

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vitamin D is a hormone responsible for maintaining calcium homeostasis and an essential nutrient that is related significantly to bone mineralization and fractures in humans [1]. With the discovery of vitamin D receptors in soft tissues, there is increasing interest in the relationship between vitamin D and extra skeletal diseases [234567]. Moreover, vitamin D deficiency and its insufficiency are global health issues that afflict more than one billion children and adults worldwide [8].
Most of the vitamin D in the blood circulation exists in the form of 25-hydroxyvitamin D (25(OH)D), which has a relatively long half-life of 2–3 weeks (1,25-dihydroxyvitamin D, the active form of vitamin D, has a half-life of only 4–6 h), and there is a high correlation with bone mineral density (BMD) [910]. Therefore, the blood level of 25(OH)D is the best indicator of the vitamin D nutritional status in the human body. According to the US Institute of Medicine (IOM), a blood 25(OH)D level of above 20 ng/mL is defined as sufficient, below 20 ng/mL as insufficient, and 12 ng/mL or less as deficient [11]. The World Health Organization (WHO) defines a vitamin D deficiency as a 25(OH)D level of 10 ng/mL or less [12].
The prevalence of vitamin D deficiency in Asians, including Koreans, has been reported to be between 45–90% in the general population and 78–98% in pregnant women [8]. According to the analysis of the 2009 Korean National Health and Nutrition Survey (KNHANES IV-3), the vitamin D deficiency rate in Korean adults was 61.8% for men and 75.4% for women [13]. The serum 25(OH)D levels of 322 Korean postmenopausal women surveyed in 2008 were at a deficient level (< 20 ng/mL) in 76.1% and at an insufficient level (21–29 ng/mL) in 18.3% of women. Moreover, 64% of the participants had osteoporosis and 28.9% had osteopenia [14].
The results of the 2008–2011 KNHANES (bone density was examined only during this period in Korea) indicated a prevalence of osteoporosis and osteopenia in women of 37.3% and 48.9%, respectively. In men, the prevalence of osteoporosis was 7.5%, which was 1/5 of that in women, while the prevalence of osteopenia was 46.8%, similar to that in women [15]. Moreover, over the past decade, it has been observed that the prevalence of osteoporosis among Korean adults increased from 6.1% to 13.1% in men and from 24.3% to 35.5% in women [16]. It is important to prevent osteoporosis because it greatly limits an individual's quality of life due to the increased incidence of fractures; however, it is difficult to treat [17]. In a previous study that analyzed the data from the 2009 KNHANES, the BMD of the total femur increased until serum 25(OH)D reached 20.4 ng/mL but did not increase proportionally above that. The authors stated that it is important to increase the serum 25(OH)D concentration to 20 ng/mL or higher for bone health in older Korean adults [18].
Ultraviolet (UV) radiation is essential for the production of vitamin D under human skin. However, since UV rays are known to affect carcinogenesis and skin aging, sunscreens are used to minimize the amount of UV rays. Therefore, if the UV irradiation dose is insufficient, vitamin D intake through the diet becomes more important to prevent vitamin D deficiency and related diseases and to maintain an appropriate nutritional status. Some studies have shown that dietary intake of vitamin D can contribute to improvements in serum 25(OH)D levels [19202122].
Vitamin D nutritional status and dietary intake in Koreans and related public health issues have not been sufficiently studied. Consequently, the Korean Dietary Reference Intake (KDRI) for vitamin D was established based on insufficient evidence. The purpose of this study was to evaluate the relationship among the vitamin D intake, serum 25(OH) D level, and BMD of Koreans utilizing large-scale 2009–2011 KNHANES, when BMD and serum 25(OH) D level were measured.
Go to : 
MATERIALS AND METHODS
Study participants
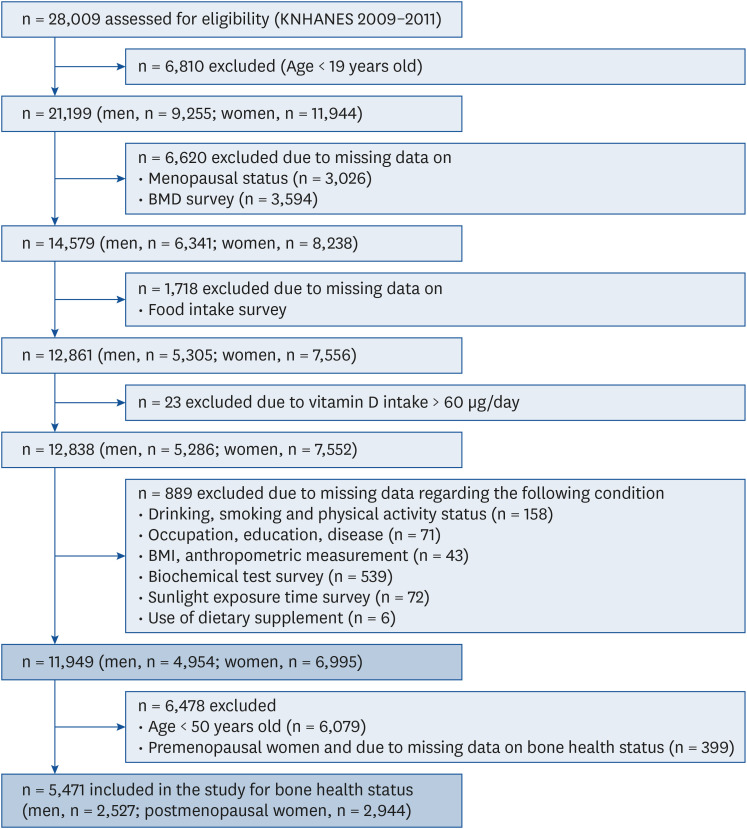
The 2009–2011 KNHANES (KNHANES IV-3, V-1, and V-2) analyzed data obtained from biochemical measurements, nutrition surveys, health interviews, physical examinations, and BMD tests. Of the 28,009 people (12,825 men and 15,184 women) who participated in the 2009–2011 KNHANES, 21,199 adults over the age of 19 yrs (9,255 men and 11,944 women) were selected. Among them, 3,026 women who did not have data on menopausal status, 3,594 participants without a BMD test, 1,718 without a food intake survey, 23 whose vitamin D intake level exceeded the upper limit intake level (> 60 µg/day), 229 who did not complete a health survey (158 without drinking, smoking and physical activity status, 71 without occupation, education, disease), 654 who did not undergo part of the medical examination (43 without BMI, anthropometric data, 539 without biochemical test, 72 without sunlight exposure time survey), and six who did not respond to questions regarding dietary supplements were excluded. The data of 11,949 people (4,954 men and 6,995 women) were used to analyze the relationship between vitamin D intake, serum 25(OH)D concentration, and BMD. In the analysis of the level of vitamin D intake according to the prevalence of osteoporosis, a total of 5,471 (2,527 men and 2,944 women) were included, excluding 6,079 participants under 50 yrs of age and 399 participants for whom osteoporosis prevalence was not investigated (Fig. 1). The KNHANES was conducted according to the guidelines of the Declaration of Helsinki and approved by the Research Ethics Review Committee of the Korea Centers for Disease Control and Prevention (approval number: 2009-01CON-03-2C, 2010-02CON-21-C, 2011-02CON-06-C). Informed consent was obtained from all participants involved in the study.
General characteristics
The age of the study participants and the amount of energy and calcium intake reported in nutrient intake surveys which employed the 24-h recall method, were used. Using sunlight exposure time survey, which was requested on one of the eye examination questionnaires, the study participants were classified into two groups based on their sunlight exposure time: less than 5 h per day or more than or equal 5 h per day.
Vitamin D intake
The daily intake of vitamin D in Korean adults was assessed using raw data on food intake collected using the 24-h recall method and the food vitamin D content database established in this laboratory [13]. Assessment of vitamin D intake unadjusted and adjusted for energy intake were conducted. The proportion of participants who ingested vitamin D below the adequate intake (AI) from the 2010 KDRI was calculated. Since KNHANES did not investigate the amount of nutrients consumed from supplements, vitamin D from supplements was not included in this study.
Serum 25(OH)D concentration
Serum 25(OH)D concentration was measured using a radioimmunoassay (RIA) with the 25(OH)D D125I RIA kit (DiaSorin, Stillwater, MN, USA) at the Neodin IOM. In this study, the cut-off point for a deficient serum 25(OH)D level was 20 ng/mL (50 nmol/L) [11]. We evaluated the relationship between vitamin D intake and blood 25(OH)D concentration after adjusting for the sun exposure time of the participants as a confounding factor.
BMD
Data on BMD were released from the KNHANES. The BMD was measured at three sites: femur total hip, femoral neck, and lumbar spine. The whole-body total BMD was calculated for the three abovementioned sites. The measurements were obtained with an X-ray bone density meter (DISCOVERY-W fan-beam densitometer; Hologic Inc., Marlborough, MA, USA) with dual-energy X-ray absorptiometry [23]. Bone health status was assessed using the Asian criteria of the WHO as follows: T-score above −1 for all BMD scores indicated a healthy bone health status, the lowest T-score between −2.5 and −1 among the three sites indicated osteopenia, and the lowest T-score of −2.5 or less among the sites indicated osteoporosis. To observe the relationship between vitamin D intake and BMD, the participants were divided according to vitamin D intake level: less than 5 µg and more than or equal to 5 µg after adjusting for serum 25(OH)D. In a previous study in which the differences in BMD were examined by dividing participants according to vitamin D intake into the following three groups: less than 5 µg/day, 5–10 µg/day, and 10 µg/day or more, similar results were observed in the group that ingested more than 10 µg/day and the group that ingested 5–10 µg/day of vitamin D. Therefore, the selected cut-off point in this study was 5 µg/day [21].
The average daily vitamin D intake was analyzed according to bone health status (normal, osteopenic, and osteoporotic) in 2,527 men over 50 yrs and 2,944 postmenopausal women.
Statistical analysis
A complex sample analysis of the KNHANES data for weighting was conducted according to the guidelines of the Korea Centers for Disease Control and Prevention. The statistical analyses were performed using the SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). In the analysis of the general characteristics, categorical variables—vitamin D intake level, serum 25(OH)D concentration, and BMD of the participants—were expressed as frequencies and percentages (%), and for continuous variables, the means and standard deviations were calculated. The χ2 test was used to estimate the differences in the distribution of categorical variables, and the t-test or analysis of variance (ANOVA) test was conducted to determine the mean differences in the continuous variables. The relationship between vitamin D intake and serum 25(OH)D was tested using a linear regression analysis of the complex samples of the general linear model, after adjusting for UV exposure which was a confounding factor. Daily vitamin D intake after adjusting for energy intake, BMD according to vitamin D intake level, and nutrient intake according to bone health status, was tested using an analysis of covariance (ANCOVA). In the ANCOVA test, the energy intake for the analysis of vitamin D intake, serum 25(OH)D for the analysis of BMD according to vitamin D intake, and age, energy intake, and calcium intake for the analysis of vitamin D intake according to bone health status, were adjusted by including it in the analysis model as a covariate. A Tukey's post hoc comparison was performed after the ANOVA and ANCOVA. In all statistical analyses, the significance level was set at α = 0.05.
Go to :
RESULTS
General characteristics
The mean age of the study participants was 44.5 yrs for men and 45.6 yrs for women. The average daily energy and calcium intakes were 2,398.8 ± 17.3 kcal/day and 586.3 ± 6.3 mg/day, respectively for men and 1,674.4 ± 11.4 kcal/day and 454.4 ± 5.1 mg/day, respectively for women. The serum 25(OH)D was significantly higher in men (18.6 ± 0.2 ng/mL) compared with women (16.4 ± 0.2 ng/mL). Significantly more men (25.9%) were exposed to sunlight for more than 5 h per day than women (13.3%) (Table 1).

Table 1
General characteristics of the participants
Variables are expressed as mean ± SE and numbers (frequencies [%]).
25(OH)D, 25-hydroxyvitamin D.
1)The P-value is derived from an independent t-test for the continuous variables and χ2 test for the categorical variables.
![]()
Vitamin D intake, serum 25(OH)D concentration, and BMD
The average daily vitamin D intake before adjusting for energy intake was significantly higher in men (4.22 ± 0.13 µg/day for men vs. 2.72 ± 0.07 µg/day for women). The highest and lowest vitamin D intakes in men were in the 30–49 yrs age group (4.80 ± 0.19 µg/day) and the 75 yrs and over age group (1.65 ± 0.21 µg/day), respectively (P < 0.001, Table 2). The highest and lowest vitamin D intakes in women were in the 30–49 yrs age group (3.14 ± 0.12 µg/day) and the 75 yrs and over age group (1.16 ± 0.11 µg/day), respectively (P < 0.001). After adjusting for energy intake, the difference in vitamin D intake between the age groups remained the same for both men and women (P < 0.001), whereas the difference in vitamin D intake between men and women, decreased. Vitamin D intake adjusted for energy intake was greater in women than men in the 19–29 yrs age group and the 75 yrs and over age group. In 2010, the KDRI established the AI for vitamin D as 5 µg for adults aged 19–49 yrs and 10 µg for those aged 50 and older. In this study, the percentage of participants with less than AI of vitamin D was 74.0–96.5% for men and 83.8–98.8% for women. The serum 25(OH)D level was the lowest in both men and women aged 19–29 yrs and the highest in men aged 65–74 yrs and in women over 75 yrs (P < 0.001). The deficiency ratio of serum 25(OH)D with 20 ng/mL as the cut-off point was 45.9–78.4% for men and 65.3–86.4% for women. BMD was highest in all the areas in men aged 19–29 yrs and it decreased in the older age groups (P < 0.001). In women, apart from the femoral neck area, BMD was the highest in the 30–49 yrs age group, and it decreased with older age.
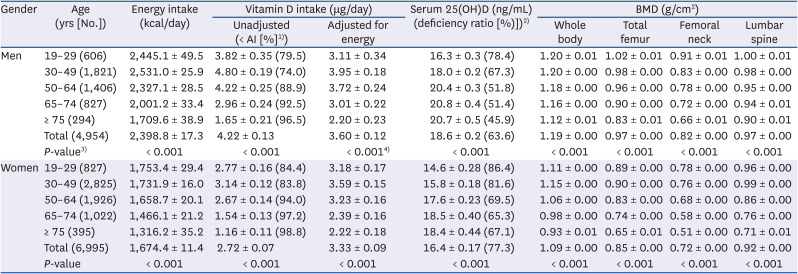
Table 2
Average of vitamin D intake, serum 25(OH)D concentration, and BMD of Korean adults by gender and age
All variables are expressed as mean ± SE.
25(OH)D, 25-hydroxyvitamin D; AI, adequate intake.
1)AI as per the 2010 Korean Dietary Reference Intake, refers to 5 μg/day for adults aged 19–49 yrs, and 10 μg/day for adults aged ≥ 50 yrs.
2)Cut-off point for the deficient serum 25(OH)D concentration is 20 ng/mL.
3)The P-values were derived from the analysis of variance.
4)The P-value were derived from the analysis of covariance after adjusting for energy intake.
![]()
Vitamin D intake and serum 25(OH)D concentration
The relationship between vitamin D intake and serum 25(OH)D concentration before and after adjusting for sunlight exposure is shown in Table 3. The relationship between the two variables was examined by classifying the total study population (men and women) into two age groups: participants under 50 yrs and participants ≥ 50 yrs. In all the groups except the female group under 50 yrs and the male group ≥ 50 yrs, there was a significant positive relationship between the two variables. These results were the same even after adjusting for sunlight exposure.

Table 3
Relationship between vitamin D intake and serum 25-hydroxyvitamin D in Korean adults aged < 50 and ≥ 50 yrs
CI, confidence interval.
1)The P-value was derived from the generalized linear regression analysis of the complex samples.
![]()
Vitamin D intake and BMD
After dividing the participants according to age, we examined the difference in BMD between the group with a daily vitamin D intake of less than 5 µg/day and the group with an intake of more than or equal to 5 µg/day. This result was derived after adjusting for serum 25(OH)D (Table 4). In all the male participants, the total femur (0.99 g/cm2) and femoral neck (0.84 g/cm2) BMDs of the group with a vitamin D intake of 5 µg/day or more, were significantly higher than those of the group who consumed less than 5 µg/day (0.97 g/cm2 and 0.82 g/cm2, respectively; P < 0.01 and P < 0.05, respectively). These results were similar in men over 50 yrs, but there was no difference in the BMD according to the level of vitamin D intake in the group under 50 yrs. In all the women, all BMDs and whole-body BMD were significantly higher in the 5 µg or more/day intake group than in the less than 5 µg/day intake group (P < 0.001). These results were similar in women ≥ 50 yrs. In women ≥ 50 yrs, the whole-body BMD was 1.04 g/cm2 when the vitamin D intake was 5 µg/day or more, and 1.02 g/cm2 when the vitamin D intake was less than 5 µg/day. However, in women under the age of 50 yrs, there was no difference in BMD according to the level of vitamin D intake.
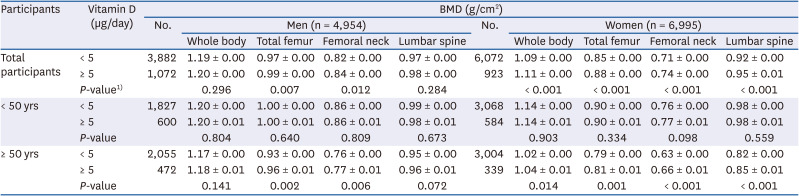
Table 4
BMD according to vitamin D intake level after adjusting for serum 25-hydroxyvitamin D concentration
Variables are expressed as mean ± SE.
BMD, bone mineral density.
1)P-value were derived from the analysis of covariance.
![]()
Vitamin D intake according to the bone health status
Men ≥ 50 yrs and menopausal women were classified into normal, osteopenic, and osteoporotic groups according to their bone health status. The average daily intakes of vitamin D, calcium, and energy in the three groups were analyzed (Table 5). The average daily intake of vitamin D was presented after adjusting for age, energy, and calcium intake, and the results without adjustment. In men, the percentage of participants with normal BMD and osteopenia were 47.6% and 45.7%, respectively while the percentage of participants with osteoporosis was insignificant (6.7%). In women, the percentage of participants with osteopenia and osteoporosis was 50.7% and 35.3%, respectively, indicating lower bone density than that in men. Bone health status was poor with age in all the study participants (P < 0.001). Energy and calcium intakes were the highest in both men and women in the normal group and the lowest in the osteoporotic group (P < 0.001). Vitamin D intake before adjustment for the confounding factors was the highest in normal men, followed by men with osteopenia and men with osteoporosis (P < 0.05). Vitamin D intake in women was significantly lower in the osteoporotic group than in the normal or osteopenic groups (P < 0.001). After adjusting for the confounding factor, there was no difference between the three groups for men; however, in women, the vitamin D intake in the osteopenic group was higher than in the osteoporotic group (P < 0.05).
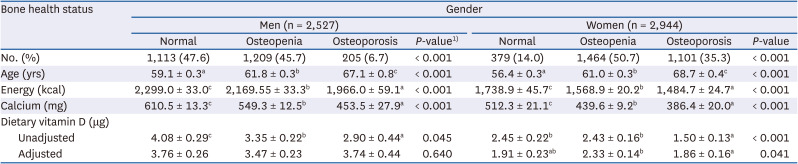
Table 5
Age and nutrients intakes by bone health status in men and postmenopausal women aged ≥ 50 yrs
Values are expressed as mean ± SE.
The differences between groups were evaluated by the analysis of covariance and Tukey's post hoc comparison test after adjusting for age, energy, and calcium intake.
1)The P-value is derived from the χ2 test for the categorical variables and from the analysis of variance and Tukey's post hoc comparison test for the continuous variables.
![]()
Go to :
DISCUSSION
This study was conducted to determine the vitamin D intake in Korean adults using the 2009–2011 KNHANES and the vitamin D food database established in our laboratory [132124], and its relationship to serum 25(OH)D or BMD. Although the data for each year were analyzed in our previous study, the relationship between vitamin D intake and BMD and serum levels of vitamin D was not established due to the exclusion of large number of participants who did not meet the study criteria. Using the same vitamin D database, this study integrated and re-analyzed the data from the 2009–2011 KNHANES.
Total vitamin D intake was significantly higher in men than in women, but after adjusting for energy intake, the intake in women was higher in the 19–29 and 75 and over age groups, and the differences between the sexes was reduced in the 30–74 age group. These results indicated that the nutrient density of vitamin D in diet was higher in Korean women than in Korean men. In a study based on the 2009 KNHANES, vitamin D intakes from seafood and eggs, which are major dietary sources of vitamin D in Korean adults [13], there were no significant differences among the groups divided by bone health status (the normal, osteopenic, and osteoporotic groups). However, the consumption of milk was greater in healthy participants and those with osteopenia than in those with osteoporosis (0.27 µg/day in the normal group, 0.20 µg/day in the osteopenic group, and 0.07 µg/day in the osteoporotic group) [24]. Nevertheless, in Korea, vitamin D deficiency continued to show an increasing trend between 2008 and 2014 [25].
Until recently, studies on the amount of vitamin D intake in Koreans have been scarce; therefore, it was difficult to understand the annual trends. In a 2015 study on 200 menopausal women aged 49–69, vitamin D intake was 3.7 µg/day in summer and 3.3 µg/day in winter, which was 38% of the AI as per the KDRI [26]. Although the participants were postmenopausal women, 60% of them had a normal bone health status and 33% had osteopenia. Compared to the participants in our study, these were people with significantly better bone health, and accordingly, the intake of vitamin D was higher. Although, the mean vitamin D intake in European adults (35–74 yrs) was reported to be 4.8 and 3.3 µg/day for men and women, respectively [27], there was considerable variation across countries. These levels are slightly lower than the vitamin D intake of Korean adults. Age-adjusted dietary vitamin D intake in US adults was 6.15 µg/day and 4.53 µg/day in men and women, respectively, during 2007–2009 [28]. While this represented a decreasing trend compared to that in 1980–1982, their intake levels are still higher than that of Koreans. According to the 2007 FINdiet study, the vitamin D intake in men in Finland was 7.1 µg/day and 5.2 µg/day for women [29], and the contribution of milk products fortified with vitamin D was high. In 2018, the dietary vitamin D intake of men and women aged 20–69 yrs in the northern and southern regions of Japan was reported to be 5.2–5.4 µg/day [22], which was significantly higher than that of Koreans. Even if UV exposure is the most plausible way to improve vitamin D nutritional status, increasing dietary vitamin D intake can serve as an alternative when UV exposure is insufficient [303132]. However, it is difficult to increase vitamin D intake due to the limited vitamin D source foods and low consumption of dairy products by Koreans. To this end, fortification of foods with vitamin D, which has been implemented and verified in advanced countries, could be an appropriate option [33]. Alternatives for improving vitamin D intake and status, including mandatory or voluntary vitamin D fortification, have been implemented in many high-income countries [34].
Since human BMD depends on the nutritional status of vitamin D and calcium, and blood vitamin D concentration is closely related to bone density [214], it was necessary to first determine the relationship between vitamin D levels in the blood and vitamin D intake through diet. The prevalence of vitamin D deficiency in Korean adults (serum 25(OH)D < 20 ng/mL) was 77.3% in women and 63.6% in men, with the highest deficiency rate in the 20s age group. In both sexes, vitamin D intake decreased after the age of 50, while the concentration of 25(OH)D remained high. This can be attributed to differences in UV exposure due to an increase in leisure time [353637], the quality of meals, intake of supplements, and maintenance of vitamin D concentration in the blood due to decreased calcium absorption [263839]. UV exposure is the most important factor for the maintenance of serum vitamin D, so we aimed to determine the relationship between vitamin D intake and serum 25(OH)D levels after adjusting for sunlight exposure time. The index related to UV exposure from the KNHANES data was obtained from an eye examination. Since this was a survey item that only investigated whether or not the sunlight exposure time was more than or equal 5h, there was a limitation in that more accurate results would have been obtained had we measured continuous qualitative values. As a result, there was a significant positive association between vitamin D intake and serum 25(OH)D in men < 50 yrs and in women 50 yrs or older. While the results of previous study were confirmed by the current results in men, the results for women appeared to be significant only after data integration.
Although inconsistent results have been reported for different age groups and sexes, several studies have reported the relationship between vitamin D intake and serum 25(OH)D levels. It was reported that the serum 25(OH)D in northern Europe was lowered during the winter and that vitamin D intake through nutrition could be helpful during this period [4041]. In a Japanese study, it was suggested that a 1 µg/1,000 kcal increase in vitamin D intake can increase 25(OH)D by 0.88 and 1.7 ng/mL in summer and winter, respectively [35].
On the other hand, most studies on the prevention of bone disease with vitamin D intake, have report that vitamin D supplementation affects musculoskeletal endpoints, such as the reduction of fractures and falls [42]. However, these results were established only when the concentration of 25(OH)D in the blood was above the threshold [43]. Since the serum 25(OH)D level and vitamin D intake in Koreans is low, it is difficult to apply the above results. In this study, the relationship between vitamin D intake and BMD was examined after adjustments for serum 25(OH)D. As a result, BMD was higher in the group with a vitamin D intake of 5 µg/day or more than in the group with a vitamin D intake less than 5 µg/day, in both sexes over 50 yrs. In particular, there were significant differences in all the BMD areas in women, therefore, the relationship between the two variables was more pronounced in women. These results were the same as those obtained in a previous study that re-analyzed the results of the 2011 KNHANES [21].
The level of vitamin D intake in Koreans over 50 yrs of age according to bone health status was significantly higher in the normal group than in the osteoporotic group among both men and women. However, since the mean age and nutrient intake of each group were significantly different, the data were analyzed after adjusting for age, calcium, and energy intake. In women, the intake of vitamin D was significantly lower in the osteoporotic than in the osteopenic group. The vitamin D intake of the normal group was between that of the osteoporotic and the osteopenic groups. Korean women maintain their dietary quality by paying attention to their BMD until their 60s, but dietary quality was lower in the older age group, such as the osteoporotic group. Feskanich et al. [44] reported that in postmenopausal women, a group who consumed 6.35 ug/day of vitamin D had a 43% lower risk of fracture than a group who consumed 2.5 ug/day. Polzonetti et al. [45] reported that diet moderately affected osteoporosis, and calcium and vitamin D intake was critical in older patients. In a randomized controlled study with a plant-based dietary intervention for coronary health improvement, diets low in dairy products were associated with an increased risk of osteoporosis [41]. A meta-analysis, including nine studies, showed a lower BMD in vegans than in milk consumers [46]. According to recent studies, the beneficial effects of vitamin D supplementation on bone health occurred when the baseline 25(OH)D concentration was ≤ 12 ng/mL [47]. Considering that the average serum 25(OH)D of Korean women over the age of 50 was 17–18 ng/mL, many would have had serum levels below 12 ng/mL; therefore, strategies for bone health improvement are required for these people. It is also necessary to improve the dietary quality along with calcium intake, which was only 386–512 mg/day. A previous study of the 2009–2010 KNHANES indicated that low calcium intake is damaging to bone health which could not be rectified by raising serum 25(OH)D level [48]. They suggested that at least 668 mg/day of calcium intake is required at serum 25(OH)D levels above 20 ng/mL to maintain bone mass. In our previous study, the BMD of the participants depended on vitamin D intake level when calcium intake was below the 3rd quartile (484–699 mg/day) [24].
This study had some limitations. First, since KNHANES is a cross-sectional study, the cause-effect relationship cannot be clearly established. Second, it was not possible to determine the amount of vitamin D intake through supplements, and food intake was investigated using only a single 24-h dietary recall. Third, BMD bias may have occurred in the elderly, making it difficult to assess the correlation accurately, since the value of BMD in KNHANES was derived without considering the bone marrow and subcutaneous fat [495051]. Nevertheless, the significance of this study was its examination of the relationship between the status of vitamin D intake and bone disease in Koreans using large-scale national survey data and a newly established vitamin D database. This study revealed an insufficiency in the nutritional status of vitamin D in Koreans; therefore, various measures need to be taken to improve their nutritional status. Polzonetti et al. [45] proposed an increase in the intake of natural vitamin D-containing foods, the production of vitamin D-fortified foods, the use of vitamin D supplements, increased UV-B exposure, and weight loss, as strategies to improve the vitamin D status of the population.
In conclusion, the amounts of calcium and vitamin D intakes were very low among Korean adults, and the prevalence of vitamin D deficiency (< 20 ng/mL) was 64% in men and 77% in women. Among the postmenopausal women 50 yrs or older, 86% had poor bone health (osteopenia or osteoporosis). The BMD of women over 50 yrs old with a vitamin D intake of 5 µg/day or more was significantly higher than the BMD of those with an intake less than 5 µg/day. To improve the vitamin D status in Korean adults, it is necessary to increase the consumption of foods rich in vitamin D based on the Korean dietary pattern (increasing the intake of seafood, eggs, and sun-dried mushrooms) to elevate serum 25(OH)D levels. Subsequent research is warranted to evaluate the amount of vitamin D consumed in the form of supplements by Koreans. Since the dietary intake of vitamin D was limited to Koreans in this study, the importance of implementing formal public health policies, based on successful cases in other countries, should not be overlooked.
Go to :
 XML Download
XML Download