

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The emergence and global spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) resulted in a declaration of a pandemic by the World Health Organization (WHO) in March 2020. The ongoing coronavirus disease 2019 (COVID-19) outbreak has posed a serious threat to global health and public safety. According to the WHO COVID-19 weekly epidemiological update, 546,363,985 cases of COVID-19 occurred globally and 6,336,802 patients died of COVID-19 as of July 2022.1
To contain the pandemic, there has been an unprecedented worldwide effort to develop vaccines against SARS-CoV-2. Various vaccines including BNT162b2 (Pfizer-BioNTech), ChAdOx1 nCov-19/AZD1222 (AstraZeneca-University of Oxford), mRNA-1273 (Moderna), and Ad26.COV2.S (Johnson & Johnson) have shown efficacies of 66–95% in preventing COVID-19 and acceptable short-term safety profiles in phase 3 trials.234 This led to emergency authorization of COVID-19 vaccines and implementation of mass vaccination in many countries. However, subsequent reports of severe adverse reactions such as thrombosis with thrombocytopenia, myocarditis, and Guillain-Barre syndrome raised concerns regarding the safety of COVID-19 vaccines.567 One of the serious adverse reactions is vaccine-associated interstitial lung disease (ILD) or pneumonitis. Recently, several cases of pneumonitis following COVID-19 vaccines have been published.8910111213 These cases, as well as the reports of patients suspicious for vaccine-associated pneumonitis in clinical practice, raised alerts among the Korea Interstitial Lung Diseases Study group, an official study group affiliated with the Korean Academy of Tuberculosis and Respiratory Diseases.
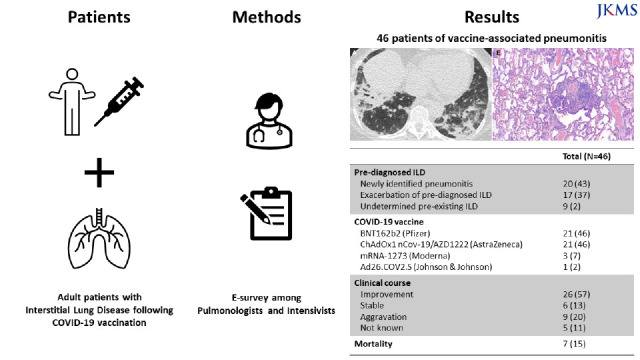
This emergency survey study aimed to identify cases of vaccine-associated pneumonitis in the Republic of Korea and demonstrate their clinical characteristics and outcomes.
METHODS
Study design and subjects
This was a nationwide multicenter electronic mail-based survey study in the Republic of Korea. An electronic mail containing questionnaires was sent to the members of the Korea ILD Study Group from 21 referral hospitals in the Republic of Korea in mid-October 2021. The members were requested to report cases diagnosed with vaccine-associated pneumonitis (development of pneumonitis or exacerbation of pre-diagnosed ILD) associated with COVID-19 vaccine, which was first administered on February 26, 2021, in the Republic of Korea. The case definition of vaccine-associated pneumonitis was 1) the development of new symptoms or acute worsening of pre-existing symptoms within 4 weeks of vaccine administration; 2) new pulmonary infiltrates including ground-glass opacities, and consolidation regardless of pre-existing infiltrates; and 3) exclusion of known etiologies or aggravating factors of ILD, such as drugs or environmental exposures. Clinical, radiological, and pathological data of all reported cases were reviewed by the authors through multiple rounds of multidisciplinary discussion (MDD) process to make the final diagnosis and enrollment.
Data collection
Details on the demographics and clinical characteristics of patients including age, gender, work and environmental exposures, drug history, smoking history, types and doses of the vaccines, symptoms and their onset, hypoxemia (defined as oxygen saturation below 90% at room air or need for oxygen supplementation), mechanical ventilation and/or vasopressor support, and hospital and intensive care unit admission were collected. Furthermore, data on pulmonary function and laboratory results including serologic tests for connective tissue diseases (CTDs) and Krebs von den Lungen-6 (KL-6) at the time of presentation were collected. Antinuclear antibody titer of 1:40 or higher was regarded as positive. Sputum culture and virus polymerize chain reaction (PCR) tests, chest computed tomography (CT) findings, bronchoalveolar lavage (BAL), transbronchial lung biopsy (TBLB), and/or surgical lung biopsy (SLB) in patients who underwent the tests were also obtained. Finally, data on the treatment and outcomes of the patients were reported.
Statistical analysis
Data are presented as median (interquartile range [IQR]) or number (n) (%). Subgroup analysis based on the presence of pre-diagnosed ILD was performed. Comparison of clinical characteristics and outcomes between patients who received mRNA vaccines and adenovirus vector-based vaccines was done using chi-square test or Fisher’s exact test for categorical variables and the Mann-Whitney U test for continuous variables. Data were analyzed using IBM SPSS Statistics 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics of the patients
A total of 49 patients diagnosed with pneumonitis associated with the COVID-19 vaccine from 17 hospitals across the Republic of Korea were reported. After multiple rounds of MDD among the authors and other members of the Korea ILD Study Group consisting of pulmonologists and intensivists, three patients were excluded. Those included one patient with advanced stage lung cancer who was enrolled in a clinical trial for new chemotherapy drug and another patient under use of immunosuppressants following lung transplantation due to idiopathic pulmonary fibrosis. We concluded that other possible etiologies of ILD could not be excluded with confidence in both patients. The other patient was excluded since respiratory symptoms developed five weeks after the vaccination.
The baseline characteristics of the 46 patients are summarized in Table 1. Among them, 20 (43%) patients were diagnosed with newly identified pneumonitis following COVID-19 vaccine while 17 (37%) were diagnosed with exacerbation of pre-diagnosed ILD. In nine (20%) patients, the pre-existence of ILD could not be determined due to a lack of chest radiographs preceding vaccination. The median age was 66 (IQR, 58–73) years and 28 (61%) patients were men. The most common vaccines were BNT162b2 and ChAdOx1 nCov-19/AZD1222 each in 21 patients, followed by mRNA-1273 in three, and Ad26.COV2.S in one patient. Half of the patients (54%) experienced development or exacerbation of ILD after the first dose of vaccination. All patients denied previous history of COVID-19 infection and were tested negative for coronavirus PCR at the time of presentation. No patient had current or recent history of treatment with drugs of potential pulmonary toxicity or thoracic radiotherapy. In addition, there was no patient with recent changes in types of cigarettes or use of e-cigarettes or vaping products. Common symptoms were dyspnea (96%) and cough (67%). Twenty-three (50%) patients suffered from hypoxemia and six (13%) patients required mechanical ventilation. The serum KL-6 level was tested in 20 patients, with a median of 1,035 (IQR, 617–1,514) U/mL. Sputum gram stain and culture yielded positive result in one patient. In a patient with newly identified pneumonitis, Citrobacter freundii was cultured from the sputum collected on the day of admission; however, no pathogen was cultured from BAL performed on the same day, suggesting the possibility of contamination. Chest CT scans were available for review in all patients. The most predominant feature was ground-glass opacity which was present in 98% of the study patients. Consolidation and interlobular septal thickening were also observed in 31 (67%) and 14 (30%) patients, respectively. The abnormalities were distributed bilaterally in all but one patient and diffusely in 35 (76%) patients (Fig. 1).
Table 1
Characteristics of 46 patients with COVID-19 vaccine-associated interstitial lung disease
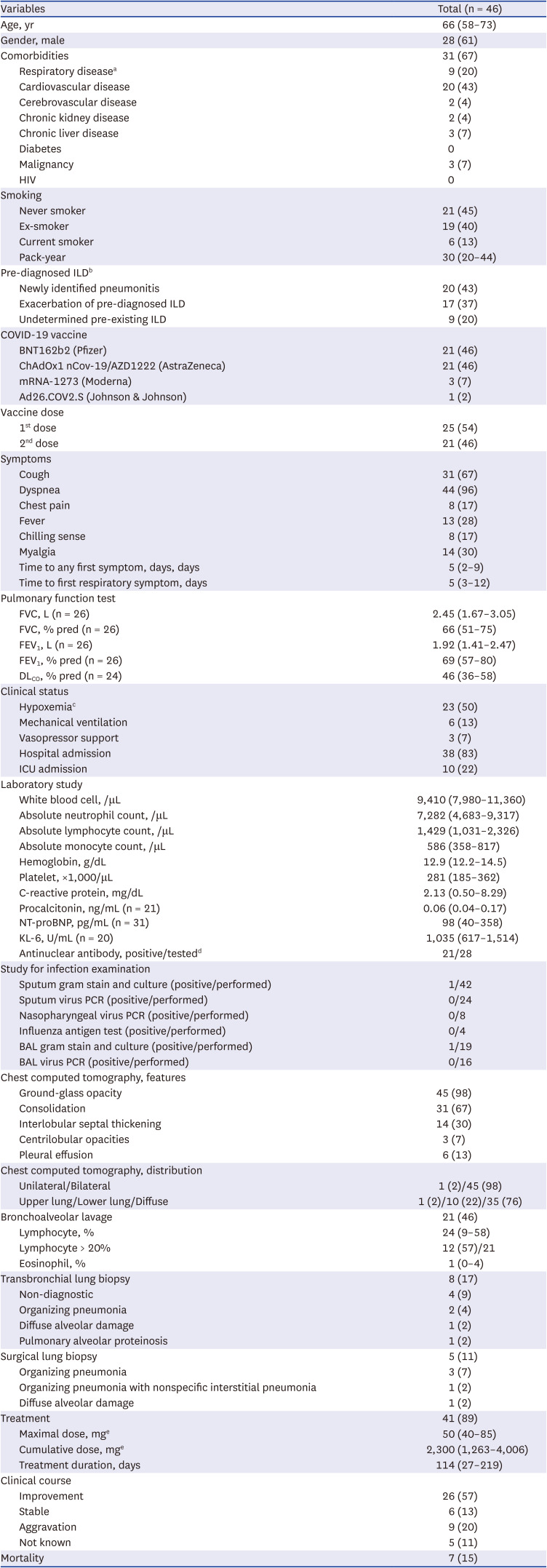
Data are presented as median with interquartile ranges or numbers (%).
COVID-19 = coronavirus disease 2019, HIV = human immunodeficiency virus, ILD = interstitial lung disease, FVC = forced vital capacity, FEV1 = forced expiratory volume in 1 second, KL-6 = Krebs von den Lungen-6, PCR = polymerize chain reaction, BAL = bronchoalveolar lavage.
aRespiratory diseases other than interstitial lung disease.
bIdiopathic pulmonary fibrosis in 10 patients, idiopathic nonspecific interstitial pneumonia in 2 patients, suspicious of idiopathic pulmonary fibrosis in 2 patients, interstitial lung disease associated with rheumatoid arthritis in 1 patient, interstitial lung disease associated with Sjogren’s syndrome in 1 patient, interstitial lung abnormalities in 1 patient.
cHypoxemia was defined as oxygen saturation below 90% at room air or need for oxygen supplementation.
dAntinuclear antibody titer of higher than or equal to 1:40 was regarded as positive.
eDose was converted to prednisolone equivalent dose.
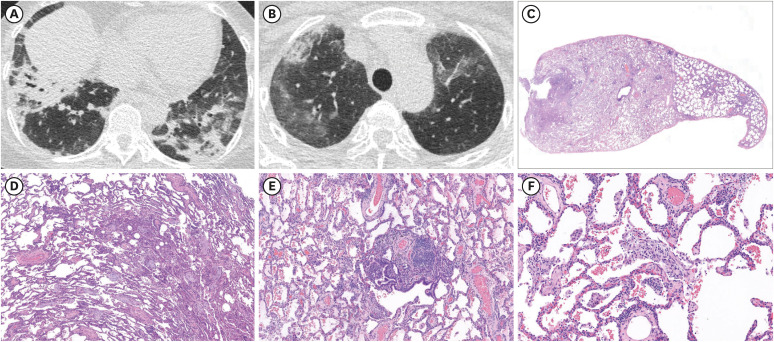
Fig. 1
Chest high-resolution computed tomography and histopathology of vaccine-associated interstitial lung disease in a 56-year-old female patient who received the first dose of BNT162b COVID-19 vaccine. Axial (panel A and B) high-resolution CT images show bilateral patch consolidation along bronchovascular bundles in lower lung zones and ground-glass opacities in upper lung zones. Lung specimen (panel C, H&E stain, ×1 original magnification) obtained by surgical biopsy. Lower power magnification (panel E and D, H&E stain, ×15 magnification) demonstrates multiple fibroblastic plugs in alveolar sacs (organizing pneumonia pattern) and uniform interstitial inflammation and thickening with lymphocytes (cellular nonspecific interstitial pneumonia pattern). High-magnification (panel F, H&E stain, ×100 magnification) shows lymphocyte infiltration in interstitium.
Bronchoscopy and surgical lung biopsy
BAL was performed in 21 (46%) patients (Table 1). Gram culture for BAL fluid grew Streptococcus mitis/oralis in one patient which was regarded as contamination based on clinical features. The median of lymphocyte and eosinophil percentages were 24% (IQR, 9–58%) and 1% (IQR, 0–4%), respectively. The proportion of patients with BAL lymphocytosis (> 20%) was 57% (12 of 21). Among them, eight patients underwent concomitant TBLB. Obtained tissue was non-diagnostic in four patients. In the other four patients, TBLB provided patterns consistent with organizing pneumonia in two patients, diffuse alveolar damage in one patient, and pulmonary alveolar proteinosis in one patient. SLB was performed in five patients. Organizing pneumonia was observed in three patients while organizing pneumonia with nonspecific interstitial pneumonia overlap pattern was found in another patient. A review of specimen revealed diffuse alveolar damage in one patient.
Treatment and outcomes of patients
Forty-one (89%) patients received corticosteroid treatment, while five patients with mild disease improved spontaneously without treatment. Patients received either methylprednisolone or prednisolone. Median of maximal dose was 50 (40–85) mg in equivalent to prednisolone. Median of duration of treatment was 114 (27–219) days. A notable improvement was observed in 26 (57%) patients including four patients without corticosteroid treatment. Six patients remained stable. These included five patients who were treated with corticosteroid but without significant improvement. One patient with pulmonary alveolar proteinosis did not receive treatment. Pneumonitis was aggravated in nine (20%) patients despite treatment.
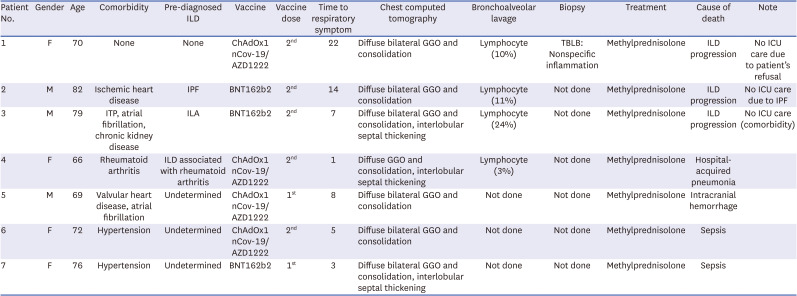
Mortality was observed in seven (15%) patients. The details of patients with mortality are described in Table 2. Of the seven deceased patients, pneumonitis occurred in one patient after the second dose of ChAdOx1 nCov-19/AZD1222 (Patient No. 1). The patient died of respiratory failure due to the progression of pneumonitis. Two patients with pre-diagnosed ILD of idiopathic pulmonary fibrosis and interstitial lung abnormalities experienced exacerbation of ILD following the second dose of BNT162b2 leading to respiratory failure (Patients No. 2 and 3). Neither patient received ICU care, considering the underlying diseases and patients’ refusal. Vaccination with the second dose of ChAdOx1 nCov-19/AZD1222 led to exacerbation of ILD in a patient with rheumatoid arthritis and ILD. Her death resulted from hospital-acquired pneumonia (Patient No. 4). Finally, three patients with undetermined pre-existing ILD died of sepsis or intracranial hemorrhage after vaccination with ChAdOx1 nCov-19/AZD1222 (Patients No. 5, 6, and 7).
Table 2
Characteristics of seven patients with mortality
Subgroup analysis based on pre-existing ILD and types of vaccines
The baseline characteristics and outcomes of 20 patients with newly identified pneumonitis, 17 patients with exacerbation of pre-diagnosed ILD, and nine patients with undetermined ILD are illustrated in the appendix (Supplementary Table 1). There were no significant differences in clinical characteristics and outcomes between patients who received mRNA vaccines and vector-based vaccines (Supplementary Table 2).
DISCUSSION
This nationwide survey identified 46 patients who were diagnosed with pneumonitis (the development or exacerbation of ILD) associated with the COVID-19 vaccine after careful exclusion of other possible etiologies. There were 20, 17, and 9 patients with newly identified pneumonitis, exacerbation of pre-diagnosed ILD, and undetermined pre-existing ILD, respectively. The common vaccines were BNT162b2 and ChAdOx1 nCov-19/AZD1222 each in 21 patients, followed by mRNA-1273 in three patients, and Ad26.COV2.S in one patient. The common symptoms were dyspnea and cough. The median interval between vaccination and onset of respiratory symptoms was 5 days. While five patients improved spontaneously without treatment, 41 (89%) patients received corticosteroid treatment. The majority of patients improved following treatment; however, nine patients progressed despite treatment. Death occurred in seven patients.
Several cases of COVID-19 vaccine-associated pneumonitis have been reported to this date. These include cases of eosinophilic pneumonia, hypersensitivity, or other ILDs accountable to either BNT162b or ChAdOx1 nCov-19/AZD1222.8910111213141516 Regarding mRNA-1253 vaccine, Yoshimura et al.17 described a case of an 88-year-old female with dyspnea following 2nd dose of mRNA-1253 whose postmortem lung specimen revealed proliferative stage of diffuse alveolar damage. To our knowledge, pneumonitis following Ad26.COV2.S vaccination has not been reported in the literature. Our nationwide survey study identified 46 patients with pneumonitis associated with the COVID-19 vaccine of various types. The results of our study as well as those of previous case reports provide compelling evidence of pneumonitis as possible and significant adverse event of COVID-19 vaccine and warrant further investigation. Of note, we report cases of not only newly identified pneumonitis but also exacerbation of underlying ILD following COVID-19 vaccination. Recently, Sgalla et al.18 observed that, among ten patients with acute exacerbation of idiopathic pulmonary fibrosis from their center, acute exacerbation occurred a few days after COVID-19 vaccination with BNT162b vaccine in four patients, suggesting COVID-19 vaccine as a potential trigger. Our study demonstrated patients with acute exacerbation of IPF and other ILDs such as idiopathic nonspecific interstitial pneumonia, ILD associated with CTDs, or interstitial lung abnormalities after COVID-19 vaccination. The result suggests that COVID-19 vaccine may be a trigger of acute exacerbation of IPF as well as other chronic ILDs.
The mechanism of pneumonitis associated with the COVID-19 vaccine is currently unknown. Various mechanisms may be involved in the pathogenesis of drug-induced pneumonitis.1920 Cytotoxic pulmonary injuries to pneumocytes or alveolar endothelium may be elicited by drugs, which are the cases for bleomycin or nitrofurantoin. Immune-mediated injuries, especially T cell-mediated reactions, are another possible mechanism of drug induced pneumonitis. Lymphocytosis observed in the BAL fluid analysis, histopathologic features of organizing pneumonia with or without nonspecific interstitial pneumonia in majority of patients available for review, and favorable response to corticosteroid in most cases in our study suggest an immune-mediated lung injury as a possible mechanism for COVID-19 vaccine-associated pneumonitis.192021 However, due to the retrospective nature of this study, we were not able to measure antibody or cytokine levels and confirm evidence for this speculation. An intriguing theory may be vaccine-induced autoimmunity. Although the manifestations and organs of injury were different, both mRNA and vector vaccines have been associated with autoimmune diseases such as arthritis, hepatitis, and Guillain-Barre syndrome.72223 Of note, the occurrence of pneumonitis in diverse vaccines of different platforms and compounds implies that the provocation of pneumonitis by COVID-19 vaccine may not be attributable to a single substance or mechanism. Interestingly, a recent study reported that SARS-CoV-2 spike protein, the main substrate of COVID-19 vaccines, induces inflammatory cytokines and chemokines.24 Spike protein itself may be the cause of hyperinflammation following COVID-19 vaccination. Nonetheless, as spike protein sequences are slightly different among vaccines, additional research is necessary to draw any conclusions.25 Future in vivo and in vitro studies are mandatory to clarify the mechanism of lung injury in COVID-19 vaccine-associated pneumonitis.
Several findings of our study require further attention. First, four vaccines were associated with pneumonitis in our study; BNT162b2 and ChAdOx1 nCov-19/AZD1222 were the most common followed by mRNA-1273, and Ad26.COV2.S. At the time of this investigation, these four vaccines were the only ones approved by the Korean Ministry of Food and Drug Safety. Considering that BNT162b2 is the most administered vaccine in 21,989,229 people followed by ChAdOx1 nCov-19/AZD1222 in 11,106,999 people, mRNA-1273 in 6,555,064, and Ad26.COV2.S in 1,484,764 people as of November 1, the frequency of vaccines in our study may reflect the number of vaccination cases rather than the tendency of specific vaccine for inducing pneumonitis. Nonetheless, most previous case reports from worldwide were on patients associated with mRNA vaccine of BNT162b2 while cases of other vaccines were scarce.810111318 It is currently not clear whether this preference results from the pathophysiology of vaccine associated pneumonitis or reporting differences. Second, the clinical characteristics of our study patients may contribute to understanding the features of vaccine-associated pneumonitis and establishing monitoring strategies. Based on our results, educating the vaccinated to observe dyspnea and cough, especially for the first week after vaccination, and advising to seek medical care if such symptoms develop seem to be a reasonable approach. In the same context, informing clinicians of pneumonitis as a possible adverse reaction of the COVID-19 vaccine and its clinical features is required, since clinical suspicion and careful exclusion are crucial in the diagnosis and differentiation of ILD. Furthermore, in half of the patients, pneumonitis occurred after the second dose of vaccination. Therefore, the absence of vaccine-associated pneumonitis from the first dose should not preclude the necessity of monitoring for pneumonitis in subsequent vaccinations. Third, although organizing pneumonia pattern was common, we could not observe pathologic features specific to vaccine-associated pneumonitis. The numbers of patients are too small to draw firm conclusion on significance of or establish indication for biopsy. Pathology may provide helpful information in differential diagnosis; however, complications of biopsy should be considered before making a decision. Further studies are necessary to determine the necessity and impact of biopsy in vaccine-associated pneumonitis. Forth, although most patients responded favorably to corticosteroid treatment, seven patients died in our study. Of them, four patients died of causes other than pneumonitis (Table 2). The deaths of the remaining three patients, including two patients with pre-diagnosed ILD, were due to the progression of pneumonitis. Further investigations on the precise incidence, risk factors, and mortality rate are mandatory to determine the risk and benefit of COVID-19 vaccination and establish recommendations for specific populations. However, results of our study should not be interpreted as signal for undermining the importance of vaccines against SARS-CoV-2. Vaccines have clearly shown to reduce not only the risk of transmission but also the risks of hospitalization and severe illness in both clinical trials and real-world settings.426 Furthermore, given the fact that the risks of COVID-19 and severe presentation are higher in patients with ILD than in those without ILD,27 the incidence of exacerbation of ILD due to vaccines for determination of risk and benefit is not yet identified, and the rather favorable response to corticosteroid treatment, the evidence is not sufficient to deter patients with ILD from COVID-19 vaccination. However, it may be rational to closely monitor for pneumonitis and inform the vaccinated individuals of the risk, especially for patients with pre-existing ILD. Finally, to date, most cases of COVID-19 vaccine-associated pneumonitis have been reported only in Asian countries. This raises the possibility of a racial or genetic vulnerability to COVID-19 vaccine-associated pneumonitis. Interestingly, most cases of influenza vaccine induced pneumonitis have been reported from Asian countries.28 Nevertheless, there is always the possibility of a reporting bias. Global epidemiological studies as well as laboratory studies, such as whole-genome single nucleotide polymorphism profiling, are needed to determine this speculation.
To fully appreciate the results of our study, several limitations should be acknowledged. First, since no single confirmative test for the diagnosis of vaccine-associated pneumonitis exists, we cannot fully validate the diagnosis of vaccine-associated pneumonitis in our study patients. Furthermore, tests for infection, which is an important differential diagnosis of vaccine-associated pneumonitis, such as respiratory virus multiplex PCR were not performed in some patients. This demonstrates the limitation of retrospective nature of the study. However, thorough history and laboratory examination for the exclusion of other possible etiologies including environmental exposures and drugs and assessment of temporal relationships were performed by each pulmonologist and/or intensivist. In addition, all the surveyees are members of the Korea ILD study group who specialize in and have robust clinical experience in diagnosis and treatment of ILD. Furthermore, clinical, radiological, and pathological data of all reported cases were thoroughly reviewed through multiple rounds of MDD before final enrollment. Second, we used four weeks as the time period for the case definition of vaccine-associated pneumonitis. Although temporal association per se does not establish causality, it is one of the key principles in defining the adverse event following vaccination.29 Therefore, accurately setting the time window is important in identifying the potential patients with adverse event and determine the incidence, thus, it should be based on factors such as clinical trials data, biological plausibility, and practical feasibility.30 Nonetheless, such evidence is lacking and current pharmacovigilance reporting guidelines do not suggest an onset interval for COVID-19 vaccine associated pneumonitis. Despite that shorter time interval may provide stronger relevance while longer time interval may help identify more potential patients, the authors chose four-week duration considering the fact that other immune mediated adverse events of COVID-19 vaccine may develop up to six weeks after vaccination (but mostly within four weeks)731 as well as drug induced pneumonitis occur commonly within four weeks,32 current definition of acute exacerbation of IPF,33 and the public recommendation by the Korean CDC to monitor for dyspnea or chest pain for four weeks of vaccination. In addition, although the authors used the onset interval for screening and possible inclusion of patients, final diagnosis of vaccine-associated pneumonitis was based on careful review of clinical, radiological, and/or pathological presentation and exclusion of other possible causes. However, possibility of underestimation of vaccine-associated pneumonitis by limiting the time interval to four weeks should be recognized. If the pathophysiology underlying the pneumonitis is due to immune-related reaction or autoimmunity, delayed presentation may be possible as seen in the cases of immune related adverse events related to immune checkpoint inhibitors.34 Thus, the authors believe that analysis of surveillance data and prospective monitoring is warranted to define the onset interval and optimal surveillance duration for vaccine-associated pneumonitis.30 Third, since this study was based on survey of pulmonologists and intensivists from major referral hospitals of Republic of Korea, there is a possibility of selection bias of including only severe cases, leading to underestimation of mild cases. Forth, although CT images were reviewed by radiologists and pulmonologists who are members of Korean ILD study group, they were performed during MDD, neither in blind nor in independent manner. Finally, although this was a nationwide survey, the prevalence and incidence of vaccine-associated pneumonitis could not be calculated as only the members of the Korea ILD Study Group were surveyed. Further national or global epidemiological research is necessary to identify the incidence of and risk factors for vaccine-associated pneumonitis.
In conclusion, clinicians should be aware that the pneumonitis (development or exacerbation of ILD) is a possible adverse reaction of COVID-19 vaccination. Close monitoring and patient education are necessary for early recognition and prompt treatment. Additional research is warranted to identify the epidemiology and characterize the pathophysiology of vaccine-associated pneumonitis.
 XML Download
XML Download