

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The first interventional rigid bronchoscopy was performed in 1897 by Gustav Killian to remove a foreign body from the right main bronchus of a farmer.1 The rigid bronchoscope was widely used as the only diagnostic and therapeutic tool that allowed direct observation of the inside of the airway until Shigeto Ikeda introduced the flexible bronchoscope in the late 1960s. The use of the flexible bronchoscope increased because it is less invasive, does not require general anesthesia, and peripheral bronchi are easier to observe than with the rigid bronchoscope, which was regarded as obsolete and virtually abandoned.2 However, as Jean-François Dumon developed laser therapy in the early 1980s and silicone stent insertion in the late 1980s to treat central airway obstruction, he pioneered modern rigid bronchoscopy.234 Because rigid bronchoscopy has several advantages over flexible bronchoscopy, such as facilitating silicone stent insertion and mechanical debulking, better airway control, and greater capability for suction, it continues to occupy an important place in interventional pulmonology.1
In Korea, Professor Hojoong Kim in Samsung Medical Center (SMC) started rigid bronchoscopy in earnest in March 1999, and 1,300 cases of rigid bronchoscopy were performed on 600 patients by October 2006,5 compared with a recently reported paper on 1,301 patients over 12 years, the largest scale at a single institution.6 The number of procedures has been steadily increasing and several physicians have been trained at SMC since 2007; however, it seems that hospitals other than SMC are not actively implementing rigid bronchoscopy.7 Although all interventional pulmonologists think that rigid bronchoscopy is an irreplaceable technique in the field of interventional pulmonology, the reasons why rigid bronchoscopy is not widely used are probably because of the steep learning curve and the difficulties of consulting with an anesthesiologist due to lack of familiarity with ventilation and general anesthesia methods.89
According to the previous report in 2007, post-tuberculous tracheobronchial stenosis (PTBS) accounted for 56% of the indications for rigid bronchoscopy, followed by post-intubation or tracheostomy tracheal stenosis (PITS) for 23% and malignant tumors for 18%.5 As the prevalence of tuberculosis is decreasing and the survival rate of lung cancer has improved significantly in recent years in Korea,1011 the indications for the procedure may have changed significantly, but there have been no studies on this yet. In addition, the obstacles that impede the widespread use of rigid bronchoscopy in Korea are not known. Therefore, this multicenter retrospective study analyzed trends in indications for rigid bronchoscopy and characteristics of patients, and investigated the difficulties associated with the procedure and advice for junior operators through an online survey for rigid bronchoscopy operators.
METHODS
Patients
We (Jeong BH and Kim H) have contacted 16 hospitals known to be performing rigid bronchoscopy in the Republic of Korea. Fourteen hospitals where the operators were affiliated with the department of pulmonary medicine expressed a desire to participate in this study; however, there was no response from two hospitals where the procedure is being performed by the department of otorhinolaryngology and thoracic surgery. We retrospectively collected data on 2,860 patients who underwent rigid bronchoscopy between January 2003 and December 2020 at 14 hospitals (Fig. 1). This study was approved by the institutional review board of each hospital (Supplementary Data 1). Informed consent was waived at all hospitals because patient information was de-identified and anonymized before the analyses.
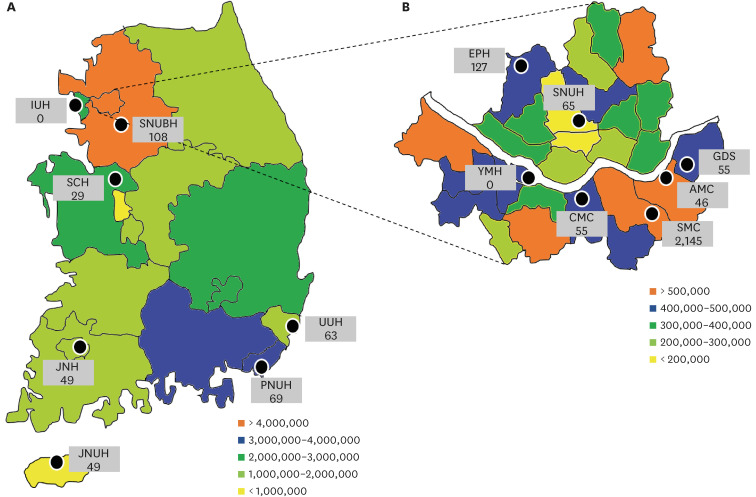
Fig. 1
Location of each hospital participating in this study. The number of populations in each region is indicated by color, and the number of patients included during the study period in each hospital is indicated by a number. Two hospitals (IUH and YMH) were unable to perform rigid bronchoscopy due to administrative problems and non-cooperation with other departments during the study period. The full name of each hospital is in the footnote of Supplementary Table 1. (A) The 17 administrative districts of the Republic of Korea. (B) The 25 administrative districts of Seoul are presented separately.
Data collection
We retrospectively collected the following data related to patient characteristics at the time of the first procedure only: age, sex, date of the procedure, indications for rigid bronchoscopy, respiratory support before the procedure (mechanical ventilation and extracorporeal membrane oxygenation, ECMO), treated sites of the airway, and severity of stenosis. Indications for rigid bronchoscopy were classified as follows: 1) malignancy, cases for symptom relief of airway stenosis caused by malignant tumors, definitive treatment for malignant tumors confined to airways, or diagnostic purpose of malignant tumors; 2) PTBS, airway stenosis caused by sequelae of endobronchial tuberculosis in patients with a history of pulmonary tuberculosis or active tuberculosis; 3) PITS, caused by sequelae of endotracheal intubation or tracheostomy; 4) benign tumor, definitive treatment for endobronchial benign tumors confined to airways, or diagnostic purpose of benign tumors; 5) foreign body, for the purpose of removing foreign bodies in the airways; 6) post-operative tracheobronchial stenosis, airway stenosis after the surgery such as sleeve lobectomy, tracheal resection and anastomosis, lung transplantation, etc.; 7) fistula, airway fistula with esophagus or other mediastinal structures; 8) radiation bronchitis and stenosis, airway stenosis caused by thoracic radiation therapy; and 9) other, airway stenosis other than the causes mentioned above. If there were two or more indications at the same time, only one indication was recorded that more contributed to the need for intervention. We also retrospectively collected data on the follow-up period and the total number of procedures performed up to December 2020 for each patient.
Since the patients could have been treated at multiple sites at the same time, the treated sites were categorized as follows to simplify the classification: when the main bronchus or bronchus intermedius were treated with its subdivisions at the same time, only the main bronchus or bronchus intermedius were mentioned; in the same way, when the lobar bronchus was treated with its subdivisions, only the lobar bronchus was mentioned. We evaluated the severity of airway stenosis using the Myer-Cotton stenosis grading system after excluding patients with lesions limited to lobar bronchi and their subdivisions: grade I, ≤ 50% luminal stenosis; grade II, 51–70% luminal stenosis; grade III, 71–99% luminal stenosis; and grade IV, no lumen.12
Online survey
We (Jeong BH and Kim H) sent an online survey to operators in 14 hospitals to find out the difficulties in starting and maintaining the procedure and to give advice to juniors who would like to learn the procedure. Among 23 operators from a total of 14 hospitals participating in this study, 14 operators responded to this online survey after excluding 9 (operators who no longer intend to participate in the procedure, n = 6; curators of this study, n = 2; and an operator who left the hospital during the study, n = 1; Supplementary Table 1). The detailed questionnaire is shown in the Supplementary Data 1.
Statistical analysis
Data are presented as the number (%) for categorical variables and median (interquartile range, IQR) for continuous variables. The study period of 18 years was divided into 6 sections of 3 years each, and the Jonckheere–Terpstra test for continuous variables and the Mantel–Haenszel test for categorical variables were used to analyze trends of indications for rigid bronchoscopy and disease severity. Since the number of patients and experiences of the procedure differed greatly between SMC and other hospitals, the data were analyzed by dividing the institutes into SMC and others. Categorical variables were compared using the Pearson χ2 test or Fisher’s exact test. Continuous variables were compared using the Mann–Whitney U test because they did not have a normal distribution. However, since it was not easy to compare some continuous variables with nonparametric methods, the mean (± standard deviation) was presented and Student’s t-test was used.
Based on the survey results, the correlation between operator characteristics and survey responses was analyzed using the Spearman method. Through this analysis, we investigated what the biggest problems of the operators with a small number of procedures are, and what they want to emphasize to their juniors. The Spearman correlation coefficient value (r
s) was considered to show moderate, strong, and very strong relationships at 0.40–0.59, 0.60–0.79, and 0.80–1.0, respectively.
All tests were two-sided, and a P value < 0.05 was considered significant. All statistical analyses were performed using SPSS software (IBM SPSS Statistics ver. 27; IBM Corp., Chicago, IL, USA).
Ethics statement
This study was approved by the Institutional Review Board of each hospital (Supplementary Data 1). Informed consent was waived at all hospitals because patient information was de-identified and anonymized before the analyses.
RESULTS
Two of 14 hospitals were unable to perform rigid bronchoscopy due to administrative challenges and lack of cooperation with other departments (Supplementary Table 1). Excluding these two hospitals, the number of new patients treated over 18 years was 2,145 in SMC and a median of 55 (range, 29–127) in other hospitals. By operator, two operators from SMC performed the procedure on 1,597 and 521 patients, respectively, and 13 operators who are still active in other hospitals performed the procedure on a median of 46 (range, 8–128) patients.
Trends on the indications for rigid bronchoscopy
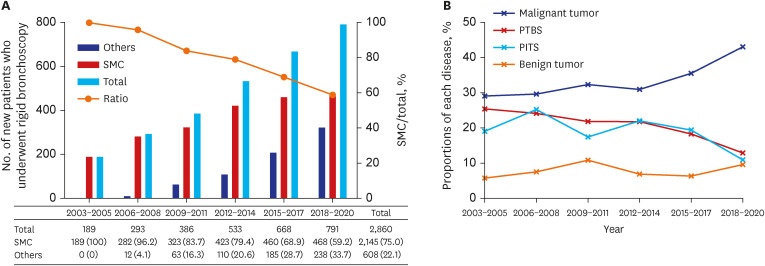
Trends in the number of new patients undergoing rigid bronchoscopy and the indications for the rigid bronchoscopy are shown in Fig. 2 and Supplementary Tables 1 and 2. The number of new patients at SMC increased from 189 in 2003–2005 to 468 in 2018–2020, and that of other institutions increased from 0 in 2003–2005 to 238 in 2018–2020. Eventually, the proportion of SMC in the total number of patients started from 100% and steadily decreased to 59.2% (Fig. 2A). The proportion of malignancy as the indication for the procedure steadily increased from 29.1% (2003–2005) to 43.0% (2018–2020) in the total hospitals (P for trend < 0.001), whereas those of PTBS and PITS steadily decreased from 25.4% and 19.0% to 12.9% and 10.9% of the total, respectively (P for trends < 0.001) (Fig. 2B). Even when dividing the total number of institutions into SMC and others, similar trends of increasing the proportion of malignancy and decreasing the proportion of benign diseases were shown over time.
Fig. 2
Trends in the number of new patients and the indications for rigid bronchoscopy. (A) The trend in the number of new patients undergoing rigid bronchoscopy over time. Black and gray bars represent the numbers of new patients treated at SMC and hospitals other than SMC, respectively. Checkered bars indicate the total number of new patients who underwent the rigid bronchoscopy. A line graph shows the ratio of the number of patients at SMC to the total number of patients. See Supplementary Table 1 for detailed figures. (B) The trend in the indications for the rigid bronchoscopy. Red, purple, green, and gray lines represent malignant diseases, PTBS, PITS, and benign tumors, respectively. See Supplementary Table 2 for detailed figures.
SMC = Samsung Medical Center, PTBS = post-tuberculosis tracheobronchial stenosis, PITS = post-intubation or tracheostomy tracheal stenosis.
Comparisons of patient characteristics between SMC and other hospitals
Baseline characteristics of patients were compared between SMC (n = 2,145) and others (n = 715) in Table 1. Patients in the SMC group were younger (median 59 vs. 61 years, P < 0.001), and fewer were male (53.2% vs. 62.8%, P < 0.001) than in the other group. In all patients, malignancy (35.3%) was the most common indication for the procedure, followed by PTBS (19.0%), PITS (17.8%), and benign tumor (8.0%). In the SMC group, the proportion of malignancy was lower (32.7% vs. 43.1%, P < 0.001) and the proportion of PTBS was higher (21.5% vs. 11.5%, P < 0.001) than in the other group. As other indications, endobronchial valve insertion for emphysema or persistent air leakage (38/39, 97.4%) and broncholith removal (36/37, 97.3%) were mostly performed in SMC, whereas all the cases of transbronchial lung cryobiopsy were performed in other institutions (35/35, 100%). When looking at the indications of 11 other hospitals (Supplementary Table 3), the proportions of each indication varied widely from hospital to hospital (23.2% to 72.4% for malignancy, 3.4% to 22.0% for PTBS, and 1.5% to 33.3% for PITS). In all hospitals, 9.1% of patients had respiratory failure before the procedure, 10.1% received treatment at multiple sites in the airway, and 66.0% had stenosis of grade III or more. In SMC, patients were followed for a longer period of time (median 10.6 vs. 8.0 months, P = 0.027) and received a higher number of procedures (mean 2.3 vs. 1.6, P < 0.001) than at the other institutions.
Table 1
Comparison of patient characteristics between SMC and other hospitals
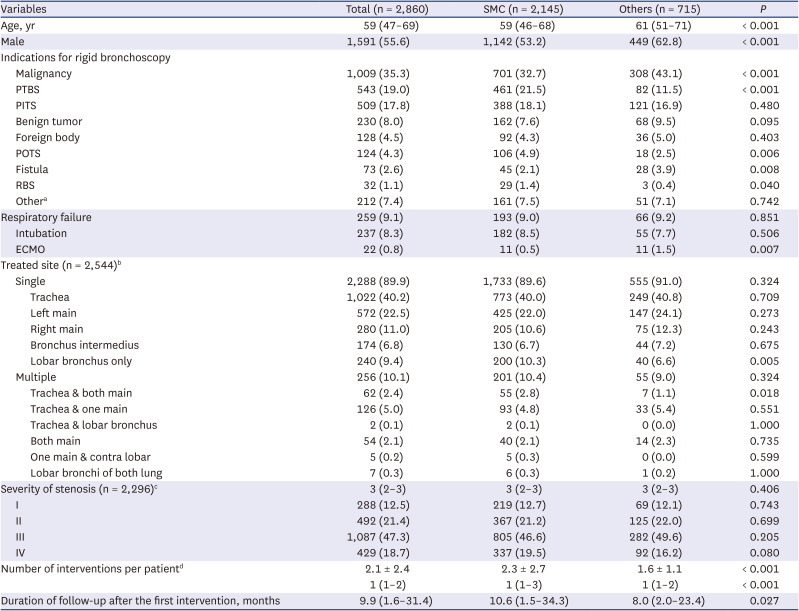
Data are presented as median (interquartile range), mean ± standard deviation, or number (%) values.
SMC = Samsung Medical Center, PTBS = post-tuberculosis tracheobronchial stenosis, PITS = post-intubation or tracheostomy tracheal stenosis, POTS = post-operative tracheobronchial stenosis, RBS = radiation bronchitis and stenosis, ECMO = extracorporeal membrane oxygenation.
aEndobronchial valve insertion for emphysema or persistent air leakage (n = 39; SMC = 38), broncholith (n = 37; SMC = 36), transbronchial lung cryobiopsy (n = 35; SMC = 0), idiopathic tracheal or bronchial stenosis (n = 17; SMC = 15), organizing blood clots (n = 16; SMC = 12), relapsing polychondritis (n = 13; SMC = 12), traumatic bronchial stenosis such as traffic or crushing accidents (n = 12; SMC = 10), post-infectious stenosis other than tuberculosis (n = 10; SMC = 6), and others (n = 33; SMC = 32).
bExcluding patients who underwent procedures for airway foreign body (n = 128) and fistula (n = 73). Among patients who underwent procedures for other indications, 108 patients without airway stenosis were also excluded. There were 7 patients with missing data on this variable.
cMyer and Cotton grade was used: grade I, ≤ 50% luminal stenosis; grade II, 51–70% luminal stenosis; grade III, 71–99% luminal stenosis; and grade IV, no lumen. Among 2,544 patients who were evaluated for the ‘treated site,’ 247 patients with lesions limited to lobar bronchi and one patient with missing values were excluded.
dSince this variable does not have a normal distribution, it should be expressed as the median (interquartile range) and a nonparametric test should be performed. However, it is not easy to compare quantities if only the median value is indicated, so the average value is also described.
For the four indications where the procedure was most commonly applied (malignancy, PTBS, PITS, and benign tumor), the patient’s baseline characteristics were also compared by dividing them into SMC and other institutions (Supplementary Tables 4, 5, 6, and 7).
Trends in disease severity
Among the baseline characteristics, trends were analyzed for three variables related to disease severity (Table 2). In all the hospitals, patients with respiratory failure before the procedure steadily increased from 4.2% to 10.5% (P for trend < 0.001) and patients with multiple stenosis also increased from 8.3% to 14.9% (P for trend < 0.001). There were no statistically significant trends in stenosis severity. However, when divided into two groups, patients with grade I stenosis steadily increased from 4.8% to 13.1% (P for trend = 0.002) in the SMC group and stenosis grades were slightly increased from 2.6 ± 1.1 to 2.8 ± 0.9 (P for trend = 0.014) in the other group. A subgroup analysis of patients with malignancy also showed a tendency that frequencies of preoperative respiratory failure and multiple stenosis increased over time (Supplementary Table 8).
Table 2
Trends in disease severity over time
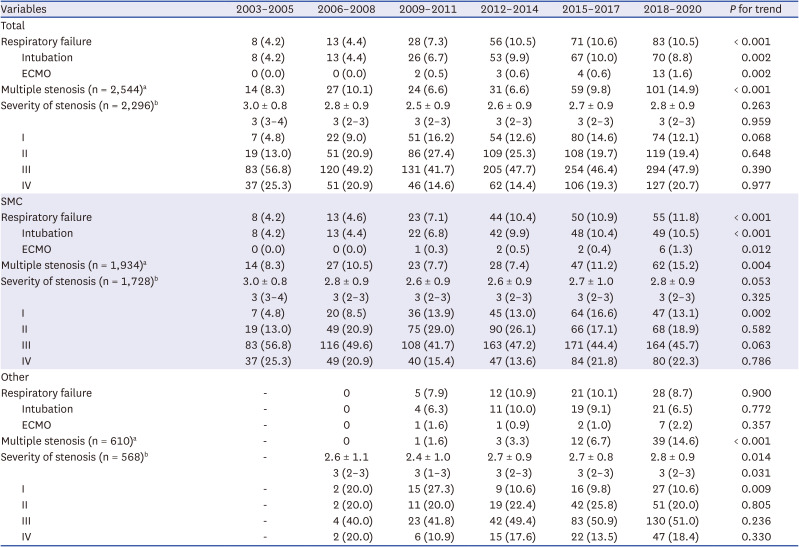
Data are presented as median (interquartile range), mean ± standard deviation, or number (%) values.
ECMO = extracorporeal membrane oxygenation, SMC = Samsung Medical Center.
aExcluding patients who underwent procedures for airway foreign body and fistula. Among patients who underwent procedures for other indications, patients without airway stenosis were excluded. Some patients with missing values were also excluded.
bMyer and Cotton grade was used: grade I, ≤ 50% luminal stenosis; grade II, 51–70% luminal stenosis; grade III, 71–99% luminal stenosis; and grade IV, no lumen. Among patients who were evaluated for ‘treated site,’ patients with lesions limited to lobar bronchi were excluded. Since this variable does not have a normal distribution, it should be expressed as the median (interquartile range) and a nonparametric test should be performed. However, it is not easy to compare quantities if only the median value is indicated, so the average value is also described.
Online survey responses
The median age of 14 online survey respondents was 47.5 (IQR, 42.5–52) years old, and 13 (92.9%) were male (Table 3). They observed rigid bronchoscopy for the first time at a median of 3.5 (IQR, 1–8.5) years after acquiring their specialist license for respiratory medicine, and performed the first procedure without a supervisor a median of 1 (IQR, 0–2) year after their first observation. The hospital where they observed their first procedure was typically SMC (11/14, 78.6%). At the time of the survey (April to May 2021), their experience as a specialist in respiratory medicine was a median of 14 (10.8–18) years. The median number of total procedures reported by each operator was 60 (IQR, 28–98). However, half of them said they were performing less than one case per month over the past year. In particular, only three operators reported that the number of cases was steadily increasing.
Table 3
Characteristics of survey subjects and the results of the responses to the questionnaire
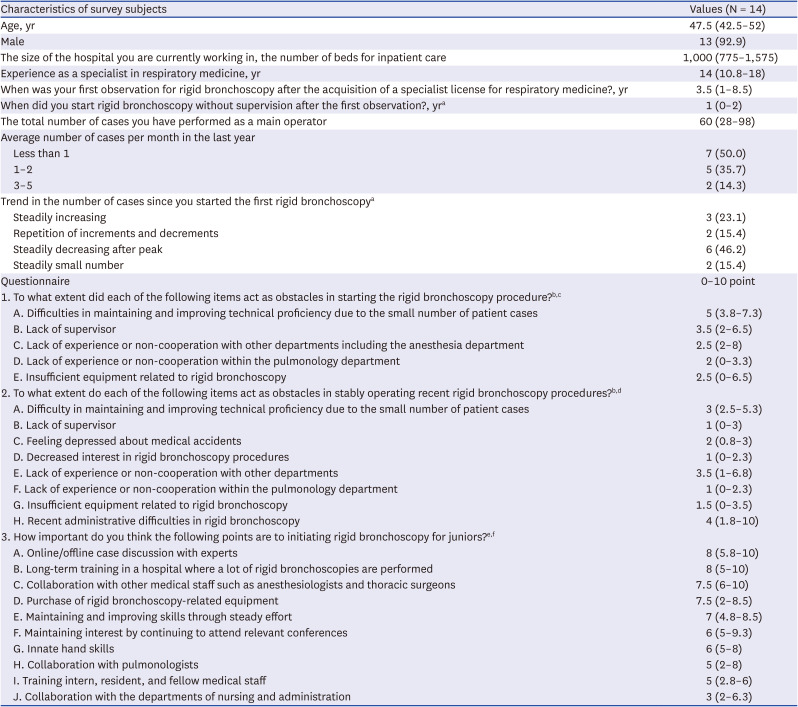
Data are presented as median (interquartile range) or number (%) values.
aExcluding one operator who could not start the procedure due to administrative difficulties.
bSurvey subjects gave each question a score from 0 to 10. A score of 0 means ‘no problem at all’ and a score of 10 means ‘enough to give up’.
cOther comments: nighttime procedures after regular working hours (8 points), the work takes a lot of time to prepare due to various problems and interferes with other work (8 points), death or serious complications during the procedure (8 points), lack of manpower to help before and after the procedure (7 points), lack of resident to help (6 points), absence of alternative operators in case of emergency (6 points).
dOther comments: the work takes a lot of time to prepare due to various problems and interferes with other work (10 points), administrative improvement was made because anesthesia was given in the bronchoscopy room (not pointed).
eSurvey subjects gave each question a score from 0 to 10. A score of 0 means ‘not at all’ and a score of 10 means ‘very important’.
fOther comments: intensive short-term training of about 3 months (7 points), understanding of the procedure, and motivation to learn (5 points).
When respondents first started the procedure as a main operator, they stated that the most difficult thing was improving their skills due to the small number of cases (median 5 points), followed by anxiety over a lack of supervision (median 3.5 points) and lack of experience or lack of cooperation with other departments (median 2.5 points). In performing the current procedure, they said that the biggest obstacle was administrative difficulties (median 4 points), followed by lack of experience or lack of cooperation with other departments (median 3.5 points) and feeling depressed by medical accidents (median 2 points). They indicated that discussion with experts (median 8 points), long-term training (median 8 points), and collaboration with other medical staff (median 7.5 points) are important for junior operators who are interested in this procedure.
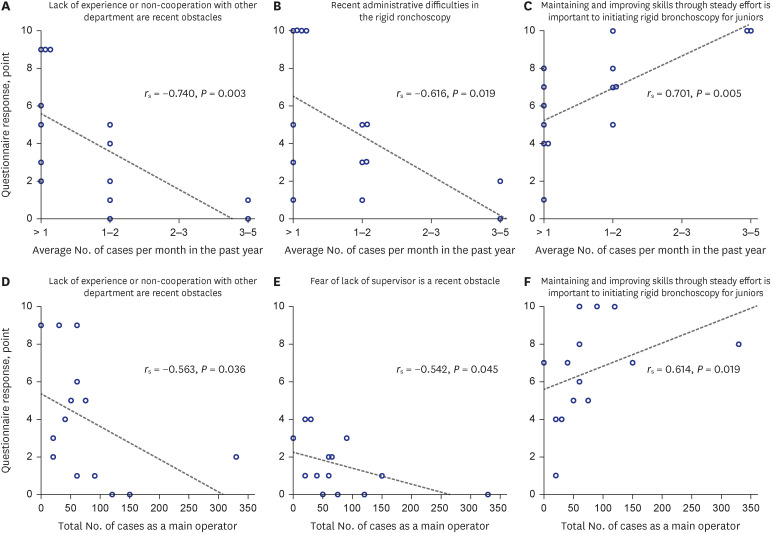
Fig. 3 shows the relationship between the number of procedures performed and the response of the operators. The fewer the number of cases performed within the last year, the more likely they were to respond that collaboration with other departments are recent obstacles (rs = −0.740, P = 0.003) and recent administrative difficulties were encountered (rs = −0.616, P = 0.019). The fewer the total number of cases as a main operator, the more likely they were to respond that collaboration with other departments (rs = −0.563, P = 0.036) and anxiety over a lack of supervisor are recent obstacles (rs = −0.542, P = 0.045). However, the greater the number of cases performed within the last year (rs = 0.701, P = 0.005) or the total number of cases as a main operator (rs = 0.614, P = 0.019), the more likely they were to indicate that steady effort is important for juniors.
Fig. 3
Correlation between respondent characteristics and survey responses. The degree of correlation was expressed as a Spearman correlation coefficient value (r s). Generally, 0.40–0.59 is interpreted as ‘moderate’, 0.60–0.79 as ‘strong’, and 0.80–1.0 as ‘very strong’ relationships. Refer to Table 3 and Supplementary Data 1 for detailed survey content and the meaning of the survey responses of 0 to 10 points.
DISCUSSION
Rigid bronchoscopy began to be re-examined as a therapeutic option with advances in laser treatment and silicone stent insertion in the 1980s and 1990s,34 but according to a survey by the American College of Chest Physicians in 1991, only 8.4% of responders indicated that they used the rigid bronchoscope in their practice,13 and even this decreased to 4.5% in 1999.14 In Korea when Professor Hojoong Kim began to actively perform rigid bronchoscopy in 1999, this procedure was mostly forgotten. However, recently, the number of patients at SMC has been steadily increasing and the proportion at other hospitals is also constantly increasing. In addition, the increase in the proportion of severe cases with respiratory failure or multiple stenosis can be interpreted as an improvement in the skill of the operators for the procedure. We think it is direct evidence that the number of physicians proficient with rigid bronchoscopy as an effective treatment method has increased, and also it is indirect evidence that the number of physicians who can present rigid bronchoscopy as another treatment option to their patients has increased.
The procedure may vary depending on the indications for rigid bronchoscopy. For example, the operator will mainly remove the tumor in patients with malignancy, widen the fibrotic stenosis in patients with benign disease, and focus on the management of long-term complications when a stent is inserted. Therefore, it will be important to prepare for the future to understand the change in the trend of the patient group that requires rigid bronchoscopy. In this study, the proportion of malignancy was steadily increasing, whereas those of benign diseases such as PITS and PTBS were steadily decreasing. Central airway obstruction can occur in more than 20% of all patients as the first diagnosis of cancer or cancer progression during treatment, not only in primary lung cancer but also in pulmonary metastasis of extrapulmonary malignancies.151617 According to the annual report of cancer statistics in Korea in 2016, the 5-year observed survival rates of patients with lung cancer have risen from 14.5% (2001–2005) to 25.3% (2012–2016) in just 10 years.11 As the cancer survival rate increases, it can be expected that the frequency of central airway obstructions requiring rigid bronchoscopy treatment will also increase. Meanwhile, even though the new tuberculosis cases per 100,000 population has halved in the past decade from 78.9 in 2011 to 35.7 in 2021,10 PTBS was the main cause of benign airway stenosis in Korea because the incidence rate was still higher than that of developed countries. In this study, although the proportion of new patients with PTBS was steadily decreasing from 25.4% during 2003–2005 to 12.9% during 2018–2020, the number increased from 48 to 102 (Supplementary Table 2). Considering that only 20–40% of PTBS patients needed bronchoscopic intervention in the active state and the remaining 60–80% received the procedure a median 3–5 years after the end of anti-tuberculosis treatment,181920 the number of PTBS patients is not expected to decrease significantly for the foreseeable future in Korea. PITS is an important cause of benign airway stenosis. Although bronchoscopic intervention is considered as a bridge therapy to surgery or as definitive treatment in cases with contraindications to surgery,221 the number of patients has decreased in this study. This probably reflects improved care in the intensive care unit, such as reduced traumatic intubation, use of low-pressure and high-volume cuffed tubes, and increased rates of early tracheostomy.2223
Even though the demand for rigid bronchoscopy is increasing, only 3 out of 14 operators answered that the number of procedures was steadily increasing in the online survey. The biggest problem in the procedure they pointed out was the difficulty in improving and maintaining skills due to the small number of patients. In addition, operators with fewer procedures tended to complain of difficulties in collaboration with other departments and administrative problems. In particular, we discovered that the operators with a small number of procedures had difficulty persuading the anesthesiologist because of unfamiliarity with the method of general anesthesia for this procedure and repulsion of sharing the airway with the operators during the procedure. The unfamiliarity of the administrative process for internists using the operating room was also identified as a barrier in this procedure. Lastly, respondents requested active discussions with experts, training in specialized hospitals, and collaboration with other departments to guide junior operators in the use of rigid bronchoscopy. They may have felt that it is important to learn the procedure systematically and that collaboration with other departments is important when performing procedures on patients at the hospital where you work.
There are several limitations to this study. First, this study did not include all cases in Korea. In particular, 2 of the 16 hospitals we contacted did not respond. Although it is not possible to determine the exact number of patients who underwent this procedure during the study period, it is likely that more than 90% of all cases in Korea have been included, so we think that the domestic situation is well represented. Second, the procedure details and clinical outcomes were not investigated. So, we could not evaluation the relationship between proficiency and clinical outcomes. It was encouraging to know that rigid bronchoscopy is being used more and more widely in Korea through this study, but the fact that half of the operators performed less than one procedure in the last month left concerns about maintaining the skill level. And, according to reports on treatment results and complications of bronchoscopic intervention for malignant central airway obstruction in 15 US centers with 26 physicians,2425 procedure details and the clinical outcomes vary from hospital to hospital. Because the equipment available at each hospital and the preferred technique of each operator vary, further studies will be needed to analyze the clinical outcomes of each situation and to explore procedure standardization.
We analyzed the past and present status of rigid bronchoscopy in Korea through this paper. This study demonstrated that the number of patients undergoing this procedure has been increasing, especially for cancer treatment, and more and more pulmonologists are interested in this procedure. Unfortunately, however, most of the operators were unable to perform this procedure actively and they complained of difficulties beyond the procedure itself, such as collaboration with other departments. Therefore, for this procedure to be used more widely, it will be important for beginners to learn systematically about the procedure itself as well as to achieve a multidisciplinary consultation through collaboration with other departments.
 XML Download
XML Download