

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Community-acquired pneumonia (CAP) is a leading cause of infectious deaths worldwide. Approximately 10% of patients hospitalized with CAP require admission to the intensive care unit (ICU) with a rate of mortality ranging from 11% to 56%.1 According to Statistics Korea, pneumonia is the third most common cause of death and the most common infection-related cause of death in Korea.2 The death rate is particularly high among elderly patients. Accordingly, both the number of patients hospitalized for pneumonia and the cost of medical expenses are rising each year in Korea because of the increasing aging population.34
For several decades, antibiotics have been the cornerstone for CAP management. The timely administration of appropriate antibiotics is associated with better outcomes, including a reduction in the rate of mortality.5 The type of antibiotics used to treat CAP mainly depends on empirical therapies because of the difficulty associated with isolating the causative pathogens. Therefore, guidelines for empirical therapies have influenced the selection of antibiotics for CAP.67 In recent published guidelines of the American Thoracic Society and Infectious Diseases Society of America (IDSA) and National Institute for Health and Care Excellence (NICE), three antibiotic classes (fluoroquinolones, beta-lactams, and macrolides) are recommended.89 The 2009 Korean guideline on CAP recommended the administration of respiratory fluoroquinolone alone or beta-lactam plus macrolide combination as empirical treatment for all patients hospitalized in general ward.10 The revised Korean guideline published in 2017 recommended a respiratory fluoroquinolone or a beta-lactam alone for patients with mild to moderate pneumonia admitted to a general ward, and a beta-lactam plus macrolide combination therapy for only suspected atypical pneumonia or severe pneumonia, under limited circumstances.7 There has been controversy over whether macrolide combination therapy is more effective in reducing mortality than beta-lactam monotherapy1112 and antibiotic treatment regimen for mild-to-moderate CAP has never been evaluated for Korean patients. Furthermore, it has never been evaluated whether the effectiveness of empirical antibiotic regimens change with the seasons worldwide. In Korea, from October 1, 2014 to December 31, 2017, National Quality Assessment Program (NQAP) for CAP management was implemented nationwide three times by Health Insurance Review and Assessment Service (HIRA). The first and third period (from October 1 to December 31) were conducted in autumn season, while the second period was conducted in spring (from April 1 to June 30). This allowed us to evaluate seasonal differences in the effectiveness of empirical antibiotics for CAP.
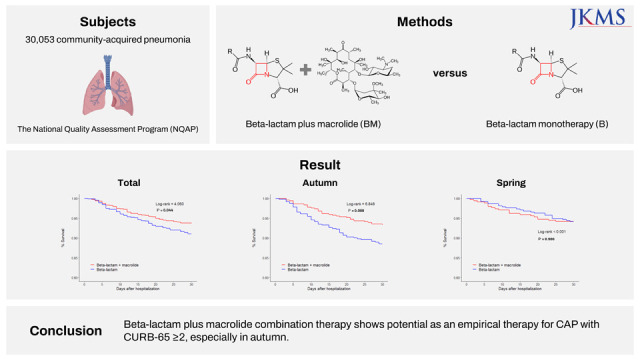
To address all of the points mentioned above, we investigated the effectiveness of beta-lactam plus macrolide combination therapy in CAP on a nationwide population-based cohort study. The 30-day survival rate between beta-lactam monotherapy plus macrolide combination (BM) group and beta-lactam monotherapy (B) group was evaluated for hospitalized patients with CAP using a National Health Insurance (NHI) database enrolled in NQAP for CAP management provided by HIRA in Korea. The differences between autumn and spring season were also evaluated in the subgroup analysis.
METHODS
Data source and management
The HIRA provides access to the Korean NHI claim database for a limited period for pre-specified individuals.13 NHI claim data contain demographic information, diagnosis codes based on the International Classification of Diseases-10th Revision (ICD-10), procedure codes, claim dates, cost of drugs/procedures/visits, and pharmacy claim records.14
The NQAP is a systematic method for the assessment of the clinical validity and cost efficiency of medical and pharmaceutical services, including diagnosis, treatment, and drugs, covered by healthcare benefits. Its purpose is to minimize the variance of treatment between medical institutions and physicians, and to improve the quality of the healthcare services provided.15
The NQAP for CAP management has been conducted since 2014, with the first evaluation period from October 1, 2014 to December 31, 2014, the second evaluation period from April 1, 2016 to June 30, 2016, and the third evaluation period from October 1, 2017 to December 31, 2017. The NQAP for CAP management excludes patients with hospital-acquired pneumonia, ventilator-associated pneumonia, healthcare-associated pneumonia, hospitalization history for more than 2 days within 90 days, immunocompromised, hospice palliative care, administration of oral antibiotics before hospitalization, delayed administration of intravenous antibiotic treatment for pneumonia more than 72 hours after hospitalization, or administration of total intravenous antibiotic treatment duration for less than 72 hours. The survey form of the NQAP for CAP management includes medical records for sex, age, place of visit, admission route, admission place, smoking history, pneumococcal vaccination history (≥ 65 years old), and confusion, urea, respiratory rate, blood pressure at age of 65 years or older (CURB-65) score. We participated in the NQAP research project and analyzed the effect of macrolide combination therapy for CAP treatment using NHI and quality assessment data.
Study methods
We conducted a retrospective cohort study with the patients selected from three evaluation periods of the NQAP for CAP management, and the National Health Insurance data on the selected patients was extracted from 1 year before the first patient enrollment and 1 year after the last patient enrollment at each evaluation period for the analysis of risk adjustment and outcomes. This data selection period was set to identify underlying diseases and confirm mortality and readmission rates up to one year after discharge.
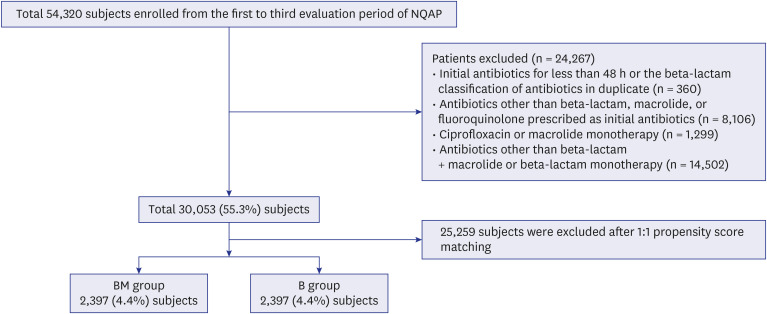
The CAP codes used in the present study are presented in Supplementary Table 1, and the initial empirical antibiotics used for this study are described in Supplementary Table 2. Individuals treated with anti-pneumococcal and anti-pneumococcal with anti-pseudomonal coverage beta-lactam antibiotics were assigned to the beta-lactam group, while those treated with azithromycin, clarithromycin, erythromycin, and roxithromycin were assigned to the macrolide group. Patients who received initial antibiotics during less than 48 hours after hospitalization, duplicated beta-lactam class antibiotics, or initial antibiotics other than beta-lactam and macrolide were excluded, as well as patients prescribed ciprofloxacin or macrolide monotherapy, to clarify the effectiveness and clinical outcomes between beta-lactam monotherapy and beta-lactam + macrolide combination therapy (Fig. 1).
The baseline characteristics, including age, sex, and CURB-65 score of the enrolled patients were measured at the time of hospitalization for CAP (index date). The CURB-65 score (presence of confusion, blood urea nitrogen > 19 mg/dL, respiratory rate ≥ 30/min, systolic blood pressure < 90 mmHg or diastolic blood pressure ≤ 60 mmHg, age ≥ 65 years) is a severity score used to determine the need for hospitalization in CAP.16 The Charlson comorbidity index (CCI) was used as a measure of a patient’s comorbidity in the year before the index date (pre-index period).17 The modification of antibiotic treatment, total duration of hospital stay, total cost of the antibiotics, total cost of hospitalization, rate of readmission within 30 days after hospital discharge, and rate of mortality (within 7, 14, or 30 days, 3 months, and 1 year) were assessed as clinical outcomes. The modification of antibiotic treatment included changes in the antibiotic administered or additional cases, as well as changes from a combination antibiotic treatment to monotherapy. The total cost of hospitalization included all expenses paid by health insurance, including cost per prescription, hospitalization charge, procedure charge, laboratory test charges, and radiologic examination charges. Non-reimbursed medical costs were not included. All costs are presented in US dollars (1 USD ≒ 1,150 KRW).
To evaluate the effectiveness of macrolide treatment against CAP, the treatment outcomes between beta-lactam monotherapy (B) and beta-lactam + macrolide (BM) groups as empirical antibiotics were compared. In addition, as the first and third evaluation period (from 1 October to 31 December) of NQAP for CAP management were conducted in autumn season, while the second study period was conducted in spring season (from 1 April to 30 June), we performed subgroup analysis for the enrolled patients from the autumn season (first and third study period) and spring season (second study period), respectively. This allowed us to evaluate any differences in the effects of macrolide combination treatment between the seasons of autumn and spring.
Statistical analysis
Descriptive statistics were used to characterize the cohort. Demographic and clinical outcomes were compared using Pearson’s χ2 test or Fisher’s exact test for categorical variables and using Student’s t-test or the Mann-Whitney U-test for continuous variables. Continuous variables are expressed as the mean ± standard deviation (SD) or median (interquartile range [IQR]) as appropriate; categorical variables are presented as frequencies (percentage, %).
The propensity scores were calculated using a multiple logistic regression model to establish patient’s probability of belonging to the beta-lactam monotherapy (B) group or beta-lactam + macrolide (BM) group according to covariates with age, sex, CURB-65 score, and CCI. The propensity scores were then used to match each therapy group 1:1 using greedy nearest-neighbor matching algorithm. The Kaplan-Meier analysis was used to estimate survival in the matched-pair cohort, and the log-rank test was used to analyze statistical significance. To analyze the seasonal impact, subgroup analysis was conducted. We repeated the primary analysis in subgroups using CURB-65 score (0–1 vs. ≥ 2). For each subgroup, we re-matched patients based on the CURB-65 score cut-off. All statistical analyses were performed in SAS Enterprise Guide version 6.1 (SAS Institute Inc., Cary, NC, USA). A P value of < 0.05 was considered statistically significant.
RESULTS
A total of 54,320 adult (≥ 18 years) hospitalized patients with ICD-10 codes for CAP (first: 15,432, second: 23,106, and third: 15,782) were included based on the NQAP for CAP management database. After excluding patients with initial antibiotics administration less than 48h or the beta-lactam classification of antibiotics in duplicate, antibiotics other than beta-lactam, macrolide, or fluoroquinolone prescribed as initial antibiotics, ciprofloxacin or macrolide monotherapy, or antibiotics other than beta-lactam + macrolide or beta-lactam monotherapy, a total of 30,053 patients were included for the comparative analysis between the BM and B groups (Fig. 1). The baseline characteristics and clinical outcomes between the BM and B groups before propensity score matching (PSM) are presented in Supplementary Table 3. After 1:1 PSM, 2,397 (4.4%) patients in each group were ultimately selected for further analysis (Fig. 1).
Baseline characteristics of study population
A comparison of the baseline characteristics of the patients in both groups is provided in Table 1. Among a total of 4,794 selected patients, the mean age was 65 ± 18, which was not significantly different between the groups (P = 0.788). The male-to-female ratio was 2,524 (52.7%) to 2,270 (47.4%), and was not significantly different between the groups (P = 0.954). The median CURB-65 score was 1 (IQR 0-2), and was also not significantly different between the groups (P = 0.945); the distribution of the CURB-65 scores also did not differ between the groups (P = 1.000). The distribution of CCI between the groups also did not differ (P = 0.903). More number of patients in the BM group were found to visit the hospital, especially the emergency room, compared with patients in the B group (P < 0.001). However, the number of patients admitted to the ICU was higher in the B group than in the BM group (P = 0.002). Glycopeptide antibiotic use was observed in 131 (2.7%) patients, with no significant difference in the number of patients administered glycopeptide antibiotics between the two groups (P = 0.658).
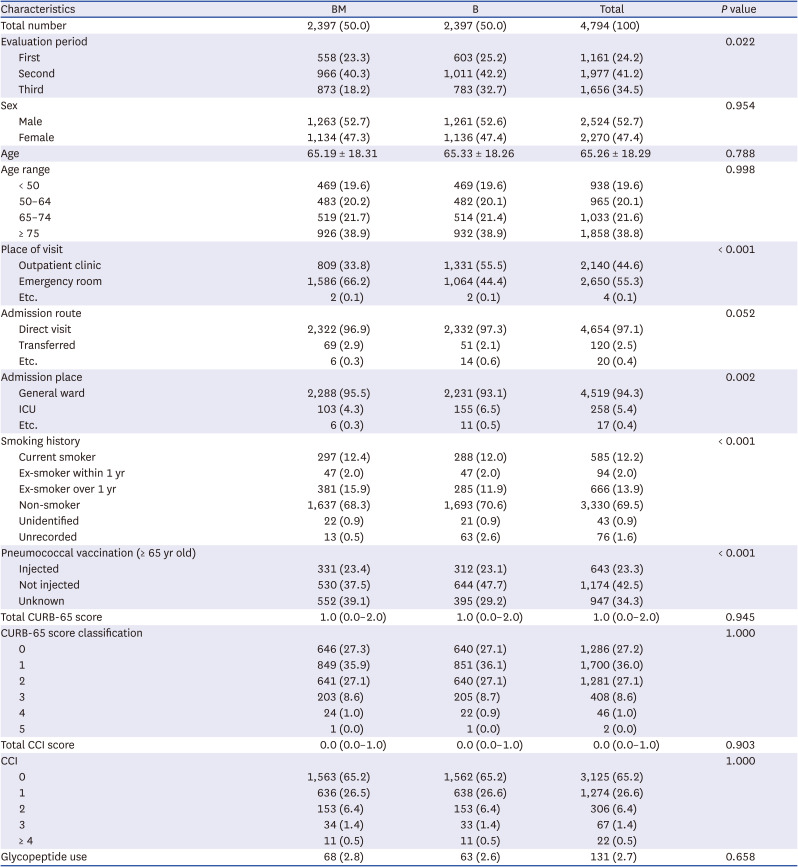
Table 1
Baseline characteristics of BM and B group after propensity score matching
Data are presented as number (%) or mean ± standard deviation or median (interquartile range).
BM = beta-lactam + macrolide combined therapy, B = beta-lactam monotherapy, ICU = intensive care unit, CURB-65 = confusion, urea, respiratory rate, blood pressure, age of 65 years or older, CCI =Charlson comorbidity index.
![]()
Clinical outcomes of the study population
The clinical outcomes of the BM and B groups after PSM are provided in Table 2. Antibiotic modification was observed in 3,970 (82.8%) patients, with a lower rate in the BM group than in the B group (93.4% vs. 72.4%, P < 0.001). The total length of hospital stay was found to be 10.16 ± 7.28 days, and was lower for the BM group than for the B group (9.49 ± 6.89 days vs. 10.83 ± 7.59 days) (P < 0.001). The total cost of antibiotics was also lower for the BM group than the B group (171.93 ± 186.51 USD vs. 188.93 ± 206.63 USD) (P = 0.003). However, the total cost of hospitalization was higher for the BM group than the B group (2,257.60 ± 2,279.15 USD vs. 2,096.16 ± 2,019.41 USD) (P = 0.010). Re-hospitalization within 30 days after initial discharge was observed in 669 (15.1%) patients, with no significant differences between the BM and B groups (332 [15%] vs. 337 [15.2%], P = 0.844).
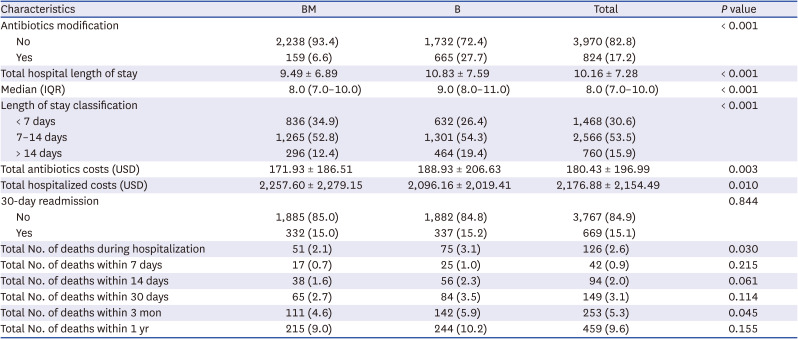
Table 2
Clinical outcomes of BM and B group after propensity score matching
Data are presented as number (%) or mean ± standard deviation or median (IQR).
BM = beta-lactam + macrolide combined therapy, B = beta-lactam monotherapy, IQR = interquartile range, USD = United States dollar.
![]()
Survival analyses after PSM
The 30-day survival rates did not differ significantly between patients in the BM and B groups (97.3% vs. 96.5%, log-rank = 3.049, P = 0.081) (Fig. 2A). In patients with scores of CURB-65 ≥ 2, the 30-day survival rate in the BM group was higher than that in the B group (93.7% vs. 91.0%, log-rank = 4.060, P = 0.044) (Fig. 2B). However, this was not observed in patients with scores of CURB-65 < 2 (99.2% vs. 99.3%, log-rank = 0.045, P = 0.833). Among patients with CURB-65 ≥ 2, the 30-day survival rate in the BM group was higher than that in the B group (93.3% vs. 88.5%, log-rank = 6.848, P = 0.009) during autumn season (Fig. 2C); notably, this pattern was not observed during spring (94.2% vs. 94.1%, log-rank < 0.001, P = 0.986) (Fig. 2D). Among patients with scores of CURB-65 < 2, no difference was observed in the 30-day survival rates between both groups in neither spring (99.2% vs. 99.2%, log-rank = 0.004, P = 0.948) nor autumn season (99.2% vs. 99.3%, log-rank = 0.053, P = 0.818). Furthermore, among all patients, no difference was observed in the 30-day survival rates between both groups in neither spring (97.4% vs. 96.5%, log-rank = 1.163, P = 0.281) nor autumn season (97.2% vs. 95.6%, log-rank = 1.926, P = 0.165).

Fig. 2
Kaplan-Meier plots showing differences in 30-day survival rate after hospitalization between the BM group (red) and B group (blue) after propensity score matching. (A) Whole patients. (B) In patients with CURB-65 ≥ 2. (C) In patients with CURB-65 ≥ 2 during autumn. (D) In patients with CURB-65 ≥ 2 during spring.
BM = beta-lactam + macrolide combined therapy, B = beta-lactam monotherapy, CURB-65 = confusion, urea, respiratory rate, blood pressure, age of 65 years or older.
![]()
DISCUSSION
Incidences of macrolide-resistant Mycoplasma pneumoniae (MRMP) have been documented for almost 20 years globally, presumably driven by antimicrobial pressure, most likely because of the widespread use of macrolides for the empirical treatment of CAP. The prevalence of MRMP in the United States ranged from 8.2% to 13.2% between 2006 and 2014.1819 The incidence of MRMP is high in Asia, with a prevalence from 90% to 100% in China, 60% to 90% in Japan between 2010 and 2014.20 According to a study from 2019, the prevalence of MRMP in South Korea increased continuously over 10 years, with a rate of 76.3% during 2014–2016.21 This increase in macrolide resistance to Mycoplasma strains has raised concerns regarding the effectiveness of macrolide in CAP. However, this concern has never been assessed on a large scale in Korea.
The recommendation of antibiotics for the empiric treatment of CAP is based on the selection of agents that are effective against the major treatable bacterial causes of CAP. The 2019 guideline for empiric antibiotics for CAP published by American Thoracic Society and Infectious Diseases Society of America (ATS/IDSA) recommended beta-lactam plus macrolide combination therapy for both nonsevere and severe inpatients pneumonia.8 Alternatively, the 2019 British guideline recommended a beta-lactam monotherapy for nonsevere pneumonia and beta-lactam plus macrolide combination therapy for only suspected atypical pneumonia or severe pneumonia.9 The panel of 2019 ATS/IDSA guideline suggest that beta-lactam monotherapy should not be routinely used for inpatients with CAP over b-lactam/macrolide combination therapy.8 The 2017 Korean guideline recommended a beta-lactam alone for patients with mild to moderate pneumonia admitted to a general ward, and a beta-lactam plus macrolide combination therapy for only suspected atypical pneumonia or severe pneumonia, under limited circumstances.7 However, antibiotic treatment regimen for mild-to-moderate CAP has never been evaluated for Korean patients. This study demonstrated that beta-lactam plus macrolide combination therapy had a survival advantage over beta-lactam monotherapy in CAP requiring hospitalization (CURB-65 ≥ 2), which was not observed in the mild pneumonia (CURB < 2). This is the first nationwide study on this subject in Korea and consistent with 2017 Korean guideline for antibiotic use in adults with CAP.
The microbial etiology of CAP is changing, particularly with the emergence of the strains that show resistance to antibiotics in different regions around the world. Accordingly, questions have been raised regarding the need for combined macrolide treatment with increased macrolide resistance to atypical pathogen, as well as Streptococcus pneumoniae.
1822 A meta-analysis of 28 randomized controlled trials published in 2012 showed that empiric atypical coverage did not improve the prognosis in hospitalized CAP.23 However, a randomized non-inferiority trial study published in 2014 found a higher effectiveness of macrolide combination therapy for patients with severe pneumonia (CURB-65 ≥ 2),11 while a prospective cohort study published in 2019 showed that macrolide combination therapy significantly reduced the 30-day mortality of patients with severe CAP.24 The mechanisms underlying the observed superiority of macrolide combination therapy in the CAP are attributed to a broader coverage of unidentified infection with atypical pathogens, as well as immunomodulatory effects on host-pathogen interaction, an improvement in mucociliary clearance, and an attenuated inflammatory response.2526 This study suggests that despite the high prevalence of MRMP, macrolides still have a benefit on the empirical therapy in adult patients hospitalized with severe CAP.
In a British multicenter study published in 2013 including 5,240 adults hospitalized with CAP, beta-lactam and macrolide combination therapy was significantly associated with a lower 30-day inpatient death rate in patients with moderate-severity CAP (CURB-65 = 2) and high severity CAP (CURB-65 ≥ 3) but not low severity CAP (CURB-65 < 2).27 In the study, the 30-day readmission rate between the BM and B groups showed no significant difference. Our study using PSM also found no difference in the 30-day readmission rate between the two groups. The overall 30-day inpatient death rate was 24.4% in the British study, but only 3.7% in the present study. This difference could be attributed to the fact that the British study included 28.9% of CURB-65 ≥ 3 patients, while our study included 8.6% of CURB-65 ≥ 3 patients. Furthermore, our study excluded patients with underlying diseases, such as immunocompromised and dialysis patients with a high probability of developing severe pneumonia, resulting in high mortality. In the present study, other clinical outcomes were investigated and a statistically significant shortened total length of hospital stay, decreased total cost of antibiotics, and a decreased mortality rate during hospitalization were observed in the BM group than in the B group. These results are similar to those of a retrospective cohort study published in 2003 with 44,814 CAP patients, which also found that macrolide combination therapy was associated with decreased mortality and length of hospital stay.28 According to our results, the combined treatment of macrolide should be recommended rather than beta-lactam monotherapy in an adult CAP patient who is not an immunocompromised and has a score of CURB-65 ≥ 2.
Seasonal variabilities in the respiratory pathogens that cause CAP have been addressed in the literature for the pediatric and adult patients.293031 According to a previous study, Mycoplasma pneumoniae CAP reached a peak incidence of 41% in the spring of 1996, compared to an incidence of 15% during winter.31 Another study published in 2016 showed that atypical etiology in hospitalized CAP patients was associated with the seasons.32 According to a nationwide retrospective cohort study conducted in Korea between 2010 to 2015, hospitalized patients with Mycoplasma pneumoniae CAP was typically prevalent between early summer and autumn season.29 A retrospective cohort study conducted for 10 years with CAP patients (> 65 years) found that doxycycline combination therapy was associated with a lower 30-day mortality rate than regimens without doxycycline.33 However, to date, no studies have demonstrated the effect of macrolide combination therapy on hospitalized adult CAP patients according to seasonal variabilities. In the present study, we demonstrated that macrolide combination therapy is an effective empirical regimen for hospitalized CAP patients with CURB-65 ≥ 2, especially in autumn. The possible explanation for this is that we might underdiagnose atypical pathogens which is prevalent in autumn season.
It is estimated that 7% to 20% of CAP is secondary to atypical bacterial microorganisms.34 As the atypical pathogens have intra-cellular nature, they are not visible on Gram stain and are difficult to culture. Accordingly, the true number of cases is unknown. In Korea, one of the important atypical pathogens prevalent in autumn season is scrub typhus.35 According to the literature, clinical presentation of scrub typhus varies and eschar can be absent.3637 Respiratory complications of scrub typhus can be presented in the form of interstitial pneumonia frequently and the incidence of chest radiographic abnormalities in patients with scrub typhus varies from 59% to 72%.3839 Therefore, there is a possibility that the clinicians misdiagnose atypical pathogens including scrub typhus and treat it with ordinary CAP empiric antibiotics which can effect on the clinical outcome of CAP.
This study results showed the seasonal variation of CAP mortality regarding to macrolide combination therapy and the possibility of atypical pathogens effect on CAP mortality, especially prevalent in autumn season. Further studies on prevalence and distribution of CAP pathogens according to seasonal change are needed and we believe that early prediction of possible seasonal causative pathogens and adequate empiric antibiotic treatment before the identification of respiratory pathogens will improve clinical CAP outcomes.
This study has several limitations. First, since NHI data were used, we were unable to confirm the specific pathogen. However, at present, the type of antibiotic used to treat CAP mostly depends on empirical therapies due to the difficulties associated with isolating the causative pathogens.7 Despite this limitation, our results are significant in that the effect of macrolide combination therapy was confirmed, excluding immunocompromised patients who are at risk of being infected by MRMP, Pseudomonas, or methicillin-resistant Staphylococcus aureus.
Second, pneumococcal vaccination could affect the prognosis, but we could not include pneumococcal vaccination status in the PSM. Because, in this study, the presence or absence of pneumococcal vaccination history under the age of 65 was not confirmed, and over the age of 65, the presence or absence of pneumococcal vaccination history was not confirmed in about 30% of all patients. Although the vaccination rate was found to be lower in the BM group than in the B group, we found that the survival rate was higher in the BM group than in the B group.
Third, although the subgroup analysis of this study found that the effect of macrolide combination treatment was more pronounced in the autumn season, it was difficult to infer a clear rationale for this phenomenon. We suggest that further studies on seasonal differences in causative pathogens and treatment outcomes of CAP are necessary.
In conclusion, a beta-lactam plus macrolide combination therapy shows potential as an empirical therapy for CAP with CURB-65 ≥ 2, especially in autumn. It is a novel finding that the effectiveness of empirical antibiotics in CAP might be affected by seasonal factors. This study is the first nationwide population-based cohort study providing consistent evidence on the 2017 Korean guideline for antibiotics use in adults with CAP.
 XML Download
XML Download