

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sleep state misperception, characterized by a discrepancy between subjective and objective assessments of sleep, is common in patients with insomnia.12 The typical example is paradoxical insomnia, in which patients have a marked propensity to underestimate the amount of sleep they are actually obtaining.3 Therefore, such patients may perceive themselves as awake during much of the time in which they are actually sleeping. Sleep state misperception can also occur in other sleep disorders such as obstructive sleep apnea (OSA).45 The frequent co-occurrence of insomnia and insomnia symptoms with OSA may contribute to sleep-wake misperception in patients with OSA.6
Unlike sleep state misperception presenting as an underestimation of sleep in patients with insomnia,13 the literature shows a wide range of sleep state misperceptions in patients with OSA.7 Patients with OSA may underestimate or overestimate their sleep duration compared to that measured by polysomnography (PSG).489 A recent study of patients with OSA showed that sleep underestimation was associated with comorbid insomnia symptoms whereas sleep overestimation was associated with sleep apnea severity.10
While the mechanisms underlying sleep state misperception are largely unknown, particularly in patients with OSA, misperception might be partly influenced by various psychological, cognitive, and physiological factors.111213 One popular hypothesis is that misperception is related to fragmentation of sleep architecture, in which light sleep stage or high frequencies of awakenings might result in an underestimation of sleep duration.9 The results of studies using neuroimaging or sleep electroencephalograph (EEG) spectral analysis techniques suggested that an altered sleep/wake arousal system may explain the apparent mismatch between objective sleep measures and subjective sleep reports.141516 However, evidence is lacking regarding the relationship between the degree of sleep misperception and stage N1 duration, the degree of fragmentation, or other metrics of sleep-wake stage composition.717
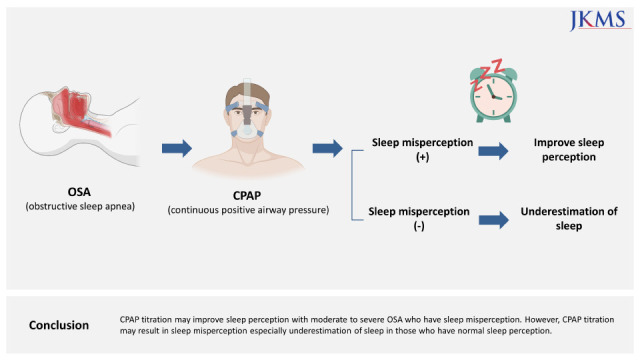
Continuous positive airway pressure (CPAP), considered the gold standard therapy for patients with moderate to severe OSA, delivers pressurized air into the upper airway to relieve obstruction during sleep.18 CPAP improves nighttime symptoms such as snoring, apnea, awakening, and nocturia, consequently preventing a disruption of sleep architecture and improving the quality of sleep. Given these benefits, CPAP might also improve sleep perception. Castillo et al.9 suggested that sleep-wake misperception might improve with CPAP treatment of OSA in patients who also exhibit misperception. However, the available literature on such effects is scarce. Therefore, the present study aimed to examine the effects of CPAP on sleep state misperception in patients with moderate to severe OSA who underwent CPAP titration studies.
METHODS
Patients
This retrospective database study analyzed data from patients who visited the sleep laboratory at Asan Medical Center for the evaluation of snoring and sleep apnea between April 2015 and January 2018. The inclusion criteria were age > 19 years, diagnosis with OSA (apnea-hypopnea index [AHI] of ≥ 5 per hour of sleep on diagnostic PSG), undergoing a subsequent full-night CPAP titration study, and the completion of a battery of sleep-related questionnaires. The exclusion criteria were as follows: a total sleep time (TST) of < 120 minutes as measured by diagnostic or CPAP titration PSG, undergoing a split-night study, an interval of > 1 year between diagnostic and CPAP titration PSGs, an AHI of ≥ 15 on CPAP titration study, or incomplete data. Basic demographic information (age, sex, height, and weight), medical comorbidities (past and current medical, psychiatric, and surgical histories), and medication information (antidepressant and antipsychotic use) were obtained from the self-reported medical history checklist and electronic medical records.
PSG
Two separate full-night standard PSGs with synchronized video were performed for the diagnosis of OSA and then for CPAP titration at a sleep laboratory. Sleep and respiratory events were scored according to the 2012 American Academy of Sleep Medicine manual.19 The variables of sleep architecture included TST (N1, N2, N3, and rapid eye movement [REM] sleep), sleep onset latency, wake after sleep onset (WASO), and sleep efficiency. An apnea episode was defined as a drop in the peak thermal sensor excursion by at least 90% of the pre-event baseline for at least 10 seconds. Hypopnea was defined as a drop in the nasal pressure signal by at least 30% of the pre-event baseline for at least 10 seconds, with at least a 3% reduction in O2 saturation or arousal. The AHI was defined as the average number of apnea and hypopnea episodes per hour of sleep.
CPAP was manually titrated until the lowest effective CPAP level was reached based on clinical guidelines.20 The starting CPAP was 4 cmH2O and the pressure was increased by at least 1 cmH2O after 5 minutes or more. CPAP was increased if there were two obstructive apneas, three hypopneas, five respiratory effort-related arousals, or at least 3 minutes of loud or unambiguous snoring.
Sleep state perception
Post-sleep questionnaires were completed in the morning after an overnight PSG. The patients were asked to subjectively assess their TST, sleep onset latency, and WASO in the last night. Sleep state misperception was quantified by subtracting the objective PSG-measured TST from the subjective sleep duration obtained by the post-sleep questionnaire.9 Thus, negative values indicated that the subjective response was an underestimate, while positive values indicated that the subjective response was an overestimate. Using the cutoff values of ± 60 minutes of sleep state misperception, the categories with normal, underestimated, and overestimated sleep state perception were defined as differences of −60 to +60 minutes, < −60 minutes, and > +60 minutes, respectively.9
Questionnaires
The validated Korean version of the Epworth Sleepiness Scale (ESS) consists of eight questions asking how often an individual dozes during daily activities.21 Each answer was rated on a four-point scale, with a total possible score ranging from 0 to 24. Higher scores represent a greater propensity toward sleeping during the day. An ESS score of ≥ 11 is indicative of excessive daytime sleepiness.
The validated Korean version of the Beck Depression Inventory (BDI) consists of 21 items rated on a four-point scale (0–3), with a total possible score ranging from 0 to 63.22 Higher scores represent a higher level of depression. A BDI score of ≥ 17 was considered indicative of moderate to severe depression.
Insomnia symptoms were defined as present if a patient had any one of three insomnia complaints at least one time per week: 1) difficulty falling asleep, 2) difficulty maintaining sleep (i.e., waking during the night and having difficulty getting back to sleep), and 3) waking too early in the morning and unable to get back to sleep.23
Statistical analysis
Data are presented as the means and standard deviations, the median and interquartile ranges, or numbers and percentages, and were compared using one-way analysis of variance, Spearman correlation tests, Wilcoxon signed-rank tests, or Mann-Whitney U tests, as appropriate. All statistical tests were two-tailed, and P < 0.05 was considered statistically significant. Statistical analyses were performed using the IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Patients
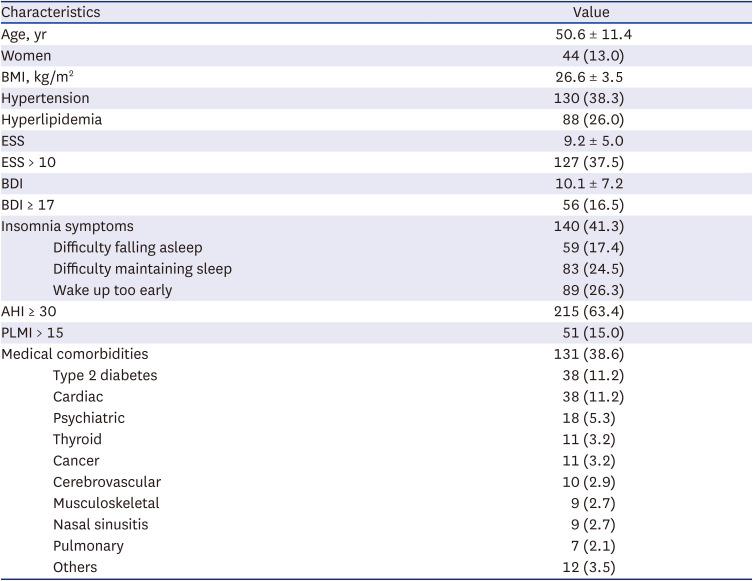
Of the 355 patients enrolled, 16 were excluded for AHI ≥ 15 on a CPAP titration study (n = 1), an interval of > 1 year between diagnostic and CPAP titration studies (n = 1), and no post-sleep questionnaires after diagnostic PSG (n = 8) or CPAP titration PSG (n = 6). The characteristics of the 339 subjects included in the study are shown in Table 1. The mean age of the patients was 50.6 ± 11.4 years, and 44 patients (13.0%) were female. Severe OSA was observed in 215 (63.4%) patients. Insomnia symptoms were noted in 140 (41.3%) patients, 28 (8.3%) and 35 (10.3%) of whom had two and all three symptoms of insomnia, respectively. The intervals between diagnostic and CPAP titration studies were within 4 weeks in 22.4% (n = 76) of patients, 4–8 weeks in 50.1% (n =170), 8–12 weeks in 18.0% (n = 61), 12–24 weeks in 6.8% (n = 23), and 24–48 weeks in 2.7% (n = 9).
Table 1
Patient characteristics (N = 339)
Sleep state perception in diagnostic and CPAP titration studies
Compared to the diagnostic study, significant improvements in sleep apnea and sleep architecture were observed in the CPAP titration study (Table 2). The median value of the difference between subjective and objective TST was lower in the CPAP titration study than that in the diagnostic study (P < 0.001), indicating a greater degree of underestimation of sleep duration in the CPAP titration study (Table 2). The differences in sleep onset latency and WASO did not differ between subjective and objective measures (P > 0.05).
Table 2
Sleep architecture, apnea parameter, and sleep perception in a diagnostic and CPAP titration PSG (N = 339)
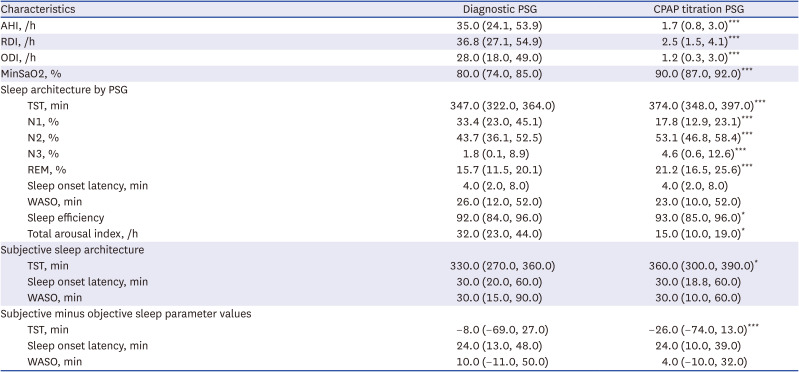
Data are presented as median and interquartile range.
AHI = apnea-hypopnea index, CPAP = continuous positive airway pressure, MinSaO2 = minimal arterial oxygen saturation, ODI = oxygen desaturation index, RDI = respiratory disturbance index, PSG = polysomnography, TST = total sleep time, REM = rapid eye movement, WASO = wake after sleep onset.
*P < 0.05; ***P < 0.001 between diagnostic and CPAP titration studies by Wilcoxon signed-rank tests.
We further subdivided sleep state perception (Table 3). Comparing to the diagnostic study, greater underestimation of sleep duration during CPAP titration was observed in each of the groups with no insomnia symptoms, BDI score < 17, and ESS score ≥ 11 but not in the groups with insomnia symptoms, BDI score ≥ 17, and ESS score < 11 (Table 3). In contrast, TST was more underestimated in the CPAP titration study regardless of categories including age > 60 years, sex, AHI ≥ 30, and periodic limb movements index > 15. In addition, each of the groups with insomnia symptoms and BDI score ≥ 17 had greater TST underestimation than those in patients without insomnia and BDI score < 17, respectively, in a diagnostic PSG.
Table 3
Comparisons of sleep perception between diagnostic and CPAP titration PSG according to patient age, sex, and clinical factors (N = 339)
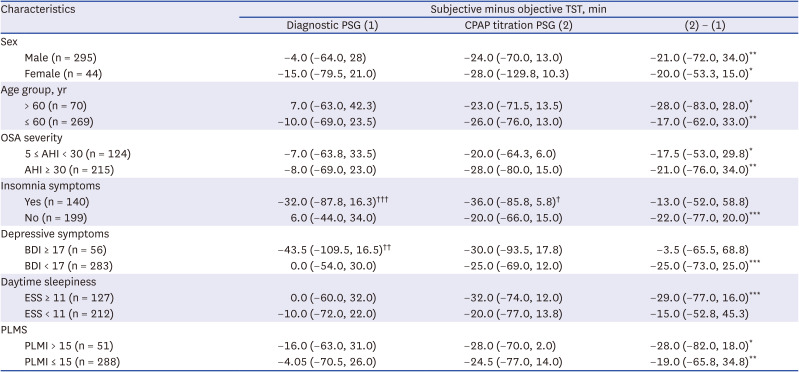
Data are presented as median and interquartile range.
AHI = apnea-hypopnea index, BDI = Beck Depression Inventory, CPAP = continuous positive airway pressure, ESS = Epworth Sleepiness Scale, OSA = obstructive sleep apnea, PLMI = periodic limb movements index, PLMS = periodic limb movements during sleep, PSG = polysomnography, TST = total sleep time.
*P < 0.05; **P < 0.01; ***P < 0.001 between diagnostic and CPAP titration studies by Wilcoxon signed-rank tests.
†P < 0.05; ††P < 0.01; †††P < 0.001 according to clinical factors within each polysomnographic study by Mann-Whitney U tests.
Changes in sleep state perception depending on the categories of sleep state perception
Using the cutoff values of ± 60 minutes of sleep state misperception, the diagnostic study showed that 26.5% (n = 90) and 13.3% (n = 45) of patients underestimated and overestimated their sleep duration, respectively. Normal perception of TST within 60 minutes was observed in 60.2% (n = 204) of patients. Patients with an underestimated misperception had less underestimation of sleep during CPAP titration (P < 0.001), whereas those with an overestimated misperception had less overestimation of sleep during CPAP titration (P < 0.001) (Table 4). These perceptual improvements were observed regardless of the presence or absence of clinical factors (Supplementary Table 1). Patients with a normal perception significantly underestimated their sleep duration during CPAP titration (P < 0.001); however, the amplitude of the changes was significantly lower than that in patients with either underestimated or overestimated misperception (P < 0.001).
Table 4
Comparisons of sleep perception between diagnostic and CPAP titration PSG according to sleep perception types (N = 339)

Data are presented as median and interquartile range.
CPAP = continuous positive airway pressure, PSG = polysomnography, TST = total sleep time.
aDefined as a difference of ± 60 minutes between subjective and objective total sleep times.
***P < 0.001 between diagnostic and CPAP titration studies by Wilcoxon signed-rank tests.
Of 90 patients with sleep underestimation, 40 (44.4%) and 8 (8.9%) had normal perception and overestimation of sleep during CPAP titration, respectively (Table 5). Of 45 patients with sleep overestimation, 34 (75.6%) and 6 (13.3%) had normal perception and underestimation of sleep during CPAP titration, respectively. Of 204 patients with normal sleep perception, 138 (67.6%) and 10 (4.9%) had underestimation and overestimation of sleep during CPAP titration, respectively.
Table 5
Comparisons of sleep perception types between diagnostic and CPAP titration polysomnography (N = 339)

DISCUSSION
Using the cutoff value of ± 60 minutes of sleep state misperception, we found that underestimated and overestimated sleep state misperceptions were present in 26.5% and 13.3% of patients with moderate-to-severe OSA, respectively. Patients with either underestimated or overestimated sleep state misperception during diagnostic PSG showed significant perceptual improvements during CPAP titration. Specifically, 44.4% of patients with sleep underestimation and 75.6% of those with sleep overestimation showed a normal perception of sleep during CPAP titration. These findings are consistent with those of Castillo et al.9 using the same criteria for sleep perception as those in the present study, in which OSA patients with > 60 minutes misperception in a diagnostic study showed significantly improved perception accuracy during CPAP titration studies regardless of the types of underestimated or overestimated misperception. These findings suggested that CPAP therapy is also effective in improving insomnia in patients with OSA, particularly those with sleep state misperception. In contrast, in the present study, patients who reported normal sleep perception significantly underestimated their sleep during CPAP titration. Specifically, of 204 patients with normal sleep perception during a diagnostic study, two-thirds of them had an underestimation of sleep during the CPAP titration study. This finding is inconsistent with those of Castillo et al.,9 in which no differences in sleep perception were observed between the diagnostic and CPAP titration studies in patients with normal sleep perception during a diagnostic study. The reasons for this discrepancy were unclear, but it could be explained in part by the differences in study sample characteristics. Compared to Castillo et al.,9 our study sample was less comorbid with insomnia symptoms (41.3% vs. 76.5%) and much more severe in OSA severity (median AHI, 35/h vs. 13/h). A recent study showed that patients with severe OSA were more likely to overestimate their sleep duration, while those with insomnia symptoms comorbid with OSA were more likely to underestimate sleep.10 These differences in study sample characteristics would have contributed to differences in the degree of sleep misperception during the diagnostic study (subjective minus objective sleep duration, median −8.0 minutes in our study vs. −34 minutes in Castillo et al.9) and differences in the changes in sleep perception during CPAP titration. In addition, significant improvements in sleep architecture during CPAP titration were observed in the present study, but not by Castillo et al.9
Little is known regarding the mechanisms underlying sleep state misperception and its improvement during CPAP titration in patients with OSA. In general, insomnia is a significant factor related to sleep underestimation.124 This also appears to be true for patients with OSA as studies have reported underestimated sleep duration in patients with both OSA and insomnia.891025 The compelling hypothesis regarding underestimated sleep duration is that it is related to the fragmentation of sleep architecture, consequently linking to increased light sleep stage or high frequencies of awakenings.91416 Based on this hypothesis, the observation of CPAP titration leading to significant improvements in sleep architecture in the present study might result in improved sleep perception in patients with OSA with underestimated misperception.
A small proportion of patients with OSA showed a significant overestimation of their sleep duration.81025 A recent study identified OSA severity as a significant factor associated with sleep overestimation.10 That is, patients with severe OSA were more likely to overestimate their sleep duration than those with milder OSA. The underlying mechanisms for this observation are largely unknown; however, the relative impairment of cognitive functioning in patients with severe OSA might contribute to their sleep overestimation.12 Spectral analyses of waking EEG, an index of cerebral functioning, showed EEG slowing across all scalp regions in patients with OSA.1426 This slowing was associated with increased omissions and reaction times during a cognitive task,26 which could be related to sleep overestimation in patients with OSA. Thus, the amelioration of sleep apnea during CPAP titration and the consequent improvement in cognitive functioning might cause improved sleep perception in OSA patients with overestimated misperception.
In the present study, patients with normal sleep perception significantly underestimated their sleep by about half an hour during CPAP titration. It is unclear which mechanisms are involved in the significant underestimation of sleep in patients with normal sleep perception during CPAP titration. One possible explanation is that discomfort with first-time CPAP application for titration such as an uncomfortable mask or air leaks around the edges of the mask could result in sleep disturbance and subsequent underestimation of sleep on the first night of CPAP. Such a potential adverse effect of CPAP on sleep perception is also expected in patients with sleep state misperception. In patients with overestimated misperception, this adverse effect of CPAP would be added to perceptual improvements during CPAP titration. In contrast, in patients with underestimated misperception, this effect of CPAP would lessen the amplitude of perceptual improvements during CPAP titration. It is not known how long the adverse effect of CPAP on sleep perception would last in CPAP machine users; however, it is expected that the adverse effect of CPAP on sleep perception will disappear when patients become accustomed to using a CPAP machine.
This study has some limitations. First, this was a retrospective study, in which confounding variables were difficult to control. Second, the assessments of sleep state perception in diagnostic and CPAP titration studies were performed using only a single overnight PSG. The data from single overnight studies may be vulnerable to the first night effect of PSG, which is characterized by longer sleep onset latency, lower sleep efficiency, longer REM latency, decreased REM, and increased alpha that may, consequently, affect sleep state perception,27 particularly in patients with OSA.28 Night-to-night variability in insomnia patterns can also reduce the reliability of single-night measurements.29 Future study needs to assess sleep perception after a period of compliant CPAP use. Finally, changes in health status between diagnostic and CPAP titration studies may be a potential confounding factor; however, most (90.6%) of the patients in this study underwent CPAP titration within 12 weeks after an initial diagnostic study.
In conclusion, CPAP titration may improve sleep perception in patients with moderate to severe OSA who have sleep state misperception, regardless of the types of underestimation or overestimation. However, CPAP titration may result in sleep misperception especially underestimation of sleep in those who have normal sleep perception. The underlying mechanisms for these observations remain to be elucidated. Our findings further our understanding of the pathophysiology of sleep state misperception in patients with OSA.
 XML Download
XML Download