

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Guidelines on the use of disease-modifying anti-rheumatic drugs (DMARDs) before severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccination in patients with rheumatoid arthritis (RA) have been continuously updated given that they are thought to lower immunogenicity.123
Patients with autoimmune diseases and those taking anti-cytokine therapies were excluded from all SARS-CoV-2 phase III trials approved by the US Food and Drug Administration and European Medicines Agency.456 Immunocompromised patients with SARS-CoV-2 mRNA vaccination elicited high immunogenicity in the original vaccine trials78; however, recent studies have shown blunted immunogenicity in immunocompromised populations after vaccination.910
Detailed understanding on the SARS-CoV-2 vaccination remains elusive given the scarcity of data on the vaccine response in immunosuppressed patients. Post-vaccination antibody titers in patients with chronic inflammatory diseases have further decreased depending on the type of vaccine as well as the type of treatment the patient is receiving.111 However, the immunosuppressive effect of autoimmune diseases on vaccination efficacy against SARS-CoV-2 is currently unclear. Furthermore, the effectiveness of the SARS-CoV-2 booster vaccine has been widely discussed and interest in antibody generation in different types of vaccines continues to grow.12131415
In South Korea, individuals aged 60 years and over were vaccinated with priority with ChAdOx-1-S nCov-19 from April 2021. Those individuals were then followed up for the second dose after 2–4 months. Individuals not eligible for ChAdOx1-S nCoV-19 were administered the Moderna, Pfizer, or Janssen vaccination after the first inoculation. However, patients with autoimmune diseases were prioritized; therefore, many were vaccinated with the ChAdOx1-S nCoV-19 vaccine on the first and second doses. After two doses of the ChAdOx1-S nCoV-19 vaccine, the mRNA vaccine (Pfizer or Moderna) was recommended for all patients 2–6 months after the last inoculation in place of a third ChAdOx1-S nCoV-19 dose.
Although there is sufficient research on the mRNA vaccine, studies on the ChAdOx1-S nCov-19 vaccine are lacking, despite administration of two doses to large population including patients with RA in South Korea. We targeted these patients who had or had not received the third mRNA vaccine for our study. Thus, we investigated the differences in antibody formation after receiving the mRNA vaccine as the third dose in patients who received the initial two doses of ChAdOx1-S nCoV-19. Factors associated with antibody production were also evaluated in patients who received two doses of ChAdOx1-S nCoV-19 under different medication scenarios and clinical parameters. Moreover, we investigated whether antibody titers decreased over time after 3rd mRNA vaccination.
METHODS
Study design and participants
This study was conducted at a single tertiary hospital in South Korea, from October 14, 2021, to June 17, 2022. Patients diagnosed with RA satisfying the 2010 American College of Rheumatology/European League Against Rheumatism classification criteria,16 who were aged 40 years or older with more than 6 months of follow-up at our center qualified for the study, while those infected with SARS-CoV-2 before or during the study were excluded.
Primary endpoint
Our study focused on patients who had received the ChAdOx1-S nCoV-19 vaccine (AstraZeneca) as first and second doses, which was initially widely distributed in South Korea. Patients with RA who met the above requirements and had received two doses of the ChAdOx1-S nCoV-19 vaccine at least 2 weeks before the study were selected as primary participants. Moreover, since most patients had received the third dose as the mRNA vaccine (Pfizer, Moderna) between 2 and 6 months after the second dose of ChAdOx1-S nCoV-19 vaccination, those who had received this third dose at least 2 weeks before the study were also included. The duration between the date of the most recent vaccination and the date of sample acquisition was calculated.
Disease Activity Score-28-erythrocyte sedimentation rate (DAS28-ESR) was measured at sample acquisition.17 All medications, including conventional synthetic DMARDs (csDMARDs), tumor necrosis factor (TNF) inhibitor, Janus kinase (JAK) inhibitor, abatacept, tocilizumab, and corticosteroids were collected at the time of sample acquisition and confirmation that the patients had been prescribed and medicated with corresponding medications for at least 3 months was obtained. In addition, for patients using these immunosuppressive agents, we explained the domestic guidelines for temporally withholding or regulating medications after each vaccination, and most patients adjusted their medications at the right time according to the guideline recommendations.18
Secondary endpoint
For patients who completed the 3rd mRNA vaccination, we followed up the antibody titers to determine whether the antibody titers were waning. We acquired the sampling of following antibody titers of whom underwent outpatient follow-up within 4 months from the date of first sample acquisition.
Detection of SARS-CoV-2 antibody
Serum samples from patients with RA were tested on the commercially available Elecsys® Anti-SARS-CoV-2 assay (ACOAS2S) (Roche Diagnostics International Ltd., Rotkreuz, Switzerland), per the manufacturer’s instructions. The ACOVA2S is an electrochemiluminescence immunoassay developed to detect antibodies to the SARS-CoV-2 spike (S) protein in human serum and plasma. The Ministry of Food and Drug Safety has granted ACOV2S emergency approval for research. The results were measured on a cobas e 602 module (Roche Diagnostics Operations, Indianapolis, IN, USA). After calibration and quality control, results were automatically reported as the analytic concentration of each sample in U/mL, with a threshold of < 0.80 U/mL interpreted as negative for anti-SARS-CoV-2 S antibodies and ≥ 0.80 U/mL interpreted as positive (Elecsys Anti-SARS-CoV-2 S assay method sheet 2021-05; version 2.0; Roche Diagnostics GmbH, Indianapolis, IN, USA). Values between 0.40–250 U/mL represent the primary measuring range. Results below this range were set to 0.4 U/mL and qualified as non-reactive.
Statistical analyses
Data are presented as box and whisker plots, and Fisher’s exact test was used for statistical analyses as appropriate. Continuous variables were assessed using Student’s t-test. Univariate binary logistic regression models were used to analyze medications and clinical parameters for acquiring high antibody titers. Multivariate tests were performed by selecting factors with a P value of < 0.05 in univariate tests in a forward stepwise approach. For all analyses, statistical significance was set at P < 0.05. All statistical analyses were performed using SPSS software (IBM SPSS Statistics version 21; IBM Corp., Armonk, NY, USA).
RESULTS
Anti-S1/receptor binding domain (RBD)-specific antibody formation
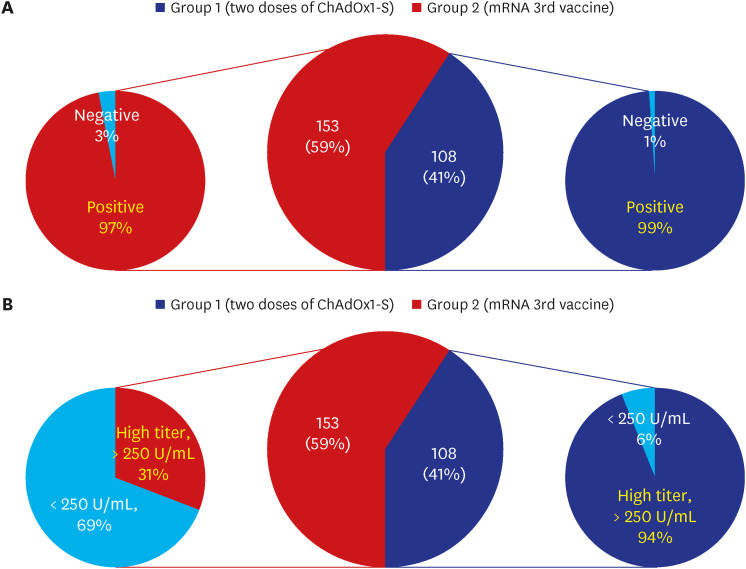
Among the 261 patients, 153 had received two doses of ChAdOx1-S nCoV-19, and 108 had been administered the mRNA vaccine as the third dose. The positive rates of anti-SARS-CoV-2 anti-S1/RBD-specific antibody (titer > 0.8 U/mL) for the two groups were 97% (149/153) and 99% (107/108), respectively. Only five patients had negative results (titer < 0.8 U/mL); two with tofacitinib, one with abatacept, one with 12.5 mg of methotrexate weekly, and one taking 5 mg corticosteroid daily). However, a high antibody titer (> 250 U/mL), which is the upper limit of the RBD antibody immunoassay, was only detected in 31% (47/153) of the second vaccination group, whereas 94% (102/108) were observed in the third vaccination group (Fig. 1).
Fig. 1
Positivity rates of SARS-CoV-2 anti-S1/RBD-specific antibody (titer > 0.8 U/mL) (A) and the high antibody titer (> 250 U/mL) rates of SARS-CoV-2 anti-S1/RBD-specific antibody (B) in each group.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, S = spike, RBD = receptor binding domain.
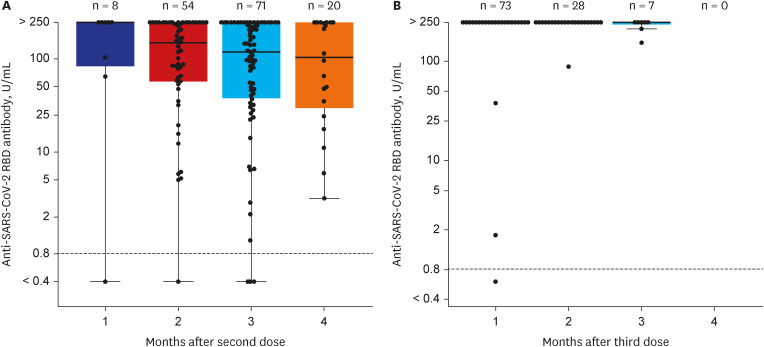
The mean duration between the date of the second inoculation of ChAdOx1-S nCoV-19 and the date of sample acquisition was 9.0 weeks in the ChAdOx1-S nCoV-19 group (group 1), with eight patients at 1 month, 54 patients at 2 months, 71 patients at 3 months, and 20 patients at 4 months (Fig. 2A). However, the mean duration between the date of the most recent mRNA vaccination and the date of sample acquisition was 4.1 weeks in the third mRNA vaccination group (group 2), with 73 patients at 1 month, 28 patients at 2 months, and seven patients at 3 months (Fig. 2B). Data in group 1 indicated that increases in the duration between the date of the most recent ChAdOx1-S nCoV-19 vaccination and the date of sample acquisition caused decreases in the median value of anti-SARS CoV-2 RBD antibody titer.
Clinical features and factors associated with antibody formation
The median age of all 261 patients was 64.9, and 73.9% (n = 190) were female. The mean DAS28-ESR score was 2.65. The mean duration between the last vaccination date and the date of sample acquisition was 7.1 weeks for all patients. Each patient with RA was presented with various medication scenarios and categorized according to the medication used as csDMARD, TNF inhibitor, JAK inhibitor, abatacept, tocilizumab, or corticosteroids.
Patients treated with csDMARD made up for more than half of the total patients with 138 patients, and 28 patients were being treated with TNF inhibitor, 54 patients with JAK inhibitors such as tofacitinib and baricitinib, 11 patients with abatacept, and 19 patients with tocilizumab. Patients treated with corticosteroids made up 62.1% of the total patients with 162 patients. Cumulative dosages of methotrexate or corticosteroids were 6.58 g and 2.23 g, respectively.
The clinical features and the medication history between group 1 and group 2 are compared in Table 1. Despite a difference in the mean duration between the date of last vaccination and the date of sample acquisition between the two groups, age, sex, and DAS28-ESR score did not differ. The only difference in medication was in patients treated with tocilizumab (17 patients in group 1 and two patients in group 2); no other differences were noted.
Table 1
Baseline characteristics of patients who received two doses of ChAdOx1-S nCoV-2 (group 1) and patients who received a third dose of the mRNA vaccine (group 2)
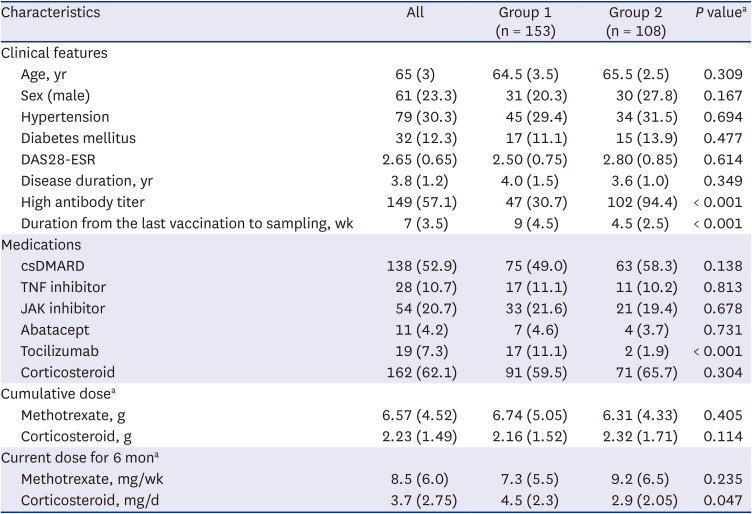
Next, we adopted univariate and multivariate binary logistic regression models for each group to determine whether the use of DMARDs and different clinical aspects of each patient affected the acquisition of a high antibody titer of 250 U/mL or more. Old age, male sex, and corticosteroid use in group 1 were associated with low acquisition of high antibody titer (> 250 U/mL) in the multivariate analyses (Table 2). As in the case of corticosteroids, increases in cumulative dose tended to be associated with decreased antibody titer.
Table 2
Analysis of DMARDs and clinical parameters for the acquisition of high antibody titer (> 250 U/mL) after two doses of ChAdOx1-S nCoV-2

Among the different DMARDs and clinical characteristics, multivariate analysis revealed that corticosteroid use (odds ratio [OR], 0.35; 95% confidence interval [CI], 0.16–0.75), older age (OR, 0.91; 95% CI, 0.86–0.98), and male sex (OR, 0.23; 95% CI, 0.07–0.74) were associated with a low rate of high antibody titers after two doses of ChAdOx1-S nCoV-19 (Table 2). On the other hand, among group 2 with the third mRNA vaccine, any DMARDs or clinical parameters did not bring significant results since the majority had high antibody titer (> 250 U/mL) (Supplementary Table 1).
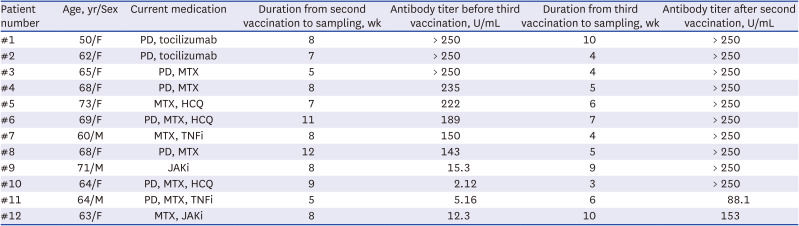
As shown in Table 3, 12 out of 261 patients underwent serial antibody testing before and after the third mRNA vaccine. Only three patients showed a high titer of > 250 U/mL after the second vaccination, two using tocilizumab, and one using methotrexate. Of the nine patients who showed a titer of ≤ 250 U/mL after the second vaccination, seven had a high titer of > 250 U/mL after the third vaccination. Of the remaining two patients, one was using a TNF inhibitor (#11). Sample acquisition was performed at 5 weeks after the second vaccination, and 6 weeks after the third vaccination, antibody titer increased from 5 U/mL to 88 U/mL; the other was using JAK inhibitor (#12), the sample acquisition was carried out at 8 weeks after the second vaccination and 10 weeks after the third vaccination, antibody titer increased from 12.3 U/mL to 153 U/mL.
Table 3
Characteristics of 12 patients who have acquired samples sequentially before and after third vaccination
Waning antibody responses in patients with high antibody titers
Of the 108 patients who completed 3rd mRNA vaccination, 103 patients except only five had a high antibody titer of 250 or higher. Antibody titers were measured again on the day of the outpatient visit to confirm the decrease in antibody titers in 46 patients who had undergone outpatient follow-up within 4 months. The mean duration of first antibody titer measurement of 46 patients was 4.2 weeks after 3rd mRNA vaccination, and the mean duration of second antibody titer measurement of the corresponding patients was 15.4 weeks after 3rd mRNA vaccination, and it was examined whether antibody titers decreased at intervals of about 3 months (Fig. 3).
Fig. 3
Waning patterns of anti-severe acute respiratory syndrome coronavirus 2 receptor binding domain antibody titer in 46 rheumatoid arthritis patients who have acquired samples two times sequentially after 3rd mRNA vaccination. To effectively mark points with the same value, jittering was used.
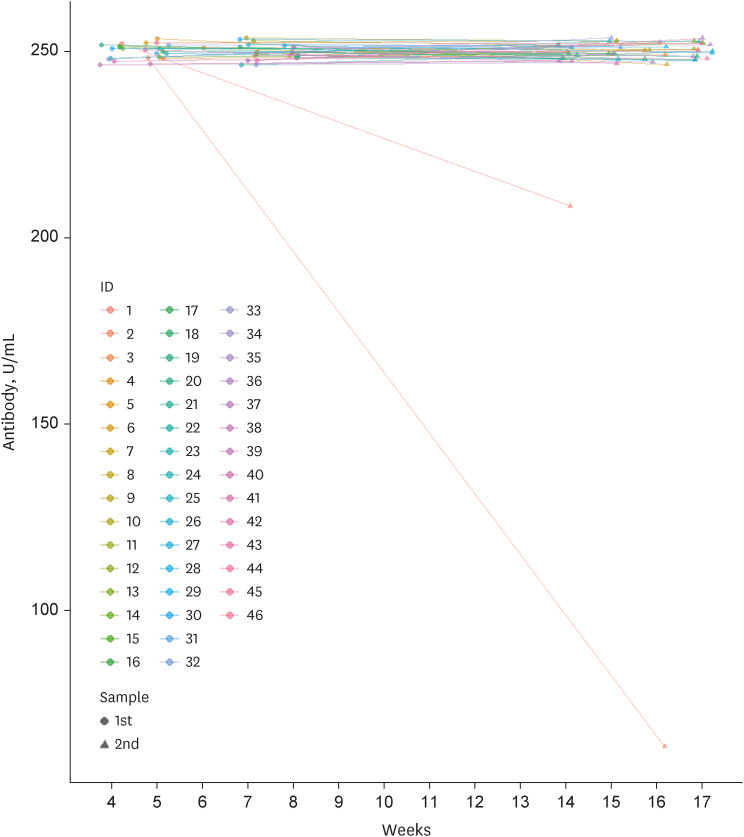
Of 46 patients who had a high antibody titer of 250 or higher, 44 patients maintained high antibody titers; however, in two patients, antibody titers decreased to 205 and 64.3, respectively. One patient was using MTX and JAK inhibitor, and the other was using only MTX and corticosteroid (Supplementary Table 2).
DISCUSSION
In this cross-sectional and longitudinal cohort of patients with RA who had completed two doses of the ChAdOx1-S nCoV-19 vaccination and a third dose of the mRNA vaccination, antibody positivity of >0.8 U/mL was achieved in 97% and 99% of patients, respectively, leaving five of 261 patients with a negative result.
However, 94% of patients in group 2 achieved a high titer compared with 31% of group 1. This disparity of more than 3 times the difference is remarkable. Our findings can be used as evidence for the need for a third mRNA vaccination in patients with RA, as well as in patients with other autoimmune diseases. Notably, the median value of the antibody titer decreased as the mean duration between the date of last vaccination and date of sample acquisition increased from 1 month to 4 months (Fig. 2).
Vaccination or natural infection-induced immunity to SARS-CoV-2 protects against reinfection and reduces the risk of clinically significant outcomes. Recovered seropositive patients have an estimated 89% protection rate from reinfection,19 and 50–95% vaccine efficacies have been reported.20 However, the duration of this protective immunity is unclear; primary immune responses are inevitably waning,212223 and there is ongoing transmission of increasingly concerning viral variants that may escape the control of vaccine-induced and convalescent immune responses. A critical challenge is identifying the immune correlates of protection from SARS-CoV-2 infection, thereby predicting how immunity changes, which will be reflected in clinical outcomes.
Individual medication scenarios appear to have no significant effect in achieving high antibody titer other than corticosteroid use. This result reflects those of previous studies conducted on patients with rheumatic disease.2425 Several studies reported that corticosteroids can be safely continued to control the underlying autoimmune disease considering coronavirus disease 2019 (COVID-19) vaccines are non-live vaccines with no potential for viral reactivation in vivo; however, corticosteroid use should be kept as low as possible to decrease the risk of COVID-19-related complications because corticosteroid at a prednisone-equivalent dose of > 10 mg/day can increase the severity of COVID-19.18 In addition, our results suggest that it is advisable to keep the corticosteroid dose as low as possible, not only to reduce COVID-19 complications, but also to increase the rate of antibody titer production after vaccination.
In addition, a recent study reported that women had higher levels of humoral immunity after ChAdOx-1 nCoV-19 vaccine.26 This result is consistent with the significantly lower rates of high antibody titer production in men in our study. Furthermore, in that study, the antibody response to mRNA vaccine was higher than the response to ChAdOx-1 nCoV-19 vaccine, which is also in line with our results. Also, other studies reported that hypertension or DM could be negatively associated with antibody response to SARS-CoV-2 vaccination,272829 however, such co-morbidities did not show a significant difference in antibody production between two groups.
On the other hand, several studies introduced cases of mycophenolate mofetil and rituximab and found that a high proportion of the patients achieved negativity in antibody titer.2324 These results should be interpreted with caution because of the variation in the vaccine type and duration. A cohort study performed with patients with inflammatory bowel disease (IBD) reported that those using TNF inhibitors showed lower antibody titer than the control group.30 Differences in the results of this study may be attributed to the large population of 480 patients and IBD showing different pathophysiology to inflammatory arthritis.
We also confirmed antibody titers in all 261 patients and, in 12 cases, acquired samples sequentially before and after the third vaccination. Of the 9 patients who had not acquired high antibody titer after two doses of ChAdOx-1-S nCov-19, only 7 patients obtained high antibody titer after the 3rd mRNA vaccine, which was less than expected. Two patients (#11, 12) treated with TNF inhibitor and JAK inhibitor did not reach a high titer of > 250 U/mL despite receiving the third vaccination. Whereas two patients (#1, 2) treated with tocilizumab showed a high titer of > 250 U/mL before and after the third vaccination.
Tocilizumab is a humanized monoclonal IL-6 receptor blocker used for RA treatment. It is also one of the choices of cytokine storm treatments that may develop during COVID-19 infection.3132 Mori et al.33 demonstrated that tocilizumab treatment did not prevent the development of antibodies against the influenza vaccine in patients with RA. Another study evaluated the humoral immune response of the pneumococcal polysaccharide vaccine in patients with RA receiving tocilizumab and found no differences between tocilizumab recipients and the control groups.3435 Until recently, most reports on tocilizumab for COVID-19 treatment have included only a limited number of patients, and there were no direct studies on therapeutic responses and antibody formation. Further research and data from ongoing trials should be collated to position tocilizumab as a major therapeutic agent for COVID-19.
In addition, research on the waning of the antibody titers depending on the period continues because the question about whether it is necessary to inoculate fourth or fifth COVID-19 vaccination, or to inoculate routinely as like Influenza. Most of the previous studies on waning immune humoral response have been conducted on patients with COVID-19 infection rather than after vaccination.3637 In Israel, the largest study with vaccinated patients was done, they compared antibody titers after two weeks and then six months sequentially in 3,800 patients who completed the first and second mRNA COVID-19 vaccines, and the results were; the anti-S1/RBD-specific antibody titer is substantially lower among men, persons 65 years of age or older, and participants with immunosuppression than those without immunosuppression.38
Our study included a relatively small number of 46 patients and followed the antibody titer over a period of median 11 weeks, and high antibody titers were maintained in most patients. One of the biggest differences in these results is that, while the previous study showed waning of antibody titers even at 3 months, the previous study looked at patients who completed only first and second mRNA vaccination, whereas we intended for patients who have completed up to the third vaccination. In the same context, in Fig. 2, in the case of patients who completed only two doses of ChAdOx1-S nCoV-19 vaccine, antibody titers decreased rapidly even at the third or fourth months. Through these results, it is conceivable that the 3rd mRNA vaccination maintains relatively high antibody titers, even in patients with immunosuppression. However, more long-term follow-up may be necessary to establish the basis for the COVID-19 vaccination interval, such as whether vaccination should be performed every 6 months or every 12 months.
This study tested patients for a high titer (> 250 U/mL) using an RBD antibody immunoassay. Anti-S1/RBD-specific antibodies are often correlated with long-term immunity in several viral infections.39 However, there is no established threshold or guideline on the value of RBD antibody immunoassay titers that implies protection over the infection. Therefore, it is difficult to interpret the high titer and predict the associated effects on the severity of infection. Although a high titer may imply higher immunity,3840 establishing further guidelines would allow for further research to be pursued.
Many patients with RA and those with other autoimmune diseases experienced increased anxiety and fear concerning the repeated vaccination schedule. Our results provide evidence for reassurance to patients with RA who may experience fear and worry over the third vaccination. In particular, male and older patients and those taking corticosteroids were associated with low antibody levels. Therefore, patients with these risk factors are strongly recommended for the third vaccination.
 XML Download
XML Download