics of the research participants included in this study. More than half the subjects were men. Malnutrition at admission was found in almost one-third of the subjects and almost half were hospitalized due to acute gastrointestinal diseases, as mentioned in our previous publication [16]. More than half the subjects experienced gastrointestinal symptoms on admission. The mean caloric intake of subjects during hospitalization was 1,391.91 ± 376.93 kcal/day with the average percentage of energy intake being 72.60 ± 19.27% (Table 2). The mean daily energy requirement of subjects was 1,970.19 ± 242.57 kcal/day, while the specialists´ prescription was 1,700 (1,208.30–2,285.42) kcal/day (Wilcoxon test, P < 0.001).
Table 1
Characteristics of the research participants
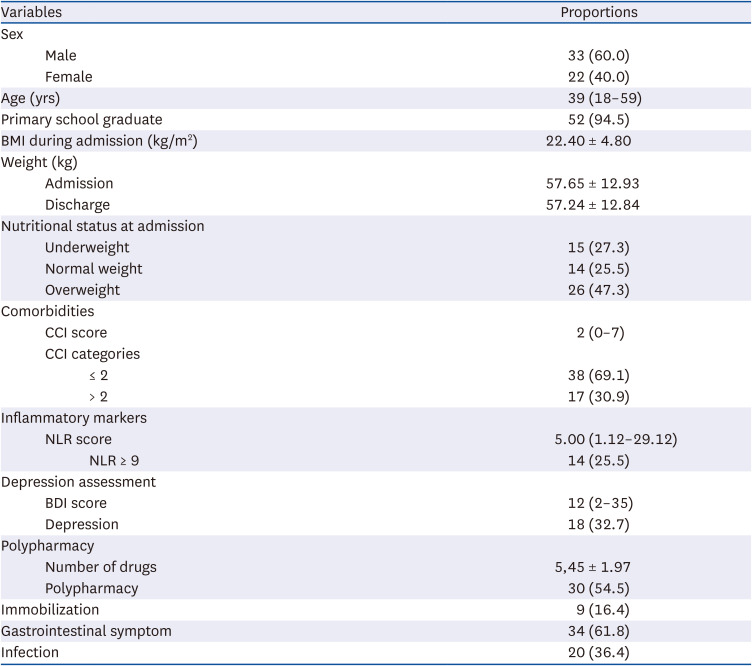
Table 2
Energy balance and dietary intake of study subjects
In-hospital weight loss
As many as 50.9% of the subjects experienced weight loss. The mean weight loss was 0.41 kg (P = 0.038). The results of the subgroup analysis based on length of stay showed that subjects with a length of stay ≥ 7 days experienced more weight loss with a mean difference of 1.21 kg and P-value of 0.009 (Table 3). Subgroup analysis based on fasting during hospitalization showed that more weight loss occurred in subjects fasting due to illness, with a mean difference of 0.7 kg, compared to fasting prior to intervention and not fasting groups which were 0.36 and 0.34 kg weight loss, respectively. However, analysis based on fasting status was not statistically significant for affecting in-hospital weight loss (Table 4).
Table 3
Weight change based on length of stay

Table 4
Weight loss of research participants during hospitalization

Factors associated with in-hospital weight loss
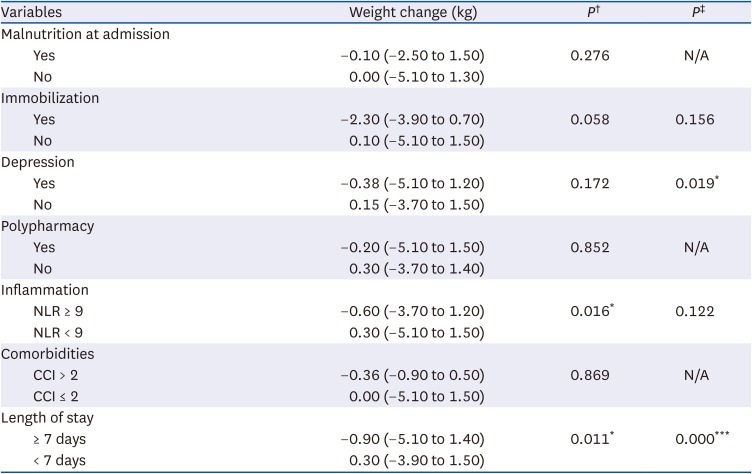
Bivariate analysis was done to compare in-hospital weight change and the presence of malnutrition at admission, immobilization, depression, polypharmacy, inflammation, comorbidities, and length of stay (Table 5). Inflammation status (P = 0.016) and length of stay (P = 0.011) were significantly associated with weight change. Variables with P-values < 0.25 were included in multivariate analysis (presence of immobilization, depression, inflammation, and length of stay). Multivariate analysis showed that inflammation status became statistically not significant (P = 0.122), whereas length of stay remained significant (P < 0.001) and depression became significant (P = 0.019) in association with weight change. These results indicate that the inflammation status (NLR > 9) might not directly influence weight loss, but length of stay (≥ 7 days) and presence of depression were independent risk factors for weight loss during hospitalization.
Table 5
Analysis of factors affecting weight changes during hospitalization
DISCUSSION
Most subjects in this study (84%) retained active mobility during hospitalization as the CCI score predominantly remained ≤ 2. This indicates that our research participants were hospitalized patients with relatively stable clinical conditions and minimal comorbidities. The average length of stay in this study was 6 (3–14) days. This finding was different from previous studies [8910] conducted in different hospitals where most subjects spent more than 7 days in the hospital. This might be due to the targeted length of stay policy in our hospital. Our study determined that 50.9% of the research participants experienced weight loss during hospitalization, which was consistent with a previous study [10].
In the current study, the mean weight loss was determined to be 0.41 kg during hospitalization (P = 0.038). Further analysis revealed that this in-hospital weight loss was observed among patients who were hospitalized for ≥ 7 days (1.21 kg; P = 0.009), while patients hospitalized for < 7 days showed no weight loss. A previous study of 42 subjects [19] reported a weight loss of 0.31 kg (P = 0.016) and also found no significant weight loss in patients who were hospitalized for < 7 days. A study in Canada [20] showed 1.1 kg of median weight loss during hospitalization, in which the patients had a length of stay of 11 days. Another study [13] described a mean weight loss of 0.76 kg (P = 0.013) in patients who were hospitalized for two weeks. This indicates that the effect of length of stay on weight loss generally occurs after 7 days of hospitalization.
A greater weight loss was observed in the study from Canada compared to our study probably due to the older population recruited (68 yrs), more comorbidities (46.4% patients with CCI > 2), more drugs received (13 drugs), and longer length of stay (11 days). A study from Vietnam reported weight loss of 2 kg in all hospitalized subjects. These differences in results as compared to our study might arise due to the different population recruited, as the study from Vietnam recruited gastrointestinal surgical patients of which 72% patients had malignancies and 48% already had malnutrition at admission [21]. The reimbursement system of a country plays a role in clinical nutrition support, especially in terms of the use of enteral and parenteral nutrition at hospitals. The proportion of patients receiving parenteral nutrition in the lower middle-income countries (including Indonesia) is significantly much lower compared to patients in high-income countries such as South Korea, Japan, and Australia [22]. Although the economy did not seem to principally affect the differences in clinical nutrition services between countries, more studies are required to help conclude this matter.
The increased length of stay correlated with increased in-hospital complications (i.e., infection, pressure ulcer), decreased food intake (procedure-related dietary restriction, underlying disease, or medication side effect), and increased inflammation that would lead to increased weight loss during hospitalization [323]. This is supported by a systematic review [24] that showed increased malnutrition in five longitudinal studies with a prevalence of more than 80% individuals who were hospitalized in 2 weeks. Our study found that length of stay ≥ 7 days is associated with weight loss during hospitalization (−1.21 kg vs. 0.003 kg). A study by Allard et al. [20] reported that as many as 25% individuals experienced weight loss of more than 5% during hospitalization which was associated with the length of stay. Kusumayanti et al. [8] reported that patients who were hospitalized for more than 7 days had an increased risk of malnutrition (as much as 8-fold) during hospitalization.
The mean energy intake of subjects in this study was 72.6% of the daily requirements. This is because almost half of our patients were hospitalized due to acute gastrointestinal diseases (gastrointestinal bleeding, gallbladder infection, or obstructive jaundice) and more than half the patients experienced gastrointestinal symptoms on admission. Moreover, as many as 62% of the subjects also fasted, both as part of the management of the disease as well as a part of the preparation for medical intervention. This can be seen from the significant difference in the percentage of energy intake between subjects who fasted during hospitalization (67.1%) compared to subjects who did not fast (81.6%) during hospitalization (P = 0.006). A study conducted on 30 hospitalized patients [13] presented that patients with malnutrition at admission consumed 70% of the daily required energy intake, whereas patients who are well-nourished at admission consumed 76.8% of the daily required energy intake during hospitalization. However, this study did not carry out a nutritional assessment at admission for most patients. We also found that the total energy intake prescription from specialists was lower than the actual required energy (1,700 vs. 1,970.2 kcal/day; P < 0.001). This is because clinical conditions of the patients are considered before prescribing energy intake. Patients admitted due to acute gastrointestinal disorders, such as gastrointestinal bleeding, need a gradual increase in energy intake until the daily requirement is fulfilled [25]. In addition, limitation of the energy that can be delivered by parenteral nutrition by as much as 50% of daily energy needs in the first 24–48 hours might contribute to an accumulation of energy intake deficits [26].
Fasting during hospitalization correlated with weight loss. Grouping of patients based on their fasting status showed that patients who were required to fast as a part of their medical treatment had a higher trend of weight loss as compared to those who fasted as a part of medical intervention preparation and those who did not fast (0.70, 0.36, and 0.34 kg, respectively). The weight loss comparison between participants based on fasting did not show statistical significance. Individuals who fasted as a part of medical intervention usually missed one mealtime (6–8 hours), and hence energy deficits could be compensated with the next mealtime. However, individuals who fasted as a part of their medical treatment, such as due to a dysfunctional gastrointestinal tract, usually missed more meals.
In-hospital weight loss has multifactorial causes, with inflammation being the most common etiology. In the current study, we observed that individuals with severe inflammation (NLR ≥ 9) experienced 0.6 kg weight loss whereas individuals without severe inflammation experienced 0.3 kg weight loss (P = 0.016). Several mechanisms might contribute to inflammation-related weight loss, such as decreased appetite due to the release of proinflammatory cytokines, increased basal metabolism, increased energy-protein needs, and increased catabolism as an acute response phase [27]. Increased catabolism in the presence of proinflammatory cytokines such as tumor necrosis factor (TNF)-α, interleukin (IL)-1 and IL-6 results from increased lipolysis, inhibition of triglyceride synthesis, suppression of the insulin signaling pathway, and suppression of peroxisome proliferator-activated receptor γ activity in adipocytes [28]. Decreased appetite and increased energy expenditure are mediated by the promotion of GLP-1 secretion and leptin expression induction as responses to the presence of proinflammatory cytokines [28]. Higher NLR has been correlated with the degree of inflammation [29]. The value of NLR ≥ 5 suggests infection and sepsis, while NLR ≥ 9 describes severe sepsis [30].
Individuals with depression experience weight loss due to several mechanisms. Depression can cause low mood, loss of energy, fatigue, and decreased appetite, all of which can lead to reduced food intake. Depression can also cause activation of the immune system that results in increased proinflammatory cytokines such as IL-6, TNF, and TNF soluble receptors [273132]. Our study found that depression at admission promotes weight loss during hospitalization (−0.38 vs. 0.15 kg). To date, no study has assessed the correlation between depression and in-hospital weight loss. A study with more than 800 patients [23] reported a strong association between depressive symptoms and malnutrition during admission. A previous study in Indonesia [14] stated that malnutrition risk increased almost 11-times in hospitalized geriatric patients who experienced depression.
Theoretically, malnutrition at admission can cause in-hospital weight loss through indirect mechanisms. Patients with malnutrition at admission will have a longer length of stay and more complications during hospitalization (pneumonia, infection, and gastrointestinal bleeding) [3334]. However, we found no association between malnutrition at admission with in-hospital weight loss. A previous study by Susetyowati et al. [7] found an increase in the relative risk of in-hospital weight loss by 7-fold among patients with malnutrition at admission. This difference might be due to the difference in study participants; the subjects in the Susetyowati study were patients with malignancy who had minimum 2-weeks of hospitalization, while our study participants were more general with a median length of stay of 6 days. In addition, the former study assessed nutritional status by using PG-SGA, whereas individuals in our study were assessed by their BMI.
Immobilization causes decreased secretion of the growth hormone which leads to decrease muscle mass and function. This condition further causes sarcopenia which, in turn, alters the body metabolism. Immobilization also decreases the patient’s daily intake due to swallowing difficulty and the patient’s dependency. Lastly, immobilization may cause increased in-hospital complications such as pressure ulcer, pneumonia, and urinary tract infection which lead to inflammation [353637]. Our study found a trend of weight loss in immobilized compared to non-immobilized subjects (2.3 kg of weight loss versus 0.1 kg of weight gain, respectively). However, it did not reach statistical significance. This might be probably due to the proportion of our immobilized subjects, which was merely 16% of the total subjects.
The strength of this study is in its comprehensiveness for assessing the effect of various clinical factors on in-hospital weight loss. The prospective cohort design shows the causality relationship better than a cross-sectional study. The limitation of this study is in the limited patients’ spectrum due to strict inclusion and exclusion criteria, although considered necessary.
In conclusion, we observed a mean weight loss of 0.41 kg during hospitalization in adult patients. Length of stay and depression were determined to be independent risk factors for weight loss during treatment.
 XML Download
XML Download