

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Obesity is one of the world’s major epidemic challenges. The global prevalence of obesity approximately tripled between 1975 and 2016 [1]. Adult obesity has been associated with various complications such as cardiovascular disease, type 2 diabetes mellitus, coronary heart disease, certain types of cancer, and obstructive sleep apnea [2]. Obesity is a multifactorial disease affected by: (1) dietary factors (e.g., energy intake that exceeds energy needs, high consumption of calorie-dense, nutrient-poor food); (2) low physical activity; and (3) unhealthy psychological conditions (e.g., depression, stress) [3]. Although high energy intake is the major factor leading to obesity, evidence is emerging that high sodium intake leads to additional weight gain in adults [456]. Therefore, research is needed to systematically review individual studies and examine associations between dietary sodium intake and obesity.
Multiple methods were utilized to estimate dietary sodium intake, such as dietary methods, 24-h urine, spot urine, and overnight urine. While 24-h urine collection is considered the gold standard for assessing dietary sodium intake, the studies often employed other methods that were less time-consuming or burdensome. However, these other methods are known to be less accurate with regard to reflecting the sodium intake of individuals [7]. Some methods of measuring dietary sodium intake could underestimate or overestimate obesity outcomes. Consequently, it is critical to determine how sodium intake methods could differ when it comes to associations between dietary sodium intake and obesity.
We conducted a review of systematic reviews to identify and synthesize the scientific evidence regarding the association between dietary sodium intake and obesity in adults. Additionally, we performed subgroup analyses of primary studies in the included systematic reviews to examine whether the association of sodium and obesity differs by dietary sodium intake assessment method.
SUBJECTS AND METHODS
Data sources and searches
The search strategy was developed based on a protocol of the earlier systematic review [8]. We conducted the data searches for systematic reviews with or without meta-analysis in the PubMed database (from inception to October 24, 2022) (Supplementary Table 1). Obesity-related outcomes were included in the search terms, such as body mass index (BMI), body weight, waist circumference, and abdominal obesity.
Study eligibility criteria
We included systematic reviews with randomized controlled trials (RCTs) and observational studies. To be included, systematic reviews had to contain information about adult subjects (over 18 yrs). Additionally, systematic reviews had to include dietary sodium intake with a quantitative assessment and different levels of sodium intake or compare the effect of dietary sodium intake based on different levels of intake. Systematic reviews describing a dietary pattern/index indicating a higher intake of sodium, but not indicating the specific levels of sodium intake, were ineligible. Systematic reviews had to have reported outcomes related to obesity (i.e., BMI, body weight, risk of overweight/obesity or abdominal obesity, and waist circumference). Finally, we included systematic reviews with or without meta-analysis, but excluded literature reviews, critical reviews, and review of systematic reviews.
Study selection process
Two researchers independently screened the abstract of all citations according to the established inclusion and exclusion criteria. To conduct the abstract screening, 2 researchers used the online software Abstrackr separately. Then, 2 researchers independently implemented the full-text screening according to the study eligibility criteria.
Data extraction and study quality assessment
We employed the Risk of Bias in Systematic Reviews (ROBIS) tool to assess the quality of the included systematic reviews. The ROBIS tool involves the assessment of 4 domains: study eligibility criteria; identification and selection of studies; data collection and study appraisal; and synthesis and findings [9]. Finally, an overall evaluation was rated as low, unclear, or high by considering the following issues: the interpretation of findings addressed all the concerns identified in the above domains; the relevance of the included studies to the review’s research question; and the emphasizing of the results based on statistical significance. The risk of bias of each systematic review was independently evaluated by 2 researchers. Any discrepancies were resolved by discussion.
Quantitative synthesis
We performed re-meta-analyses of the individual studies included in the earlier systematic reviews to examine the association between dietary sodium and obesity. Due to significant clinical and methodological heterogeneity (e.g., various levels of sodium intake, different characteristics of participants), we used a random effects model for the meta-analyses. To examine the degree of statistical heterogeneity, we utilized the I2 index. The cut-off values were 25% for low, 50% for moderate, and 75% for high heterogeneity for the descriptive purpose [10]. Meta-analyses were conducted in STATA/SE 17 (Stata Corp., College Station, TX, USA). Less than 0.05 of 2-tailed P-values were considered statistically significant.
RESULTS
Characteristics of individual reviews
The initial search generated 1,069 citations. Then, we conducted the abstract screening and selected 21 possibly relevant articles for full-text screening. Finally, we selected 3 systematic reviews (2 systematic reviews with meta-analyses and 1 systematic review without meta-analysis) that met the inclusion criteria. The study selection process is shown in Fig. 1. Included 3 systematic reviews were published between 2016 and 2021 [111213]. Table 1 shows a summary of review characteristics. One systematic review included RCTs and observational studies [11], while 2 systematic reviews included only observational studies [1213]. Moosavian et al. [12] performed a meta-analysis of studies with the inclusion of both children and adults, while Grimes et al. [11] implemented a meta-analysis among children and adults separately [11]. Because the specific aim of this study was to investigate the association between sodium intake and adiposity outcomes across sodium intake assessments, we analyzed subgroup analyses with the use of the individual studies only in adults included in the past 2 systematic reviews [1112]. The risk of bias for observational studies was evaluated by a modified version of the Newcastle-Ottawa Scale in the included 2 systematic reviews [1112]. The risk of bias for RCTs was evaluated using a modified version of the Cochrane Collaboration in one systematic review [11]. However, the remaining systematic review did not include information related to the risk of bias for the included studies [13].
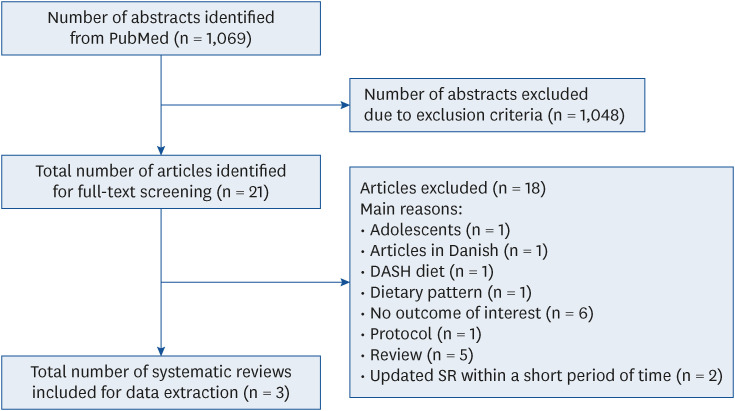
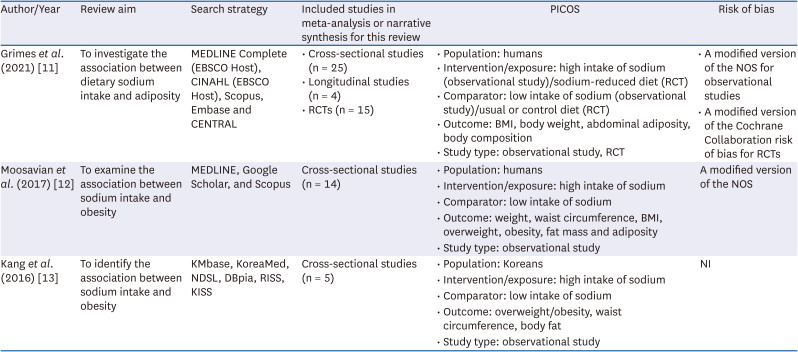
Fig. 1
Literature search and study selection process.
DASH, Dietary Approaches to Stop Hypertension; SR, systematic review.
![]()
Table 1
Characteristics of individual reviews
| Author/Year | Review aim | Search strategy | Included studies in meta-analysis or narrative synthesis for this review | PICOS | Risk of bias |
|---|---|---|---|---|---|
| Grimes et al. (2021) [11] | To investigate the association between dietary sodium intake and adiposity | MEDLINE Complete (EBSCO Host), CINAHL (EBSCO Host), Scopus, Embase and CENTRAL | • Cross-sectional studies (n = 25) | • Population: humans | • A modified version of the NOS for observational studies |
| • Longitudinal studies (n = 4) | • Intervention/exposure: high intake of sodium (observational study)/sodium-reduced diet (RCT) | • A modified version of the Cochrane Collaboration risk of bias for RCTs | |||
| • RCTs (n = 15) | • Comparator: low intake of sodium (observational study)/usual or control diet (RCT) | ||||
| • Outcome: BMI, body weight, abdominal adiposity, body composition | |||||
| • Study type: observational study, RCT | |||||
| Moosavian et al. (2017) [12] | To examine the association between sodium intake and obesity | MEDLINE, Google Scholar, and Scopus | Cross-sectional studies (n = 14) | • Population: humans | A modified version of the NOS |
| • Intervention/exposure: high intake of sodium | |||||
| • Comparator: low intake of sodium | |||||
| • Outcome: weight, waist circumference, BMI, overweight, obesity, fat mass and adiposity | |||||
| • Study type: observational study | |||||
| Kang et al. (2016) [13] | To identify the association between sodium intake and obesity | KMbase, KoreaMed, NDSL, DBpia, RISS, KISS | Cross-sectional studies (n = 5) | • Population: Koreans | NI |
| • Intervention/exposure: high intake of sodium | |||||
| • Comparator: low intake of sodium | |||||
| • Outcome: overweight/obesity, waist circumference, body fat | |||||
| • Study type: observational study |
PICOS, Population, Intervention/exposure, Comparator, Outcome, and Study type; NI, no information; RCT, randomized controlled trial; NOS, Newcastle-Ottawa Scale; BMI, body mass index; CINAHL, Cumulative Index to Nursing and Allied Health Literature; CENTRAL, Cochrane Central Register of Controlled Trials; NDSL, National Discovery for Science Library; RISS, Research Information Sharing Service; KISS, Korean Information Service System.
![]()
The results of the ROBIS evaluation are shown in Table 2. Regarding study eligibility criteria (domain 1), a clear definition of the search criteria revealed that all included systematic reviews were at low risk [1112]. However, concern regarding methods used to identify and select studies (domain 2) was considered by Kang et al. [13], who did not include methods beyond database searching to identify relevant studies [13]. In the domain of data collection (domain 3), 2 systematic reviews described sufficient study characteristics extracted by independent reviewers [1112], while the remaining systematic review was not reported with regard to this [13]. Because an adequate tool to assess the risk of bias was used in only 2 systematic reviews, Kang et al. [13] raised an additional concern regarding quality assessment for the included studies. Overall, one systematic review was rated as being at high risk of bias [13].

Table 2
Risk of bias using the Risk of Bias in Systematic Reviews tool
| Author/Year | Study eligibility criteria | Identification and selection of studies | Data collection and study appraisal | Synthesis and findings | Risk of bias in the review |
|---|---|---|---|---|---|
| Grimes et al. (2021) [11] | Low | Low | Low | Low | Low |
| Moosavian et al. (2017) [12] | Low | Low | Low | Low | Low |
| Kang et al. (2016) [13] | Low | High | High | NA1) | High |
NA, not applicable.
1)Because the population of interest was limited to Koreans, there were not enough studies to implement quantitative synthesis.
![]()
Meta-analysis findings
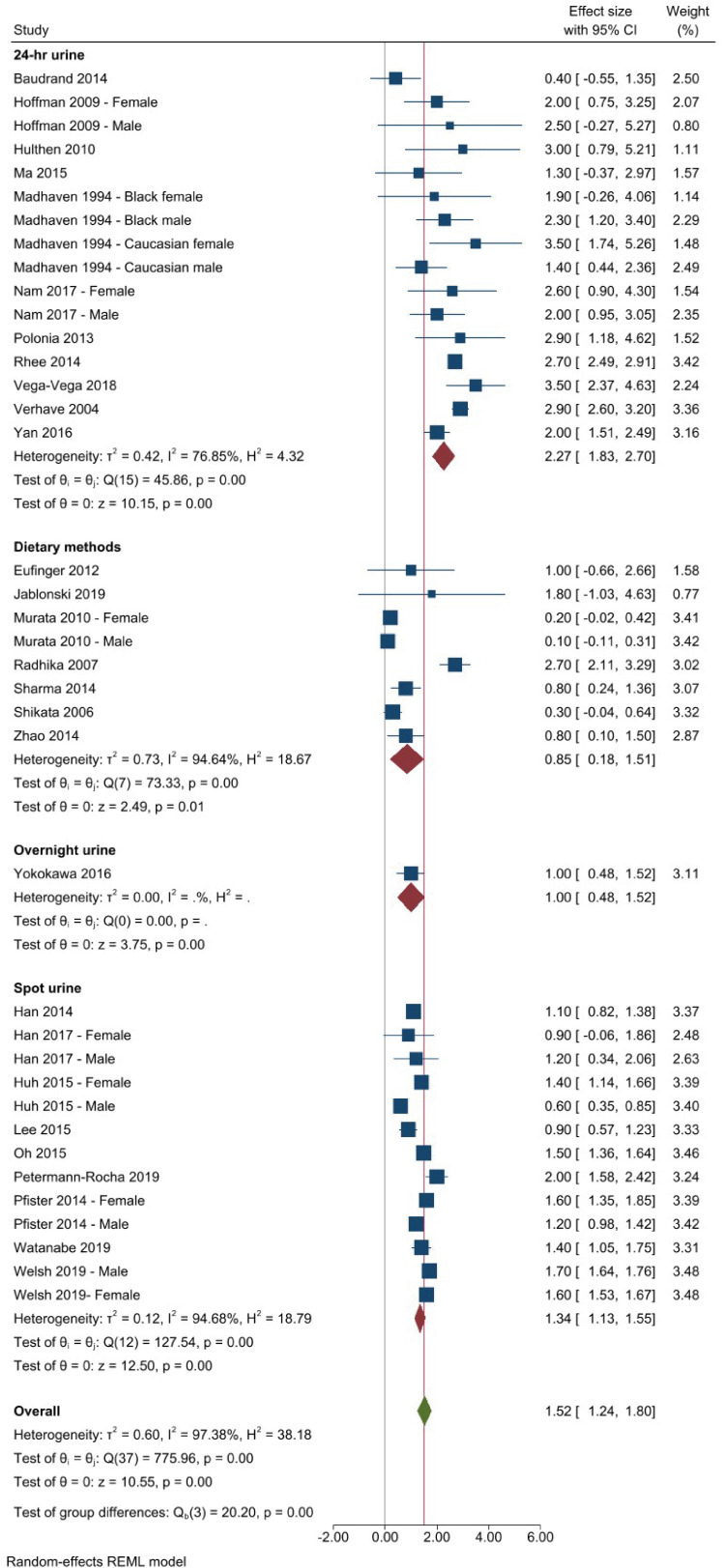
BMI: cross-sectional studies
We performed a subgroup analysis for 28 cross-sectional studies that reported an association between dietary sodium intake and BMI (Fig. 2). The included unique studies utilized: (1) 24-h urine in 11 studies [1415161718192021222324]; (2) spot urine in 9 studies [252627282930313233]; (3) dietary methods in 7 studies [34353637383940]; and (4) overnight urine in 1 study [41].The results from this pooled analysis (38 effect sizes) indicated that BMI was significantly greater among adults in the highest intake group of sodium compared to those in the lowest intake group of sodium (BMI mean difference = 1.52 kg/m2; 95% confidence interval [CI], 1.24–1.80; P < 0.001; I2 = 97%), presenting considerable heterogeneity. When we implemented the subgroup analysis by sodium intake assessment method, the greatest BMI was seen in studies that used 24-h urine to examine sodium intake (BMI mean difference = 2.27 kg/m2; 95% CI, 1.59–2.51; P < 0.001; I2 = 77%), followed by: (1) spot urine (BMI mean difference = 1.34 kg/m2; 95% CI, 1.13–1.55; P < 0;001; I2 = 95%); (2) overnight urine (BMI mean difference = 1.00 kg/m2; 95% CI, 0.48–1.52; P < 0.001); and (3) dietary methods (BMI mean difference = 0.85 kg/m2; 95% CI, 0.18–1.51; P < 0.05; I2 = 95%).
Risk of overweight/obesity: cross-sectional studies
We implemented a meta-analysis of 5 cross-sectional studies (8 effect sizes) (Fig. 3) [1926314243]. The findings from this pooled analysis show that higher sodium intake was significantly associated with an increased risk of overweight or obesity (odds ratio [OR], 1.75; 95% CI, 1.40–2.18, P < 0.001; I2 = 72%), presenting substantial heterogeneity. In a subgroup analysis by the sodium intake assessment, the risk of overweight/obesity was not significantly different across the group. A higher level of dietary sodium intake was significantly associated with a risk of overweight/obesity in studies that used the 24-h urine (OR, 2.44; 95% CI, 1.67–3.56; P < 0.001; I2 = 59%) [1942] and dietary methods (OR, 1.48; 95% CI, 1.17–1.88; P < 0.001; I2 = 16%) [43]. However, in studies that used spot urine, there was no association between dietary sodium intake and the risk of overweight/obesity [2631].

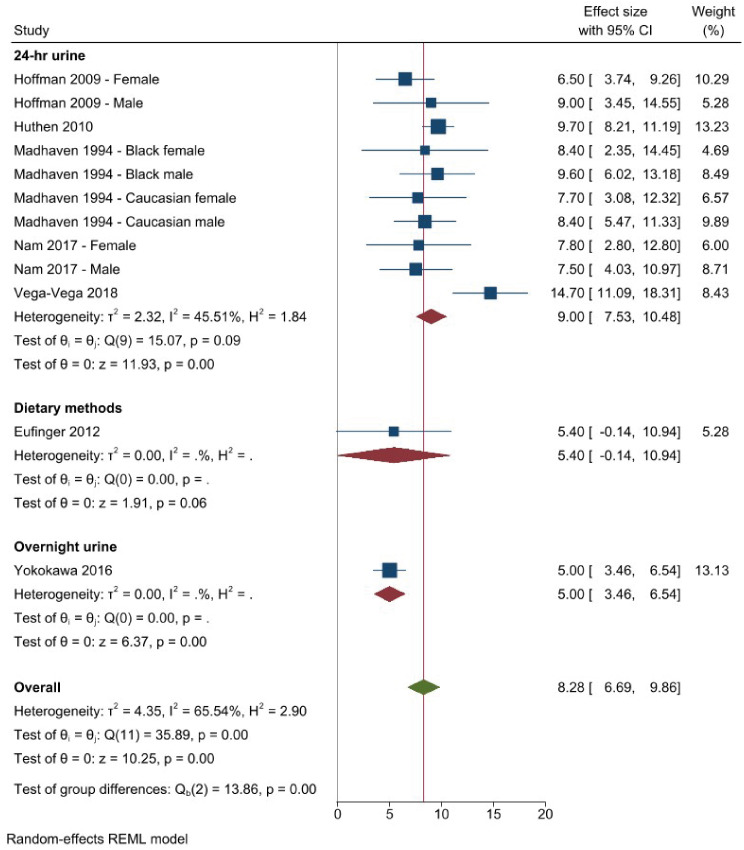
Body weight: cross-sectional studies
The findings from a meta-analysis of 7 cross-sectional studies (12 effect sizes) indicated that body weight was significantly greater among adults in the highest group of dietary sodium intake (body weight mean difference = 8.28 kg; 95% CI, 6.69–9.86; P < 0.001; I2 = 66%), presenting substantial heterogeneity (Fig. 4) [15161819213441]. The results of a subgroup analysis showed that body weight was greatest in studies that used 24-h urine (body weight mean difference = 9.00 kg; 95% CI, 7.53–10.48; P < 0.001; I2 = 46%) [1516181921], followed by those that used overnight urine (body weight mean difference = 5.00 kg; 95% CI, 3.46–6.54; P < 0.001) [41]. Studies that used dietary methods showed that there was an insignificant relationship between dietary salt intake and body weight [34].
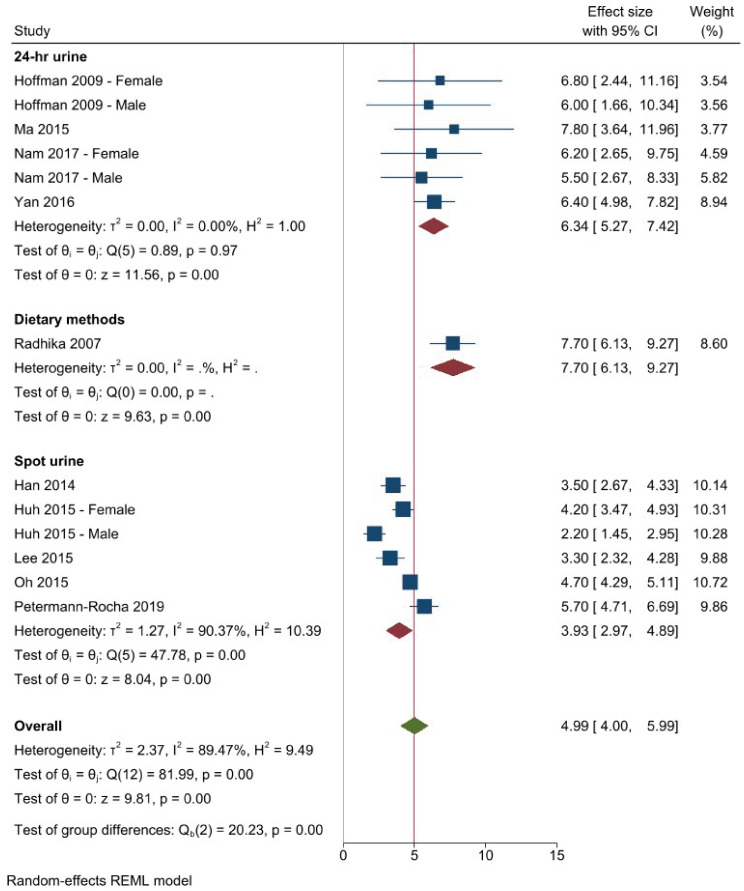
Waist circumference: cross-sectional studies
We performed a meta-analysis of 10 cross-sectional studies (13 effect sizes) (Fig. 5) [15171923252728293037]. The results of this meta-analysis showed that higher sodium intake was significantly associated with an increase in waist circumference (waist circumference mean difference = 4.99 cm; 95% CI, 4.00–5.99; P < 0.001; I2 = 89%), presenting considerable heterogeneity. In a subgroup analysis by sodium intake assessment, waist circumference was greater in studies that used 24-h urine (waist circumference mean difference = 6.34 cm; 95% CI, 5.27–7.42; P < 0.001; I2 = 0%) [15171923] compared to those that utilized spot urine (waist circumference mean difference = 3.93 cm; 95% CI, 2.97–4.89; P < 0.001; I2 = 90%) [25272829]. Additionally, one study utilizing the dietary method showed that higher sodium intake is significantly associated with greater waist circumference (waist circumference mean difference = 7.70 cm; 95% CI, 6.13–9.27; P < 0.001) [37].
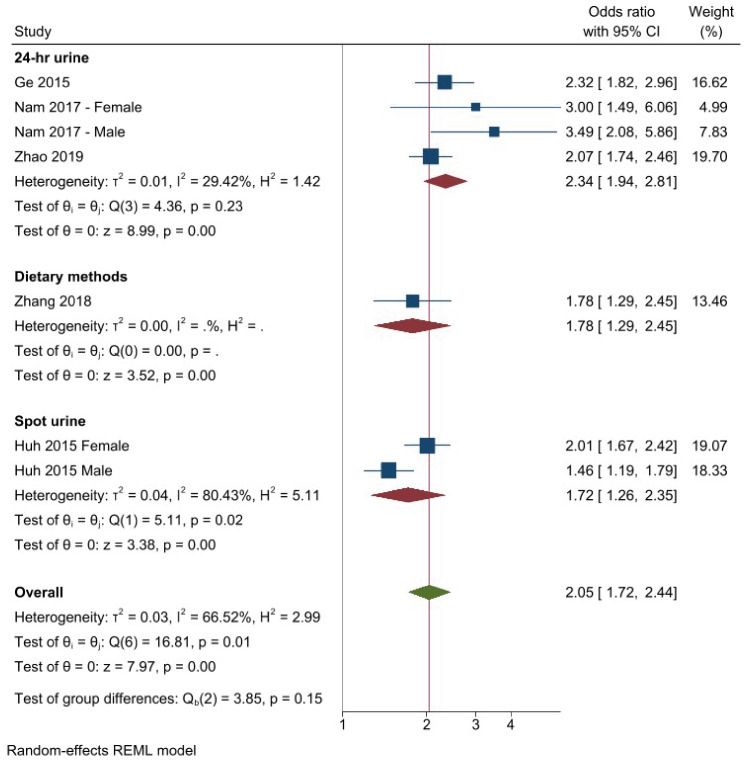
Abdominal obesity: cross-sectional studies
We employed a meta-analysis of 5 cross-sectional studies (7 effect sizes) to investigate the association between dietary sodium intake and abdominal obesity (Fig. 6) [1927424445]. The findings from this pooled analysis showed that higher sodium intake was significantly associated with an increased risk of abdominal obesity (OR, 2.05; 95% CI, 1.72–2.44; P < 0.001; I2 = 67%), presenting substantial heterogeneity. Subgroup analysis by sodium intake assessment showed that the association between dietary sodium intake and the risk of abdominal obesity was not significantly different among groups. There was a significant association between dietary sodium intake and the risk of abdominal obesity in all 3 groups: (1) 24-h urine (OR, 2.34; 95% CI, 1.94–2.81; P < 0.001; I2 = 29%) [194244]; (2) dietary methods (OR, 1.78; 95% CI, 1.29–2.45; P < 0.001) [45]; and (3) spot urine (OR, 1.72; 95% CI, 1.26–2.35; P < 0.001) [27].
Body weight: RCTs
The prior systematic review included 15 RCTs with durations ranging from 3 mon to 4 yrs. Included RCTs were conducted in various countries: (1) 4 in the USA; (2) 3 in the UK; (3) 3 in Australia; and (4) 1 in the Netherlands, 1 in Italy, 1 in Belgium, 1 in Japan, and 1 in China. Ten RCTs employed nutrition education or nutrition counseling and behavioral strategies to reduce sodium intake. Grimes et al. [11] performed a pooled analysis of RCTs to examine the effects of a reduced sodium diet on body weight. The findings of 15 RCTs reported that reduced-sodium diets compared to a usual diet or control diet showed non-significant effects on body weight [464748495051525354555657585960].
Narrative synthesis
Obesity-related outcomes: longitudinal studies
Grimes et al. [11] included 4 longitudinal studies to examine the association between dietary sodium intake and obesity outcomes. Four studies showed that higher sodium intake did not change body weight [4616263] (Table 3). One study indicated that higher sodium intake did not increase waist circumference [4]. However, higher sodium intake significantly increased body fat [4] but decreased fat free mass per a 100 mmol/d sodium increase [4].
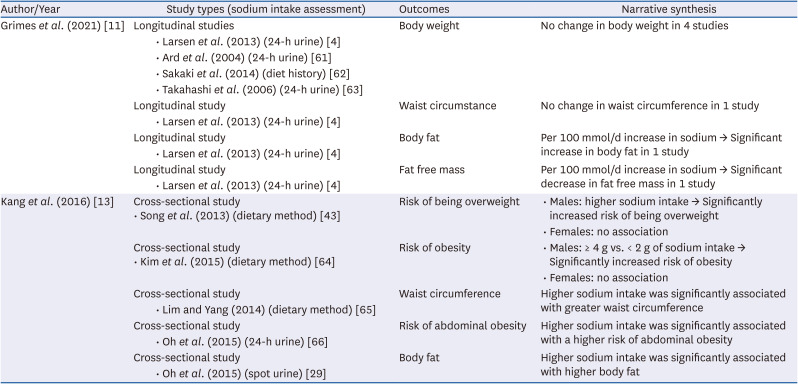
Table 3
Results of individual reviews that state a narrative synthesis for obesity-related outcomes
| Author/Year | Study types (sodium intake assessment) | Outcomes | Narrative synthesis | |
|---|---|---|---|---|
| Grimes et al. (2021) [11] | Longitudinal studies | Body weight | No change in body weight in 4 studies | |
| • Larsen et al. (2013) (24-h urine) [4] | ||||
| • Ard et al. (2004) (24-h urine) [61] | ||||
| • Sakaki et al. (2014) (diet history) [62] | ||||
| • Takahashi et al. (2006) (24-h urine) [63] | ||||
| Longitudinal study | Waist circumstance | No change in waist circumference in 1 study | ||
| • Larsen et al. (2013) (24-h urine) [4] | ||||
| Longitudinal study | Body fat | Per 100 mmol/d increase in sodium → Significant increase in body fat in 1 study | ||
| • Larsen et al. (2013) (24-h urine) [4] | ||||
| Longitudinal study | Fat free mass | Per 100 mmol/d increase in sodium → Significant decrease in fat free mass in 1 study | ||
| • Larsen et al. (2013) (24-h urine) [4] | ||||
| Kang et al. (2016) [13] | Cross-sectional study | Risk of being overweight | • Males: higher sodium intake → Significantly increased risk of being overweight | |
| • Song et al. (2013) (dietary method) [43] | • Females: no association | |||
| Cross-sectional study | Risk of obesity | • Males: ≥ 4 g vs. < 2 g of sodium intake → Significantly increased risk of obesity | ||
| • Kim et al. (2015) (dietary method) [64] | • Females: no association | |||
| Cross-sectional study | Waist circumference | Higher sodium intake was significantly associated with greater waist circumference | ||
| • Lim and Yang (2014) (dietary method) [65] | ||||
| Cross-sectional study | Risk of abdominal obesity | Higher sodium intake was significantly associated with a higher risk of abdominal obesity | ||
| • Oh et al. (2015) (24-h urine) [66] | ||||
| Cross-sectional study | Body fat | Higher sodium intake was significantly associated with higher body fat | ||
| • Oh et al. (2015) (spot urine) [29] | ||||
![]()
Obesity-related outcomes: a systematic review including only Korean studies
Kang et al. [13] included only Korean studies that examined the association between dietary sodium intake and obesity-related outcomes. Two studies suggested that higher sodium intake increased the risk of overweight/obesity in males but not in females [4364]. Higher sodium intake was significantly associated with: (1) greater waist circumference in one study [65]; (2) increased risk of abdominal obesity in one study [66]; and (3) increased body fat in one study [29].
DISCUSSION
The main findings from this review of systematic reviews and re-meta-analysis indicated consistently positive associations between dietary sodium intake and obesity-related outcomes in cross-sectional studies. Additionally, subgroup analyses showed that the associations between dietary sodium intake and obesity outcomes (i.e., BMI, body weight, and waist circumference) were significantly different across sodium intake assessments. Compared to studies utilizing 24-h urine collection, the other sodium intake assessments (spot or overnight urine and dietary methods) tend to underestimate the sodium-obesity association in cross-sectional studies. This review of the systematic reviews provides useful information to detect the difference in the association between sodium intake and obesity-related outcomes by sodium intake assessment.
The possible biological mechanisms could explain this positive association between dietary sodium intake and obesity. First, salt treatment increased adipogenesis/lipogenesis and pro-inflammatory adipocytokine secretion. However, it decreased lipolysis in a dose-dependent manner in adipocytes, suggesting inflammatory adipogenesis as a possible mechanism [67]. Second, endogenous fructose production was identified as the primary mechanism regarding salt-induced obesity in high-salt-fed mice [68]. High-salt-diet-fed rats were also associated with increased adipose tissue mass by enhancing insulin-stimulated glucose uptake and lipogenic capacity [6970]. Third, a high-salt diet (18 g/day) increased significantly fasting ghrelin levels compared to a normal salt diet (3 g/day) in normotensive subjects, indicating that increased ghrelin induced obesity by stimulating appetite, fat accumulation, and glucose intolerance [71]. In addition, increased salt intake (6 g/day) decreased significantly diet-induced thermogenesis compared to the placebo group, which contributes to increased weight gain [72].
To identify the association between sodium intake and obesity, it is critical to use a valid, reliable tool for assessing sodium intake. Twenty-four urine collection is known to be the gold standard method for the assessment of dietary sodium intake [7], as about 90% of ingested sodium is excreted in urine within 24 h [73]. Because participants would carry a considerable burden with 24-h urine collection, some researchers tend to utilize more convenient or affordable alternatives such as spot or overnight urine and dietary assessments. However, this dietary assessment intake is limited to reflecting dietary sodium intake due to the variable of sodium content from food sources (e.g., home-cooked foods, restaurant foods, or processed foods), the omission of discretionary salt use, and the under-reporting of problems, especially for obese participants [7]. Spot or overnight urine samples are influenced by many non-dietary sources. Short-term urine samples would varied sodium content due to hydration status, body standing position, time of day, natriuretic or diuretic substance (e.g., caffeine), and disease status (e.g., renal disease and cardiac diseases) [7475]. Consequently, short-term urine collection (i.e., spot urine or overnight urine) and dietary assessment methods could not replace 24-h urine.
Major scientific organizations have raised concerns about research methods for sodium intake assessments. Spot and short-duration timed urine collection methods show systematic errors in estimating an individual’s sodium intake [7677]. The International Consortium for Quality Research on Dietary Sodium/Salt (TRUE) recommends that single spot or short-duration timed urine collections not be used for assessments of dietary sodium intake of individuals especially related to health outcomes [74]. Consequently, it is critical to identify the association between sodium intake and obesity outcomes by utilizing a valid sodium assessment tool such as 24-h urine collection.
We concluded that there is a cross-sectional association between sodium intake and adiposity outcomes. These cross-sectional associations between dietary sodium and obesity were significantly different across sodium intake assessments. Studies that used spot or overnight urine tended to underestimate the sodium-obesity association compared to those utilizing 24-h urine collection. The limitation of this review is that we used only the PubMed database to search for relevant studies. It is recommended that more databases be used to conduct comprehensive searches. Another limitation is that some observational studies did not control for confounding factors for obesity-related outcomes. To identify the causal effects of sodium intake on obesity, we need more high-quality RCTs with the provision of a sodium-reduced diet or foods and a large number of prospective cohort studies that use 24-h urine collection.
 XML Download
XML Download