

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Gastric cancer (GC) ranks fifth in morbidity and third in cancer-related mortality among malignancies worldwide [1], and it has a relatively higher prevalence in East Asian countries [2]. Cases of GC increase with increasing age, and the peak incidence occurs in the 7th decade of life, making GC that mainly affects the elderly population [345]. Generally, GC among elderly patients is more complex and severe, with a higher risk of frailty resulting from comorbidities and malnourishment [46], a higher risk of surgical complications [78], and a shorter life expectancy than in the young population.
Previous studies have shown that several clinicopathological factors, including tumor location in the entire stomach, tumor size, stage, vascular invasion, perineural invasion and adjuvant chemotherapy, are related to a poor prognosis in elderly GC patients [9]. Comorbidities may impact survival in cancer patients. Cancer-specific survival (CSS) was found to be reduced among patients with comorbidities in some studies [10]. However, other studies did not find associations between CSS and comorbidities [1112]. The impact of comorbidities on CSS is not consistent and is likely to vary depending on the severity of the comorbidity, prognostic factors for the cancer, the stage of the cancer and the impact of treatment [1213].
Moreover, elderly cancer patients have a high prevalence of malnutrition, ranging from 19% to 55% [141516], and that proportion is even higher in GC patients, reaching up to 80% [17]. Malnutrition has been shown to be associated with poor survival in GC patients [18]. Recent studies have been dedicated to developing risk models for overall survival (OS) and CSS in GC patients after gastrectomy [192021], which might be more beneficial and urgently needed in the elderly population. Therefore, we aimed to identify the potential risk factors for CSS in elderly GC patients after gastrectomy at an academic Chinese medical center.
SUBJECTS AND METHODS
Participants and study design
All patients included in our study were consecutively admitted to our hospital from January 2013 to December 2017. The inclusion criteria were as follows: (1) age ≥ 70 yrs, (2) selective curative gastrectomy, and (3) pathological diagnosis of gastric adenocarcinoma. Patients who underwent emergency surgery, had other malignancies, had incomplete clinicopathological data or were lost to follow-up were excluded from the study. We defined age ≥ 70 yrs as “elderly” in this study based on the published literature [2223]. The primary endpoint was cancer-related death, and CSS was defined as the duration from operation to cancer-related death. All patients had regular follow-up visits, and the follow-ups were updated by January 31, 2020. The study protocol was reviewed and approved by the Institutional Review Board of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, for a quick pass based on its retrospective nature. The IRB number is PUMCH-B117. Each patient provided written informed consent.
Data collection and evaluation
We collected clinicopathological data, including sex, age, history of smoking, Charlson comorbidity index (CCI) score without age adjustment [24], American Society of Anesthesiologists (ASA) score, ICU admission, perioperative blood transfusion, tumor differentiation grade and the tumor, node, and metastasis (TNM) stage based on postoperative pathological reports. Age was defined at the time of inpatient admission. The criteria for ICU admission were as follows: (1) postoperative need for hemodynamic monitoring and frequent nursing care; (2) a high risk of postoperative respiratory complications requiring mechanical ventilation, such as patients with chronic obstructive pulmonary disease; and (3) cardiac function evaluated by cardiologists as being high risk and needing continuous monitoring and dose adjustment. GC staging was performed according to the 7th Union for International Cancer Control & American Joint Committee on Cancer (UICC & AJCC) staging system for gastric cancer [25].
Nutritional variables included preoperative body mass index (BMI), weight loss, Nutritional Risk Screening 2002 (NRS 2002) [26], Prognostic Nutrition Index (PNI) [15], and serum hemoglobin, albumin and prealbumin levels. BMI was defined by weight (kg)/height(m)2 at admission. Preoperative weight loss was defined as losing at least 5% of one’s total body weight within 12 mon before surgery. NRS 2002 is a widely used tool to screen nutritional risk in hospitalized patients from three dimensions, including severity of diseases, severity of malnutrition and age (see full chart in Supplementary Table 1) [26]. An NRS 2002 score ≥ 3 indicated nutritional risk, and an NRS 2002 score ≥ 5 indicated high nutritional risk. The PNI scores were calculated as follows: 10 × serum albumin value (g/dL) + 0.005 × peripheral lymphocyte count (/mm3) [15]. A PNI score < 45 indicated poor nutritional status.
We collected surgical data, including approaches to gastrectomy, dissection area of the stomach and perigastric lymph nodes, combined resection of organs, duration of operation, and intraoperative blood loss. The combined resection of organs refers to gastrectomy combined with surgical removal of the spleen, part of the transverse colon, or part of the pancreas. We used 240 min as the cutoff for the operation duration [27] and 400 mL as the cutoff for intraoperative blood loss [28]. Most patients had regular visits to our clinic annually; for those who did not visit us over one yr, we made phone calls to update their survival status. Death date and causes were reported by the families. Patients who died from causes other than GC were recorded as censored. CSS was defined as days from the operation date to the date of death, loss to follow-up or the end of the study.
Statistical analysis
Continuous variables are presented as the means ± SD or medians with interquartile ranges. Categorical variables are described as numbers and percentages. We included all the clinicopathological, nutritional and surgical variables in the univariate analysis to identify the potential risk factors for CSS, then we assessed the effects of covariates on univariable association by multivariate analyses. Variables in univariate analyses with P < 0.05 were included in multivariate analysis, including age, ICU admission, TNM stage II, III, and all the nutritional variables. Hazard rations (HRs) and 95% confidence intervals (CIs) were calculated and reported both in the univariate and multivariate analyses. The Cox model was used to perform survival analysis to simultaneously assess the effects of several risk factors on survival time. A receiver operating characteristic (ROC) curve was used to identify the cutoff value for BMI. Survival curves were estimated by the Kaplan–Meier method using the log-rank test. P < 0.05 was regarded as statistically significant. All statistical analyses were performed using SPSS for Windows (version 20; IBM Corp., Armonk, NY, USA).
RESULTS
In our database of 1,446 consecutive EGC patients, 290 patients met the inclusion and exclusion criteria and were included in the study (Fig. 1). In this cohort, 290 patients had a median follow-up duration of 31 (1–77) mon. There were 86 deaths in total during the follow-up, including 68 tumor-related deaths. The postoperative 1-, 3-, and 5-yr CSS rates were 93.7%, 75.9% and 65.1%, respectively. The characteristics of these patients categorized into clinicopathologic, nutritional and surgical outcomes are summarized in Tables 1, 2 and 3, respectively.
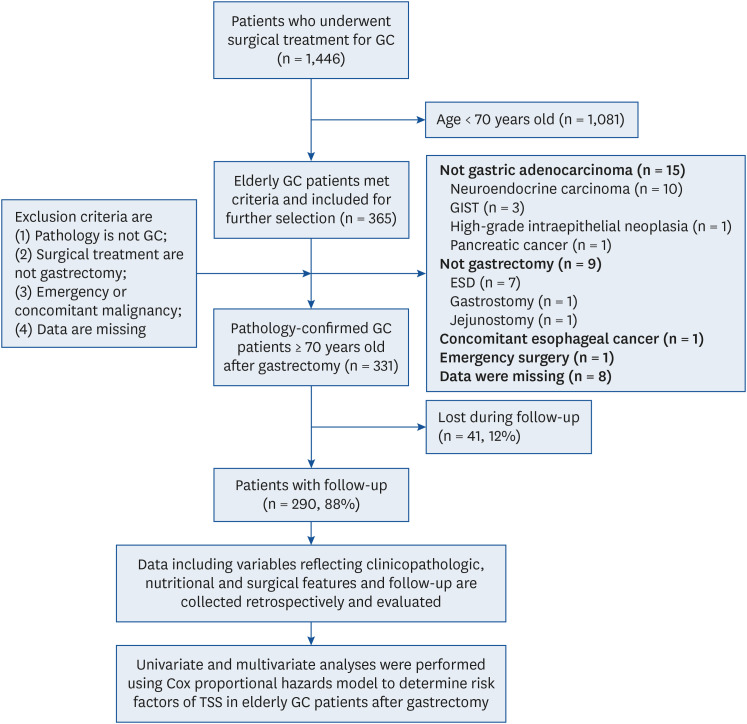
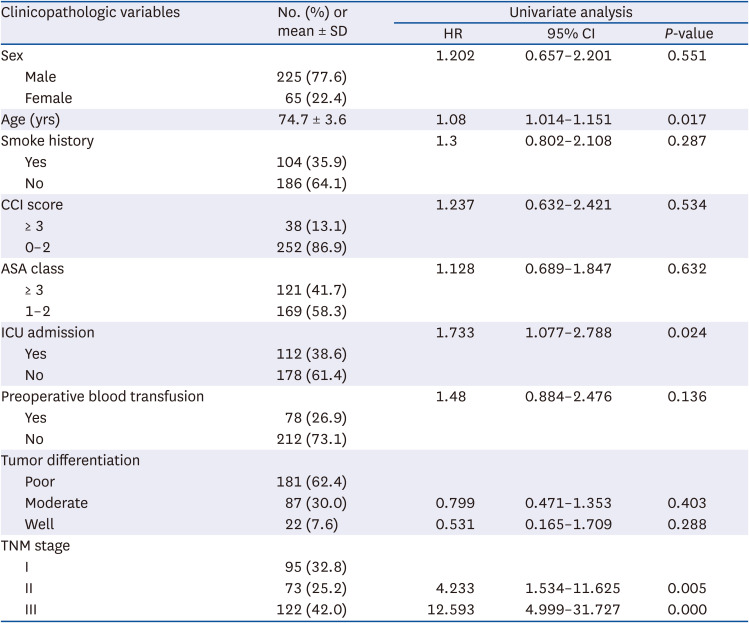
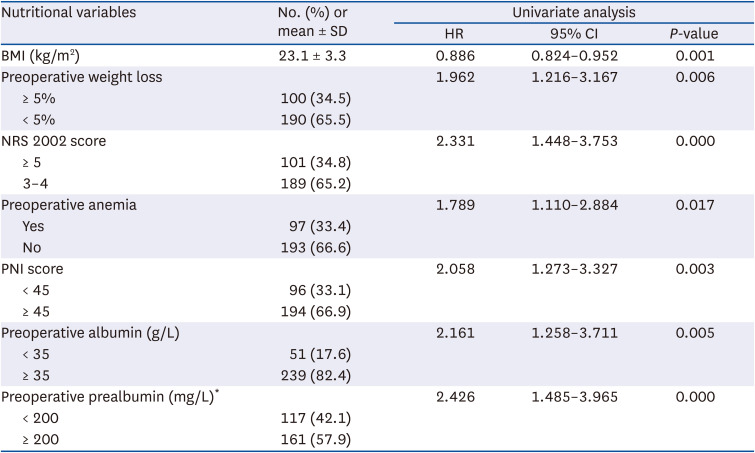
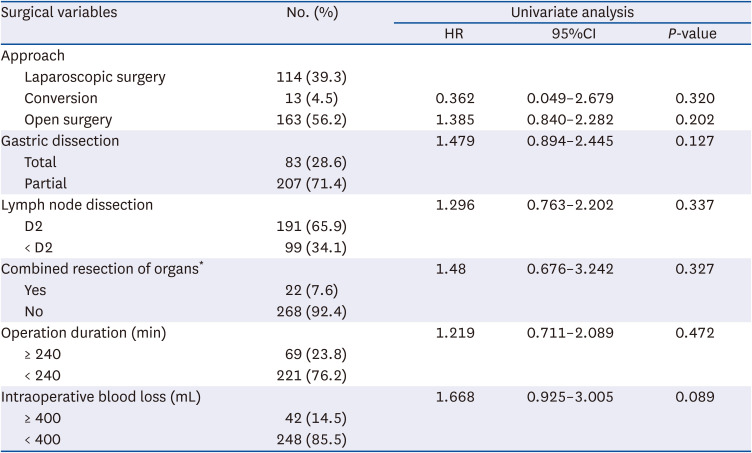
Fig. 1
Flow diagram shows inclusion and exclusion criteria of patients and study design. Missing data refers to loss of pathological, laboratory tests or surgical records.
GC, gastric cancer; GIST, gastrointestinal stromal tumor; ESD, endoscopic submucosal dissection; TSS, tumor-specific survival.
![]()
Table 1
Clinicopathologic variables and risk factors of CSS in univariate analysis
CSS, cancer-specific survival; CCI, Charlson comorbidity index; ASA, American Society of Anesthesiologists; ICU, intensive care unit; TNM, tumor node, and metastasis; HR, hazards ratio; CI, confidence interval.
![]()
Table 2
Nutritional variables and risk factors of CSS in univariate analysis
CSS, cancer-specific survival; BMI, body mass index; NRS 2002, Nutritional Risk Screening 2002; PNI, Prognostic Nutrition Index; HR, hazards ration; CI, confidence interval.
*Preoperative prealbumin value of 12 patients were missing.
![]()
Table 3
Surgical variables and risk factors of CSS in univariate analysis
CSS, cancer-specific survival; HR, hazards ration; CI, confidence interval.
*Combined resection of organs refers to gastrectomy combined with spleen, part of transverse colon, or part of pancreas.
![]()
Clinicopathologic characteristics at baseline and its associations with cancer-related death
Among the 290 EGC patients, the average age was 74.7 ± 3.6 yrs, and 77.6% were male. A total of 38 (13.1%) had CCI scores ≥ 3, and 121 (41.7%) of all included patients were classified as ASA class ≥ 3, indicating a relatively high percentage of patients with fragility as a cohort of elderly hospitalized populations. In total, 112 (38.6%) of the patients were admitted to the ICU after surgery, and 78 (26.9%) of the patients underwent perioperative blood transfusion. Pathological reports showed that 195 (67.2%) patients had locally advanced GC, and 181 (62.4%) had poorly differentiated GC. Univariate analysis demonstrated that the risk factors for CSS included age (HR = 1.08; 95% CI, 1.01–1.15), ICU admission (HR = 1.73; 95% CI, 1.08–2.79) and pathological TNM (pTNM) stage (stage II: HR = 4.23; 95% CI, 1.53–11.63; stage III: HR = 12.59; 95% CI, 5.00–31.73; Table 1).
Nutritional outcomes
In terms of the nutritional assessment, 100 (34.5%) patients had preoperative weight loss ≥ 5%, 101 (34.8%) had an NRS 2002 score ≥ 5 and 96 (33.1%) had a PNI score < 45. These three parameters had relatively high consistency, implying that over 1/3 of all elderly GC patients were at a high nutritional risk. In addition, the proportions of patients with anemia, hypoalbuminemia and low prealbumin levels were 33.4%, 17.6% and 42.1%, respectively. Single serum nutritional variables had large ranges of prevalence of nutritional risk. At baseline, BMI (HR = 0.89; 95% CI, 0.82–0.95), weight loss ≥ 5% (HR = 1.96; 95% CI, 1.22–3.17), NRS 2002 score ≥ 5 (HR = 2.33; 95% CI, 1.45–3.75), PNI score < 45 (HR = 2.06; 95% CI, 1.27–3.33), anemia (HR = 1.79; 95% CI, 1.11–2.88), an albumin level ≤ 35 g/L (HR = 2.16; 95% CI, 1.15–4.28) and a prealbumin level < 200 mg/L (HR = 2.43; 95% CI, 1.49–3.97) were significantly associated with CSS in univariate analysis (Table 2). Furthermore, an ROC curve was generated, and a BMI of 20.6 kg/m2 was determined to be the optimal cutoff value in our cohort of patients to categorize these patients into low and high BMI groups (Fig. 2A). The 5-yr CSS was significantly higher in patients with a BMI > 20.6 kg/m2 than in those with a BMI ≤ 20.6 kg/m2 (72% vs. 39%; Fig. 2B).
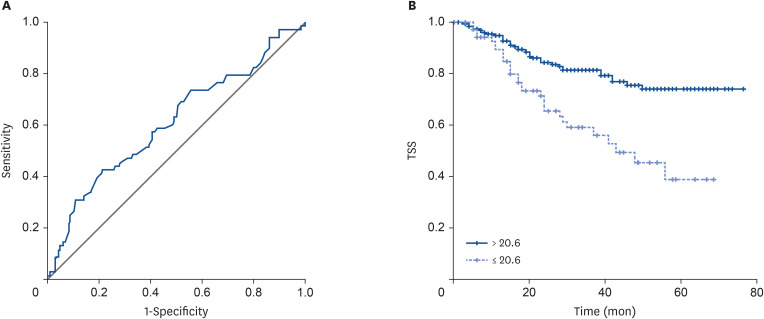
Fig. 2
(A) ROC curve showed the predictive accuracy of BMI values for tumor-specific survival. AUC was 0.61 (95% CI, 0.53–0.69, P = 0.006). Youden index was 0.21, sensitivity was 0.43 and specificity was 0.79. The BMI cut-off value was 20.65 kg/m2. (B) TSS was compared between low BMI and high BMI groups using the novel cut-off value, 20.6 kg/m2, in Kaplan-Meier method. Log-rank test was performed and χ2 was 16.27, P < 0.001.
ROC, receiver operating curve; BMI, body mass index; AUC, area under curve; CI, confidence interval; TSS, tumor-specific survival.
![]()
Surgical outcomes
In total, 56.2% of patients underwent open surgery, 39.3% underwent laparoscopic surgery, and 4.5% underwent conversion from laparoscopic to open procedures. In terms of resection areas of the stomach, perigastric lymph nodes and surrounding organs, 28.6% received total gastrectomy, 65.9% underwent D2 lymphadenectomy, and 7.6% had combined resection of other organs (Table 3). However, none of these surgical variables were significantly associated with CSS.
Independent risk factors for CSS
In univariate analyses, we found that age, ICU admission, TNM stages II and III in Table 1, and all the nutritional variables in Table 2 were associated with CSS. Then we included these variables in multivariate analyses to identify independent risk factors for CSS by using a Cox proportional hazards model. It is demonstrated that a BMI ≤ 20.6 kg/m2 (HR = 2.30; 95% CI, 1.36–3.87), ICU admission (HR = 1.97; 95% CI, 1.17–3.30) and pTNM stage (stage II: HR = 5.56; 95% CI, 1.59–19.43, P = 0.007; stage III: HR = 16.202; 95% CI, 4.99–52.59) were significantly associated with CSS (Table 4). Therefore, these variables were identified as independent risk factors for poor CSS in EGC.
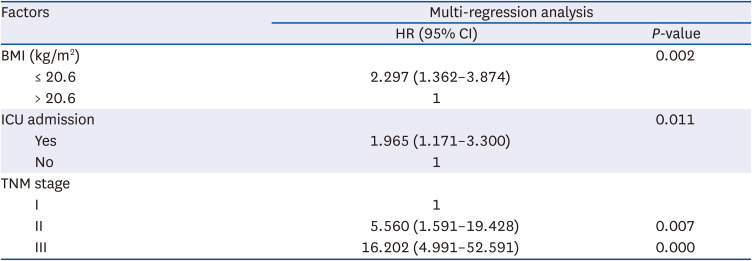
Table 4
Independent risk factors of CSS were in multivariate analysis using Cox proportional hazards model
Variables in univariate analyses with P < 0.05 were included in multivariate analyses using Cox model.
CSS, cancer-specific survival; HR, hazards ratio; CI, confidence interval; BMI, body mass index; ICU, intensive care unit; TNM, tumor, node, and metastasis.
![]()
DISCUSSION
In this study, we collected clinicopathological data from a cohort of EGC patients aged ≥ 70 yrs. We aimed to investigate the potential risk factors for CSS in these patients. In particular, we focused on nutritional parameters in this cohort, since elderly patients may have worsened appetite and decreased food intake, leading to a poor nutritional status. Indeed, approximately one-third of these patients were at a high nutritional risk, whether using the NRS 2002 tool (34.8%) or the PNI (33.1%,
Table 2). Additionally, 34.5% of these patients had weight loss ≥ 5% within 12 mon before surgery. Multivariate analysis indicated that a BMI ≤ 20.6 kg/m2, ICU admission and advanced pTNM (stages II and III) were independent risk factors for CSS.
Our study demonstrated that a low BMI predicted poor survival in GC patients, which was consistent with some previous reports [293031]. Kim et al. reported a cohort of 510 GC patients in whom a preoperative BMI ≤ 18.5 kg/m2 was an independent prognostic factor for CSS in the stage I/II group (HR = 13.52; 95% CI, 1.19–154.20) [29]. Liu et al. [30] and Feng et al. [31] both reported that a low BMI was associated with poor OS in GC patients. Zhao et al. [32] performed a meta-analysis of 12 studies including 12,626 GC patients and demonstrated that 15.1% had a low BMI (< 18.5 kg/m2) and that those with a low BMI had a significantly lower survival rate than patients with normal BMI. However, some studies did not find a relationship between BMI and survival [3334]. Lee et al. [33] demonstrated that there was no significant difference in OS between the groups with low and normal preoperative BMI values (HR = 1.01; 95% CI, 0.72–1.40) in a study of 1,909 GC patients with a mean age of 58 yrs [31]. They found that patients with a low BMI had significantly lower OS than those with a high-normal BMI range (23.0 to 24.9). Interestingly, the subgroup analysis implied that the traditional BMI cutoff value is not as helpful as expected, and a better BMI cutoff value probably lies within the low-normal BMI range (18.5 to 22.9) [33]. Ejaz et al. [34] reported 775 GC patients in whom BMI was not related to CSS or OS, but patients who were underweight (BMI < 18.5 kg/m2) and had low albumin levels (< 35 g/L) had worse OS. However, researchers did not pay specific attention to elderly patients in these studies, and they used the low BMI cutoff value of 18.5 recommended by the World Health Organization.
BMI, which is an easily available index, is widely used as an indicator of nutrition in clinical practice, and a BMI < 18.5 kg/m2 is used as an indication of underweight or malnutrition. Clinical researchers noticed that elderly patients probably had different BMI classifications due to reduced metabolic status [35]. However, there is no consensus about the BMI cutoff values in elderly patients. The Dutch Malnutrition Steering Group (DMSG) defines a low BMI for patients over 65 yrs as less than 20 kg/m2 [36], and the European Society of Clinical Nutrition and Metabolism (ESPEN) recommends < 22 kg/m2 as one of the malnutrition criteria for patients ≥ 70 yrs [37]. These novel cutoff values were validated as predictors of short-term survival in the general hospitalized population [36]. In our study, we identified a BMI of 20.6 kg/m2 to classify patients into low BMI and high BMI groups as a novel cutoff value. Moreover, BMI ≤ 20.6 kg/m2 proved to be a significant independent risk factor for poor CSS in elderly GC patients after curative gastrectomy. This finding helped us to recognize that the novel BMI cutoff value, i.e., higher than 18.5, might be more suitable in elderly GC patients when evaluating their nutritional status, which is similar to the DMSG and ESPEN recommendations [3637]. Further studies with larger sample sizes may be needed in the future. Prospective studies in elderly GC patients are also warranted.
Studies have reported that nutritional status might be associated with surgical mortality in GC patients. Based on the NRS 2002 score, all elderly GC patients were at nutritional risk, which is associated with surgical outcomes [3839]. A PNI score < 45 might be a prognostic factor for survival in GC patients [4041]. Anemia and low levels of albumin and prealbumin were reported to be related to cancer survival after surgery separately or combined in a model [4243]. In our study, we found that weight loss ≥ 5%, NRS 2002 score ≥ 5, PNI score < 45, anemia, and low albumin and prealbumin levels were associated with CSS in the univariate analysis. However, none of these variables were independent risk factors in the multivariate analysis. One possible explanation would be associations between low BMI and them based on the methodology.
The CCI is associated with surgical outcomes, both in terms of postoperative morbidities and long-term survival, particularly in elderly patients [4445]. As a common tool used in geriatric units, a CCI score ≥ 3 was recently reported by Iwai et al. [46] to be associated with OS (HR = 7.88; 95% CI, 4.50–13.80) in elderly GC patients. However, we did not find similar results, although ICU admission was an independent risk factor. ICU admission often results from a high risk of cardiac and/or pulmonary dysfunction, which can be quite common in elderly patients with multiple comorbidities. In our study, we found that ICU admission was an independent predictor of CSS (HR = 1.97; 95% CI, 1.17–3.30), which could be related to complex comorbidities in elderly GC patients. Additionally, a higher pTNM stage indicated a poor CSS (stage II: HR = 5.56; 95% CI, 1.59–19.43; stage III: HR = 16.202; 95% CI, 4.99–52.59), which is widely recognized.
There are some limitations of the present study. First, this is a retrospective study with a relatively small sample size. Second, we did not collect data on surgical morbidity and quality of life, which are important in elderly GC patients. Third, patients may have other lifestyle exposures, such as alcohol use, that were unaccounted for in the study, and some patients may receive other forms of treatment. Moreover, the patients were from a single academic medical center in China, and caution should be exerted when extrapolating the results to various other populations. To the best of our knowledge, the BMI cutoff value of 20.6 kg/m2 is a novel finding, and a low BMI was determined to be an independent predictor of poor CSS in elderly GC patients. Future studies may examine the efficacy of the predictive value of these cutoff values for survival (20.6 vs. 18.5) in elderly surgical patients.
In conclusion, we found that a low BMI (≤ 20.6 kg/m2), postoperative ICU admission and advanced pathological TNM stages (II and III) were independent risk factors for CSS in elderly GC patients after gastrectomy. These findings may help optimally and efficiently evaluate and identify patients at high risk of poor outcomes. Survival in elderly GC patients could be improved by enhancing their nutritional status, treating their comorbidities and early diagnosis.
 XML Download
XML Download