

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular disease (CVD) is one of the major causes of global mortality and morbidity. The death rate from heart diseases increased nearly 7-fold in 2016 compared with the rate in 1990. Besides, this death rate is higher than that from infectious diseases and cancer. It is predicted that this ratio of death will increase as the years pass and that it will be over 23.6 million in 2030.1)
Vitamin D (VitD) is a steroid prohormone. According to the former information, VitD was known to be effective only on calcium and phosphorus metabolism. Today, it is known that VitD regulates nearly 2,000 genes on DNA.2) Therefore, VitD is associated with many diseases by researchers. Since endothelial and cardiomyocyte cells have VitD receptors,3) CVD is one of the diseases.2) Moreover, the active form of VitD is synthesized in endothelial cells.4)
YKL-40 (chitinase 3-like protein 1) is an inflammatory biomarker. It is secreted from endothelial and vascular smooth muscle cells as well as from macrophages and neutrophils in atherosclerosis lesions.5) Compared with healthy individuals, the level of plasma YKL-40 is high in patients with CVD. It is reported that the risk of developing ischemic heart disease in the future will increases in parallel with an increase in the level of plasma YKL-40. In addition, YKL-40 levels were increased in type 2 diabetes patients with suspected coronary artery stenosis but these patients were asymptomatic for AMI. Researchers have evaluated this increase in YKL-40 released from inflammatory cells to be associated with CVD.6) Similarly, the increase in the level of plasma YKL-40 accompanies the progress of the disease, and it rises exponentially as one gets older.7) It is considered that YKL-40 has no effect on the development of CVD-related diseases; however, it could be a prognostic factor after the diagnosis of these diseases.8)
In experimental studies, it is known that VitD suppresses soluble intercellular adhesion molecule-1 (sICAM-1) and soluble vascular cell adhesion molecule-1 (sVCAM-1), and even IL6, which contribute to the development of CVD.9)10) However, there is no data on the effect of VitD on YKL-40, which is thought to be an inflammatory marker in the diagnosis of CVD in the chronic inflammatory model. According to the information just mentioned, it is necessary to investigate how the differences in serum VitD levels will affect YKL-40, the amount of which increases with the development of CVD. Our research is original in this respect. Moreover, since the real VitD deficiency will be created in the project, CVD and VitD will contribute to each other different results of the relationship.9)11) In this study, we have investigated the effect of 25(OH)VitD on serum YKL-40 levels in the chronic inflammatory process induced by a hypercholesterolemia model.
METHODS
Ethical statement
All experiments were performed in adherence with the Health Guidelines of on the Use of National Institutes Laboratory Animals, and were approved by the Necmettin Erbakan University, Experimental Animal Ethics Committee (2018-27).
Animals and ethical consideration
A total of 32 male wistar albino rats (age, 3–4 months; weight, 368±27 g) were obtained from Necmettin Erbakan University, Experimental Medicine Application and Research Center, Konya, Turkey. The animals were housed as 4 rats in each cage and with drinking water available at all times, maintained under standard conditions of temperature (22±1°C) and humidity (45±5%), in an air-conditioned room (12 full changes of air per 1 hour), with regular 12 hours light/dark cycle. Each of the rats was placed in direct exposure to light for the project time.12)
Chemicals
Cholesterol (CAS No.: 57-88-5), corn oil, which is the solvent of cholecalciferol (CAS No.: 8001-30-7) and cholecalciferol (CAS No.: 67-97-0) were purchased from Sigma-Aldrich Chemical Company (St. Louis, MO, USA).
Experimental design
After one-week acclimation period, animals were divided into 4 groups: 1st group as control (n=8), 2nd group as high-cholesterol (H-CH) adequate VitD group (H-AdeVD; n=8), 3rd group as H-CH deficient VitD group (H-DefVD; n=8), 4th group as H-CH supplement VitD (H-SupVD; n=8).
Feeding was composed of 2 stages. During the first stage (5 months), the H-DefVD group was fed on VitD deficient chow, while the other groups (control, H-AdeVD, H-SupVD) were fed on standard chow. During the second stage (3 months), the control group was fed on standard chow, whereas the H-AdeVD and H-SupVD groups were fed on the H-CH chow and the H-DefVD group was fed on the H-CH-deficient VitD chow. Moreover, during the second stage, the H-SupVD group was given 100 IU/kg/day cholecalciferol orally, while the other groups were given cholecalciferol solvent corn oil (Table 1).
Table 1
Experimental design

Diets
In this project, 4 separate dietary compositions were used. 1. Standard rat chow (Cat. No.: RT 01); 2. VitD deficient chow: standard rat chow (only without 1 IU/g cholecalciferol); 3. The H-CH chow: 1.25% cholesterol and 0.5% colic acid were added to the standard chow (wt/wt); 4. VitD deficient H-CH chow: 1.25% cholesterol and 0.5% colic acid were added to the VitD deficient chow (wt/wt). In order to prevent variations in chow’s contents, diets were prepared isocalorically (2.7 kcal/g) by adding the same feed additives and content, at the same time (DSA; Arden Research Experiment, Ankara, Turkey). All the groups were given 20±1 g/rat/a day chow to prevent obesity due to excessive chow consumption. In addition, body weight changes and Lee Index of Obesity (LIO) were calculated every 2 weeks in all the groups.13) Experimental points and experiences are given in Supplementary Data 1.
Blood sampling
Blood samples were collected under anesthesia with sevoflurane (2%). Blood was withdrawn from the jugular veins of all the rats after 4 hours of fasting, and the samples were stored in polymer gel-containing tubes (up to 1 mL blood/animal). These samples were collected in the same manner and were allowed to clot for 30 minutes before centrifugation. Then all the samples were centrifuged at 1,800×g for 10 minutes at 8°C, and they were frozen at −80°C.
Biochemical analyses
During the first stage of the study, serum 25(OH)VitD (0th, 2.5th, and 5th months) was measured in the H-DefVD group. During the second stage, serum total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglyceride (TG) and 25(OH)VitD, IL-6, sICAM-1, sVCAM-1, and YKL-40 were conducted for all the groups (5th, 6th, 7th, and 8th months). Also, serum calcium, phosphorus and parathormone analyses were conducted (0th, 5th, and 8th months).
The levels of serum TC, TG, LDL-C, HDL-C, calcium, phosphorus, parathormone and 25(OH)VitD were measured using commercially available kits based on routine methods on Architect C 8000 System (Abbott Laboratories, Abbott Park, IL, USA). IL-6, sICAM-1, sVCAM-1, and YKL-40 levels were analyzed by ELISA method with the respective kits specifically for rats according to the manufacturer’s instructions (Bioassay Technology Laboratory Rel Assay Diagnostics; Cat. No.: E0135Ra, E0418Ra, E0421Ra, E0899Ra; sequentially).
Statistical analysis
All of the data were analyzed using Statistical Package for the Social Sciences (SPSSv16.0; SPSS, Chicago, IL, USA) statistical software. Tests of normality were performed on response variables using the Shapiro-Wilk statistic. All results were given as means±standard error of mean. Multiple groups were compared using repeated-measures analysis of variance, which was followed by a Bonferroni test. Dunnett test was used for post hoc assessment of the control group and the other groups; Tukey test was utilized for the comparison of all the groups. In addition, a simple effect test was performed for each group.
RESULTS
Body weight and serum 25(OH)VitD values
All the animals continuously gained weight during the study; on the other hand, no significant difference was observed between the groups in terms of weight changes (Table 2), since LIO values were not over LIO >0.3, which is considered obesity (data were not shown).
Table 2
Body weight, serum calcium, phosphorus, and parathormone parameter values
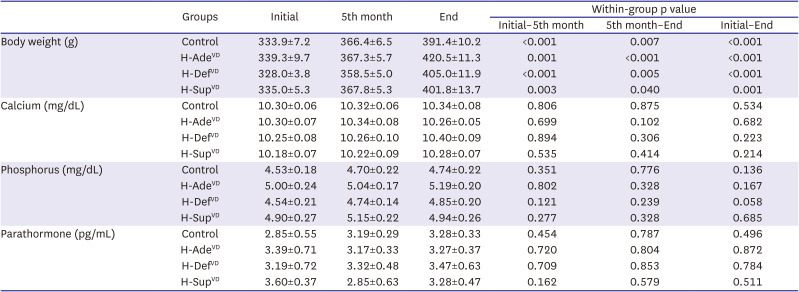
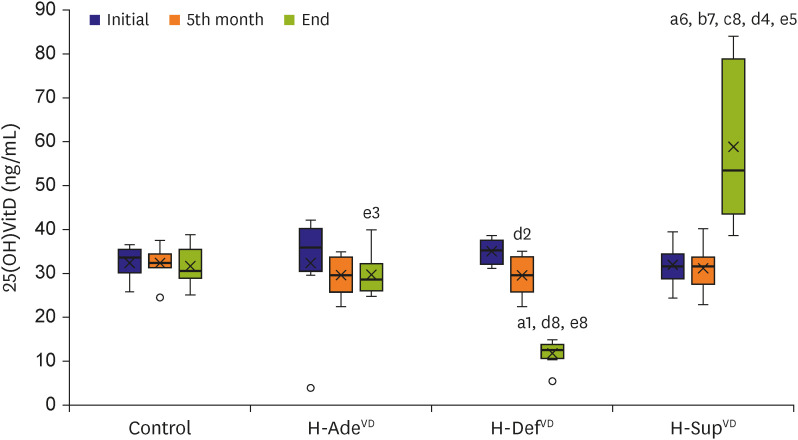
The decrease in the averages of serum 25(OH)VitD values in the H-DefVD at the end of the study in comparison with those at the beginning of the project (p<0.001) was found significant. Also, the decrease in the levels of 25(OH)VitD in the H-AdeVD group (p=0.016) and the increase in the H-SupVD group (p=0.010) were found to be significant at the end of the study compared with the values in the 5th month. In the evaluation between groups, the decrease in the averages of the levels of serum 25(OH)VitD in the H-AdeVD group (29.6 ng/mL) was not significant compared with the control group (31.4 ng/mL), whereas the decrease in the H-DefVD group (11.3 ng/mL), (p=0.05) and the increase in the H-SupVD group (59.1 ng/mL) was found significant (p=0.008) (Figure 1). There were no significant differences in serum calcium, phosphorus, and parathormone parameters both in intra-group and inter-group assessments (Table 2).
Figure 1
Serum 25(OH)VitD values. Groups were compared using repeated-measures analysis of variance between groups and within groups values.
H-AdeVD = high-cholesterol adequate vitamin D group; H-DefVD = high-cholesterol deficient vitamin D group; H-SupVD = high-cholesterol supplement vitamin D group; 25(OH)VitD = 25(OH) vitamin D.
Different superscripts indicate significant difference (lowercase letters: control, H-AdeVD, H-DefVD, initial, 5th month; number: p=0.05, p=0.045, p=0.016, p=0.011, p=0.01, p=0.008, p=0.001, p<0.001).
Lipid panel values
Serum TC, LDL-C and TC/HDL-C values significantly increased in the H-CH fed groups (H-AdeVD, H-DefVD and H-SupVD) at the end of the study compared to both within the group and control group (Table 3).
Table 3
Serum lipid panel parameter values
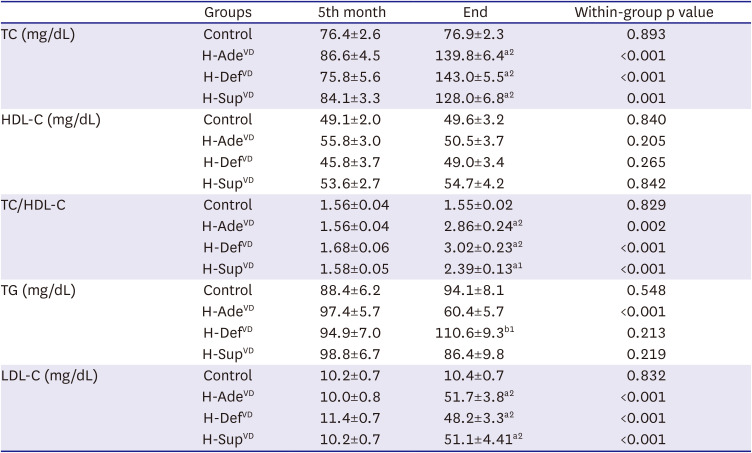
Groups were compared using repeated-measures analysis of variance between groups and within groups values.
H-AdeVD = high-cholesterol adequate vitamin D group; H-DefVD = high-cholesterol deficient vitamin D group; HDL-C = high-density lipoprotein cholesterol; H-SupVD = high-cholesterol supplement vitamin D group; LDL-C = low-density lipoprotein cholesterol; TC = total cholesterol; TG = triglyceride.
Different superscripts indicate significant difference (lowercase letters: control, H-AdeVD, H-DefVD; number: p<0.05, p<0.001).
In intra-group evaluation, serum TG values decreased significantly in the H-AdeVD group at the end of the study compared with the values in 5 months (p<0.001). The decrease in TG levels in the H-AdeVD group was found to be significant compared with the H-DefVD group (p<0.05) (Table 3).
YKL-40 and other values
IL-6, sICAM-1, sVCAM-1 and YKL-40 values increased significantly in the H-AdeVD and H-DefVD groups at the end of the study according to intra-group evaluation. IL-6, sICAM-1 and sVCAM-1 values in the H-AdeVD and H-DefVD groups significantly increased in inter-group evaluation compared with control group ([p<0.05, p<0.05, p=0.05], [p<0.001, p<0.001, p=0.009]; sequentially). Also, YKL-40 value in the H-DefVD group increased significantly compared with control group (p=0.005) (Figures 2 and 3).
Figure 2
Serum IL-6, sICAM1 and sVCAM1 parameter values. Groups were compared using repeated-measures analysis of variance between groups and within groups values.
H-AdeVD = high-cholesterol adequate vitamin D group; H-DefVD = high-cholesterol deficient vitamin D group; H-SupVD = high-cholesterol supplement vitamin D group; IL-6 = interleukin-6; sICAM1 = soluble intercellular adhesion molecule-1; sVCAM1 = soluble vascular cell adhesion molecule-1.
Different superscripts indicate significant difference (lowercase letters: control, H-AdeVD, H-DefVD, 5th month; number: p<0.05, p=0.05, p=0.005, p=0.001, p<0.001).
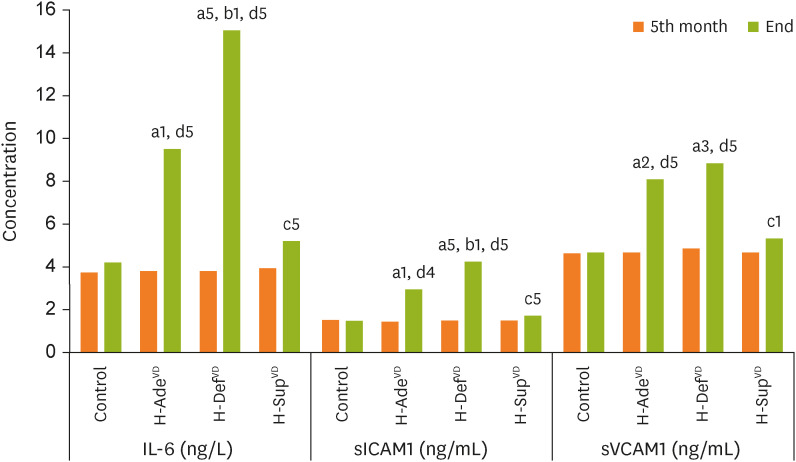
Figure 3
Serum YKL-40 values. Groups were compared using repeated-measures analysis of variance between groups and within groups values.
H-AdeVD = high-cholesterol adequate vitamin D group; H-DefVD = high-cholesterol deficient vitamin D group; H-SupVD = high-cholesterol supplement vitamin D group.
Different superscripts indicate significant difference (lowercase letters: control, H-DefVD, 5th month; number: p<0.05, p=0.055, p=0.007, p=0.005, p=0.001).
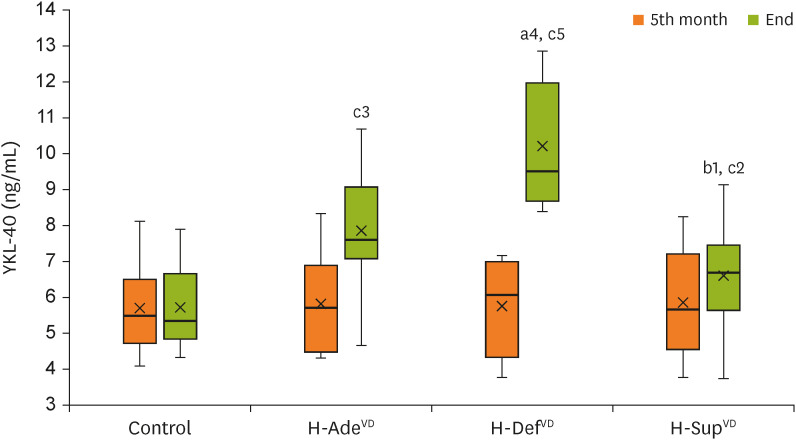
In comparison with the H-AdeVD group, IL-6, sICAM-1 values increased significantly in the H-DefVD group (p<0.05, p<0.05; respectively). Compared with the H-SupVD group, IL-6, sICAM-1, sVCAM-1 and YKL-40 values increased significantly in the H-DefVD group (p<0.001, p<0.001, p<0.05, p<0.05; sequentially) (Figure 2).
DISCUSSION
In this study, the effect of VitD on YKL-40 was evaluated in an experimental hypercholesterolemia pattern. In the project, in order to increase the differences in serum VitD levels between groups, the H-DefVD group was fed with a VitD deficient chow, while the H-SupVD group was given additional VitD. The first stage of the feeding was conducted because VitD is stored in fat tissue and released very slowly to blood during the deficiency of VitD until depletion.12)14) The levels of serum calcium, phosphorus and parathormone were monitored in the experiment. These parameters didn't make a statistically significant difference between the groups. In other words, toxicity and/or secondary hyperparathyroidism related to VitD did not develop (Table 2). As a result of VitD deficient nutrition and VitD supplementation, according to the baseline 25(OH)VitD values, the expected decrease in the H-DefVD group, and the desired increase in the H-SupVD group were observed. The 25(OH)VitD values in our study are consistent with the studies in the literature with a similar nutritional pattern.11)12)15)
In our study, H-AdeVD, H-DefVD, and H-SupVD groups were fed with 1.25% ratio of cholesterol chow for 12 weeks to create chronic inflammation due to H-CH.15) Although the highest increase in serum TC values was in the H-DefVD group (143.0±5.5 mg/dL) and the lowest increase in the H-SupVD group (128.0±6.8 mg/dL), there was no significant difference between the groups. In our previous study, we investigated the effect of VitD on serum TC levels in a hypercholesterolemia rabbit model and it was found that a reducing effect of VitD on serum TC was observed at much higher serum TC values when rabbits were fed with H-CH diet groups. That is, while serum TC levels increased to 1,312±648 mg/dL in the group fed with H-CH diet, it increased to 726±246 mg/dL in the group fed with H-CH diet and supplemented with VitD, and there was a significant difference between the 2 groups (p<0.05). However, in the groups fed with normal rabbit chow of the same study, serum TC value was decreased (35.0±12.4 mg/dL) in the VitD supplemented group compared to the control group (46.0±17.1 mg/dL), but it was not statistically significant.16) Therefore, considering the current study, a cholesterol-lowering effect of VitD may be minimal17) because there was no significant difference between the H-CH fed groups in this project (Table 3). Besides, according to the data, VitD may have a cholesterol-lowering effect by increasing cholesterol efflux (CYP27A1 activation).14)
The decrease in serum TG level of H-AdeVD group was statistically significant at the end of the study when compared to the H-DefVD group. Although this was an unexpected result, it could be explained by the coprophagy behavior of the rats.18) It is well known that rat feces contain fatty acids and some vitamins. These fatty acids could also have affected TG levels. Likewise, animals in the H-DefVD group showed more feeding behavior than the other groups.18) Both the significant decrease in TG levels in the H-AdeVD group and the significant increase in the H-DefVD group could have resulted from coprophagy when compared to each other (Table 3).
In the physiological process, the endothelium protects vessels. Owing to this protective mechanism, blood vessels remain in a constant state of vasodilation. Nitric oxide (NO) is primarily responsible for endothelium-dependent vasodilation. VitD, on the other hand, activates immune system cells and decreases the expression of proinflammatory cytokines such as IL-610) and IL-1β4) that will occur in endothelial cells. In our study, we are of the opinion that VitD protects the vessels from endothelial damage by stimulating immune system cells,4) increasing NO synthesis,19) and suppressing the expression of proinflammatory cytokines.4) In addition, there are data indicating that VitD activates the Apelin/APJ system and suppresses the synthesis of proinflammatory cytokines and adhesion molecules.9) Conversely, in the chronic inflammatory process, it has also been known that intima-media thickness increases, atheromatous plaques form and as a result, adhesion molecules such as sCAM-1 and sVCAM-1 increase.15)20)21)
As mentioned in the upper paragraph, it was seen in the intergroup evaluation in our study that there is no significant difference between the H-AdeVD, H-DefVD, and H-SupVD groups, although the least increase in serum TC values was observed in the H-SupVD group. In fact, chronic inflammation in these 3 groups was expected to be close to each other. However, there was a significant decrease in IL-6, sCAM-1 and sVCAM-1 values in the H-SupVD group compared to the H-DefVD group. We assumed that the protection against this chronic inflammation is due to the VitD difference between the groups. Besides, serum TC levels were found to be lower in the H-SupVD group than in the H-DefVD group. Based on this information (albeit to a small decrease in serum TC level) we assume that VitD reduces CVD risk factors in addition to chronic inflammation (Table 3).
Considering the data of the 5th month in the H-AdeVD group, we see that the serum VitD levels decreased significantly at the end. Although, the reason of this decrease is not clear, it can be due to the increase in serum TC levels. Moreover, because of the decrease in VitD level in H-AdeVD group, there is no significant difference between H-AdeVD and H-DefVD groups based on YKL-40 level (Figure 1).
In a similar way, we can conclude that VitD may also suppress the YKL-40 expression. There are a limited number of studies in the literature on the relationship between VitD and YKL-40. In a study with the patients with type II diabetes, it was shown that YKL-40 level was decreased with the VitD supplementation.22) In addition, it has been reported that the increase in YKL-40 levels as a result of endothelial damage and inflammation in kidney transplant patients may contribute to CVD complications.23) Furthermore, YKL-40 is associated with other diseases (such as liver, acute infectious disease, etc.).5) It is also stated that YKL-40 could be a useful biomarker in the diagnosis and follow-up of chronic obstructive pulmonary disease.24) Although it needs further investigation, it is thought that the inhibition of YKL-40 can be a new treatment method in CVD.8)25)
Limitations of the research: The study was an animal model and new biomarkers considered CVD risk factors could be added to the study.
In the light of the literature and according to our results, VitD may have suppressed YKL-40 by suppressing IL-6, sCAM1 and sVCAM1, that is, by suppressing the inflammatory process9)26) and/or affecting VitD and YKL-40-related metabolic pathways.8)27) Although there are different results about VitD’s ability to prevent CVD, YKL-40, which is increased in the development and follow-up of VitD CVD, is suppressed. If the accumulated evidences or clinical trials for humans comes out, the effect of VitD and YKL-40 on development of CVD will be understood well and, how the treatment can be applied to prevent it.
 XML Download
XML Download