

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Intensive care units (ICUs) are hospital wards designed for treatment and close monitoring of critically ill patients who require intensive therapy.1 Since the establishment of ICUs in the late 1950s, the specialty of critical care medicine has been developing.23 In South Korea, the first ICUs were set up in two university hospitals to administer respiratory care after surgery, and the number of ICUs has since increased.4 Critical care medicine is important in improving the survival rate and quality of life of critically ill patients.
Lifestyle factors such as smoking, alcohol consumption, and physical activity are known modifiable risk factors associated with age to first chronic disease.5 Previous studies have reported that lifestyle factors are associated with the incidence of several diseases, including new-onset atrial fibrillation, diabetes mellitus, and kidney stone disease.678 Lifestyle is a modifiable risk factor for all-cause mortality and health-related outcomes in adults.9 However, no study has focused on the impact of prior lifestyle habits on mortality among critically ill patients after ICU admission.
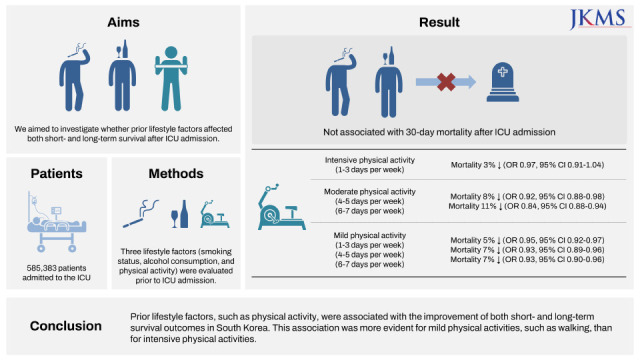
Therefore, this study aimed to investigate whether prior lifestyle factors, such as smoking, alcohol consumption, and physical activity, affect both short- and long-term survival after ICU admission.
METHODS
Data source
All research data were retrieved from the National Health Insurance Service (NHIS) database. The NHIS is the only public health insurance in South Korea and contains and manages data on disease diagnoses and prescriptions for procedures and drugs. Physicians (from all outpatient clinics and hospitals) must register all prescription information on procedures, medications, and disease diagnoses in the NHIS database to obtain information from the government regarding treatment costs. Disease diagnoses were registered using the International Classification of Diseases, External 10th Revision (ICD-10) codes. In addition, the NHIS database contains demographic and socioeconomic status-related information for all patients in South Korea.
Study population
All adult patients (aged ≥ 20 years) who were admitted to the ICU during hospitalization between January 1, 2010, and December 31, 2018, were initially screened. Among the screened patients, we included those who had undergone standardized health examinations in the year prior to admission to the ICU. In South Korea, NHIS subscribers aged ≥ 40 years are recommended to undergo standardized health examinations every 2 years.10 Only the first ICU admission case on the earliest date was included in this study if a patient was admitted to the ICU two or more times during the study period. This exclusion criterion increased the homogeneity of our study population because the physical condition of the patients in the ICU might have been worse on the subsequent ICU admissions than on the first ICU admission. In addition, patients with missing data regarding lifestyle factors in the standardized health examinations were excluded from the final analysis.
Lifestyle factors before ICU admission
Three lifestyle factors were evaluated prior to ICU admission: smoking status, alcohol consumption, and physical activity. Information regarding lifestyle factors was obtained through voluntary responses to questionnaires obtained during standardized health examinations. Smoking status was classified into two groups: current and non-current smokers. Based on previous reports,1112 alcohol consumption was divided into three groups: non-drinkers, mild drinkers, and heavy drinkers. The mild drinkers group was defined as alcohol consumption of ≤ 210 g and ≤ 140 g per week and the heavy drinkers group was defined as alcohol consumption of > 210 g and > 140 g per week in men and women, respectively. Physical activity was divided into three types according to intensity: intensive, moderate, and mild physical activity. Intensive physical activity was defined as strenuous exercise for more than 20 minutes, and moderate physical activity was defined as moderate exercise without breathlessness for more than 30 minutes. Mild physical activity was defined as walking for > 30 minutes. Each exercise intensity was divided into four groups: no exercise, 1–3 times per week, 4–5 times per week, and 6–7 times per week. These physical activities include all type of physical activities from work or leisure in all patients, and the questionnaire for physical activity is presented in Supplementary Data 1. As we used data from standardized health examinations in the year prior to admission to the ICU, physical activity was evaluated during the year prior to admission to the ICU.
Study endpoint
Our study had two primary endpoints: 30-day mortality and 1-year all-cause mortality after ICU admission. Mortality was defined as death within 30 days or 1 year after ICU admission.
Covariates from standardized health examination
Information from the standardized health examination was collected and used as covariates. Body mass index data were collected and categorized into six groups: < 18.5, 18.5–24.9, 25.0–29.9, 30.0–34.9, 35.0–39.9, and > 40 kg/m2. Waist circumference was measured and classified into two groups: ≥ 90 cm and < 90 cm. All laboratory results were obtained from venous blood samples during standardized medical examinations. Included individuals were diagnosed with anemia, according to the World Health Organization criteria, as hemoglobin levels of < 12 g/dL and < 13 g/dL for women and men, respectively. Cut-off values of 125, 200, 40, and 130 mg/dL were used for fasting serum blood glucose, serum total cholesterol, high-density lipoprotein, and low-density lipoprotein levels, respectively. Cut-off values of 40 IU/L were used for aspartate transaminase, alanine transaminase, and gamma-glutamyl transferase.
Other covariates
All covariates in this study were collected based on previous research on the epidemiology of ICU admissions in South Korea.13
Statistical analysis
The clinicopathological characteristics were presented as mean values with standard deviation (SD) for continuous variables and numbers with percentages for categorical variables. We constructed a multivariable logistic regression model to assess the prior lifestyle factors associated with 30-day mortality. All covariates were included in the multivariable adjustment in the model. The Hosmer–Lemeshow test was used to confirm that the goodness of fit in the model was appropriate. The results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). We also constructed a multivariable Cox regression model to determine prior lifestyle factors associated with 1-year all-cause mortality. All covariates were included for multivariable adjustment in the model, and log-log plots were used to confirm that the central assumption of the Cox proportional hazard models was satisfied. The results are presented as hazard ratios (HRs) with 95% CIs. There was no multicollinearity issue with the criterion of variance inflation factors < 2.0 between variables. All statistical analyses were performed using IBM SPSS Statistics for Windows (version 25.0; IBM Corp., Armonk, NY, USA), and statistical significance was set at P < 0.05.
Ethics statement
This retrospective, population-based cohort study was conducted after obtaining approval from the Institutional Review Board (IRB) of Seoul National University Bundang Hospital (IRB approval number: X-2102-666-904). The Big Data Center of the NHIS also approved data sharing for this study (NHIS-2021-1-620). The requirement for informed consent was waived because the data analyses were performed retrospectively using anonymized data derived from the South Korean NHIS database.
RESULTS
Study population
Fig. 1 shows a flowchart of the patient selection process. From January 1, 2010 to December 31, 2018, there were 3,132,769 ICU admissions, of which 2,212,923 were adult patients. Among them, 695,897 ICU admissions of 665,732 patients who had undergone standardized health examinations in the year prior to admission to the ICU were initially screened. A total of 30,165 patients with ≥ 2 ICU admissions during the study period were excluded to focus only on the first ICU admission on the earliest date. Next, 80,349 patients with missing standardized health examination data in the year prior to admission to the ICU were excluded. Ultimately, 585,383 patients were included in the analysis. Among them, 59,075 (10.1%) and 113,476 (19.4%) patients died within 30 days and 1 year after ICU admission, respectively. Table 1 shows the clinicopathological characteristics of the patients included in this study. The patients were 62.9% male (368,343/585,383) with a mean age of 64.9 years (SD: 13.1 years). The mean length of hospital and ICU stays was 13.8 days (SD: 12.0 days) and 3.0 days (SD: 4.2 days), respectively. The surgery-associated hospital admissions were 72.9% (426,834/585,383). Table 2 shows the data regarding standardized health examinations in the year prior to ICU admission.
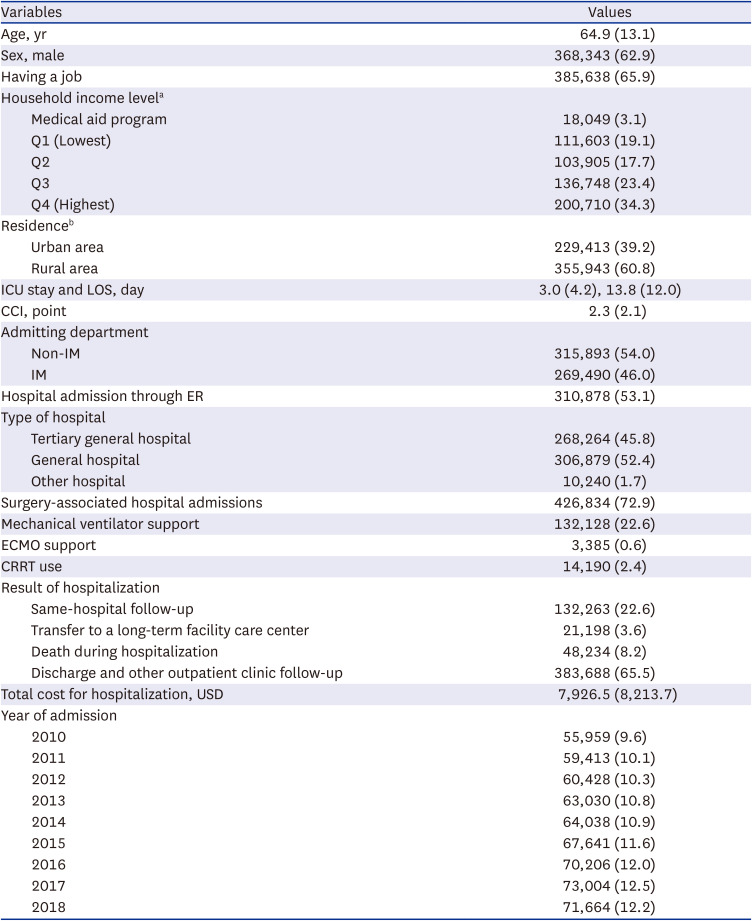
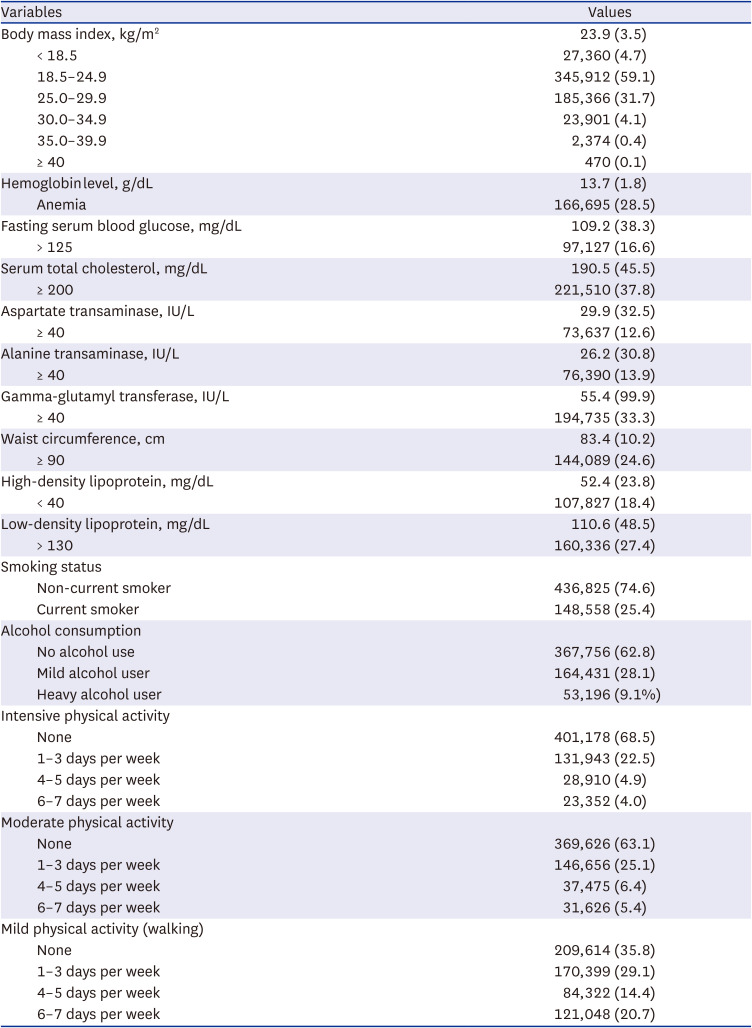
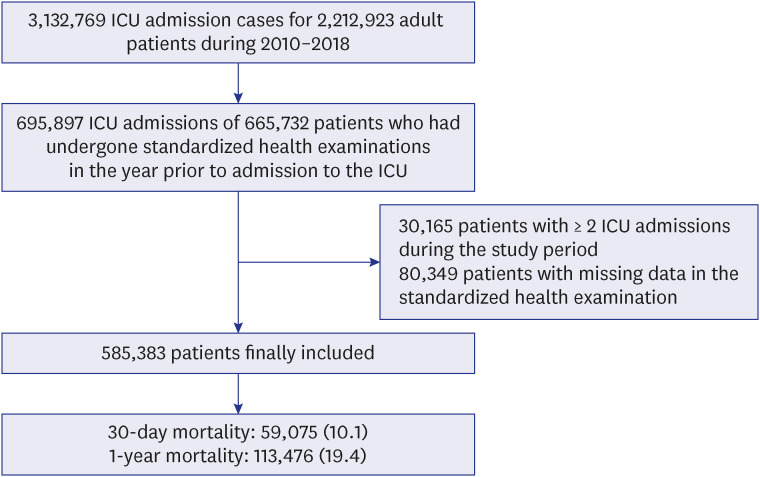
Table 1
Clinicopathological characteristics of the patients included in this study.
Values are presented as mean ± standard deviation or number (%).
ICU = intensive care unit, LOS = length of hospital stays, CCI = Charlson comorbidity index, IM = internal medicine, ER = emergency room, ECMO = extracorporeal membrane oxygenation, CRRT = continuous renal replacement therapy, USD = United States Dollar.
aUnknown values of household income level were 14,368 (2.5%); bUnknown values of residence were 27 (0.0%).
![]()
Table 2
Data regarding standardized health examinations in the year prior to ICU admission
![]()
30-Day mortality
Table 3 shows the results of the multivariable logistic regression model for 30-day mortality after ICU admission. Current smoking (vs. non-current smokers: OR, 0.99; 95% CI, 0.96–1.02; P = 0.432), mild alcohol drinking (vs. no alcohol drinking: OR, 1.00; 95% CI, 0.96–1.03; P = 0.825), and heavy alcohol drinking (vs. no alcohol drinking: OR, 0.97; 95% CI, 0.92–1.01; P = 0.166) were not associated with 30-day mortality after ICU admission. One to 3 days per week of intensive physical activity was associated with lower odds of 30-day mortality (OR, 0.96; 95% CI, 0.93–0.99; P = 0.016) than without intensive physical activity. Four to 5 days per week (OR, 0.92; 95% CI, 0.88–0.98; P = 0.005) and 6–7 days per week (OR, 0.89; 95% CI, 0.84–0.94; P < 0.001) of moderate physical activity were associated with lower odds of 30-day mortality than without moderate physical activity. One to three days per week (OR, 0.95; 95% CI, 0.92–0.97; P < 0.001), 4–5 days per week (OR, 0.93; 95% CI, 0.89–0.96; P < 0.001), and 6–7 days per week (OR, 0.93; 95% CI, 0.90–0.96; P < 0.001) of mild physical activity were associated with lower odds of 30-day mortality than no physical activity. Other ORs with 95% CI for all other covariates are presented in Supplementary Table 1.
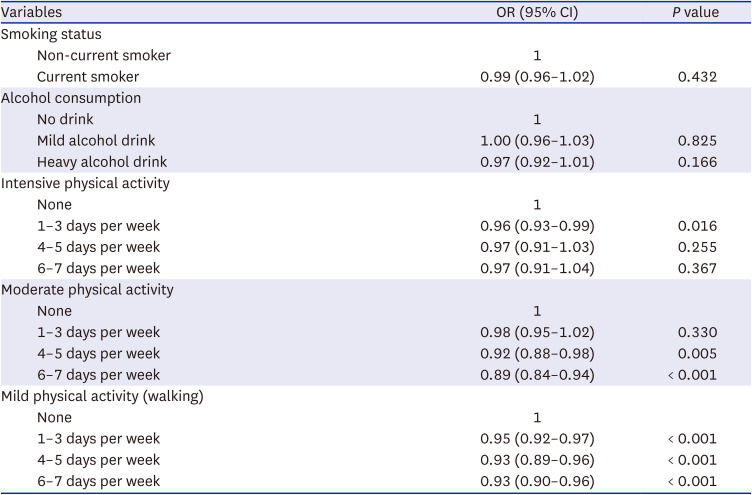
Table 3
Multivariable logistic regression model for 30-day mortality after intensive care unit admission
![]()
1-Year all-cause mortality
Table 4 shows the results of the multivariable Cox regression model for 1-year all-cause mortality after ICU admission. Current smoking was associated with a higher risk of 1-year all-cause mortality (HR, 1.02; 95% CI, 1.01–1.04; P = 0.020) than not currently smoking. Mild alcohol drinking (vs. no alcohol drinking: HR, 1.02; 95% CI, 0.99–1.03; P = 0.545) and heavy alcohol drinking (vs. no alcohol drinking: HR, 0.98; 95% CI, 0.93–1.02; P = 0.156) were not associated with 1-year all-cause mortality after ICU admission. One to 3 days per week (HR, 0.95; 95% CI, 0.93–0.97; P < 0.001) and 4–5 days per week (HR, 0.95; 95% CI, 0.91–0.98; P = 0.003) of intensive physical activity were associated with lower risk of 1-year all-cause mortality than no intensive physical activity. One to 3 days per week (HR, 0.97; 95% CI, 0.95–0.99; P = 0.004), 4–5 days per week (HR, 0.94; 95% CI, 0.91–0.97; P < 0.001), and 6–7 days per week (HR, 0.92; 95% CI, 0.91–0.97; P < 0.001) of moderate physical activity were associated with lower risk of 1-year all-cause mortality than no moderate physical activity. One to 3 days per week (HR, 0.94; 95% CI, 0.93–0.96; P < 0.001), 4–5 days per week (HR, 0.94; 95% CI, 0.91–0.97; P < 0.001), and 6–7 days per week (HR, 0.92; 95% CI, 0.89–0.95; P < 0.001) of mild physical activity were associated with lower odds of 1-year all-cause mortality than no mild physical activity. Other HRs with 95% CI for all other covariates are presented in Supplementary Table 2.
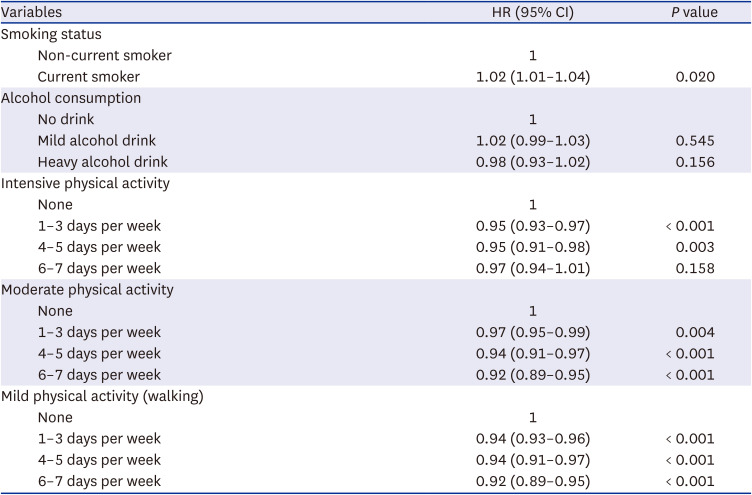
Table 4
Multivariable Cox regression model for 1-year all-cause mortality after intensive care unit admission
![]()
DISCUSSION
This population-based cohort study showed that prior lifestyle factors, such as physical activity, were associated with improvements in both short- and long-term survival outcomes. Moreover, this association was more evident for mild physical activities, such as walking, than for intensive physical activities. However, prior lifestyle factors, such as smoking and alcohol consumption, were not associated with survival outcomes after ICU admission. This was the first study to show that prior lifestyle factors could affect the prognosis of critically ill patients requiring ICU admission.
In the United States, an estimated $117 billion in annual health care costs and approximately 10% of premature mortality are associated with inadequate physical activity.14 Therefore, physical activity guidelines exist for improving health conditions.15 Physical inactivity has a major health effect worldwide, and an increase in physical activity could substantially improve health.16 Although there has been one report that emphasizes the effect of physical activity during ICU stay or hospitalization for rehabilitation,17 the importance of prior physical activity in improving survival outcomes after ICU admission among critically ill patients has not yet been studied.
Compared with intensive physical activity, mild physical activity, such as walking, provided better short- and long-term survival outcomes among critically ill patients. Walking is associated with important cardiovascular health benefits and has been shown to reduce anxiety and tension and aid in weight loss.18 In a large prospective cohort of older adults in the United States, walking was associated with a lower risk of all-cause mortality than inactivity.19 This can be explained by the following assumptions. First, regular physical exercise promotes improvements in the quality of life and can act on the immune response, reducing the risk of developing systemic inflammatory processes and stimulating cellular immunity.20 Lymph drainage is known to be elevated by muscular contractions; thus, exercise may enhance immune cell transport from the site of antigen administration to the lymph nodes.21 Moderate exercise also has a favorable effect on immunity, which might result in decreased illness rates.22 A recent review reported that physical exercise can increase immune function against coronavirus disease.23 Second, patients who could walk prior to ICU admission had a relatively better performance status than those who could not. This could also affect the results of this study because prior health status, such as frailty, plays an important role in determining the outcomes of critically ill patients requiring ICU admission.24
While our results suggested that mild physical activity, such as walking, was associated with lower mortality rates than intensive physical activity, previous literature has reported that vigorous- and moderate-intensity physical activities reduce all-cause mortality.25 The characteristics of patients in this cohort study should also be considered. As we focused on patients who were admitted to the ICU due to critical illness, patients were likely to have various underlying or chronic medical conditions, and the mean value of CCI among total patients was 2.3 point (SD: 2.1 point). Therefore, intensive or moderate physical activity might be difficult in patients in our study. However, this information is currently lacking, and further study is needed to determine the impact of the degree of physical activity on mortality among critically ill patients.
Interestingly, although current smoking status was not associated with 30-day mortality risk in the multivariable Cox regression model, it was associated with an increased 1-year mortality risk than not currently smoking. In a retrospective analysis from a single institution, it was reported that in patients with severe sepsis or septic shock, current smoking was associated with longer hospital stay, need for mechanical ventilation, and increased mortality.26 A multicenter cohort study in Australia and New Zealand reported that smoking had a dose-related effect on mortality in critically ill patients.27 Smoking induces endothelial injury during the development of acute respiratory distress syndrome and emphysema.28 A meta-analysis of previous literature found that smoking status affects disease severity and mortality in hospitalized patients with coronavirus disease.29 More studies are needed to confirm the relationship between current smoking before ICU admission and mortality risk after ICU admission.
This study had several limitations. First, the ICU data and disease severity of all patients during ICU stay were not adjusted according to the Acute Physiology and Chronic Health Evaluation II score or simplified acute physiology score II. Second, the generalizability of the results of this study may be limited because the environment or policies of critical care in ICU differ in other countries. Lastly, in South Korea, NHIS subscribers aged ≥ 40 years are recommended to undergo standardized health examinations every 2 years10; therefore, the study population was relatively older, with a mean age of 64.9 years (SD: 13.1 years). If we had included all patients regardless of age, the results may have been different.
In conclusion, prior lifestyle factors, such as physical activity, were associated with improvements in both short- and long-term survival outcomes in South Korea. This association was more evident for mild physical activities, such as walking, than for intensive physical activities.
 XML Download
XML Download