

 PDF
PDF Citation
Citation Print
Print



Introduction
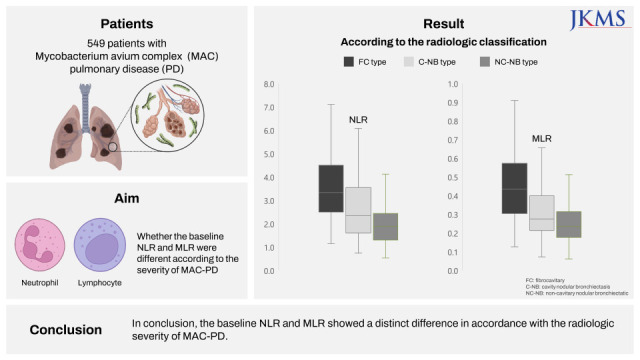
The neutrophil-lymphocyte ratio (NLR) and monocyte-lymphocyte ratio (MLR) are readily available laboratory markers calculated from a complete blood count (CBC). Previous studies have reported that both NLR and MLR were useful laboratory markers of the severity, treatment response, or recurrence of pulmonary or extrapulmonary tuberculosis.12345 Although the clinical characteristics of Mycobacterium avium complex (MAC)-pulmonary disease (PD) are similar to those of tuberculosis in many aspects, such as symptoms, radiologic findings, or treatment regimen,6 to date, no study has investigated the value of NLR and MLR in MAC-PD. Therefore, we aimed to assess this issue in patients with MAC-PD. Considering that, notably, NLR and MLR were associated with tuberculosis severity, we investigated whether the baseline NLR and MLR were different according to the severity of MAC-PD based on the radiologic classification.
Methods
Study subjects
Patients were enrolled in the Asan Medical Center in Seoul, South Korea. From 2001 to 2019, 1,148 patients with MAC-PD who had initiated treatment with a macrolide-containing regimen were identified. We excluded those 1) who did not undergo CBC examination within 90 days prior to treatment initiation (n = 384), 2) whose computed tomography (CT) findings were categorized as unclassifiable type (n = 150), and 3) who had comorbidities that could affect the results of white blood cell differential count, including liver disease (n = 24), infectious disease such as pneumonia (n = 21), were receiving calcineurin inhibitor (n = 7) or anti-cancer chemotherapy (n = 6), and others (n = 7). The medical records of the remaining patients were retrospectively analyzed in November 2021.
Radiologic classification and baseline NLR and MLR
Radiologic findings on chest CT were classified into one of the three major types: fibrocavitary (FC), cavitary nodular bronchiectatic (C-NB), and non-cavitary nodular bronchiectatic (NC-NB) types.7 The baseline NLR and MLR were compared according to each radiologic type. NLR and MLR were calculated from peripheral CBC. An automatic blood count device was employed for the analysis of CBC. NLR and MLR were determined as follows: NLR = Absolute Neutrophil Count/Absolute Lymphocyte Count, MLR = Absolute Monocyte Count/Absolute Lymphocyte Count.4
Statistical analysis
All data are presented as means ± standard deviation or as medians (interquartile range [IQR]) for continuous variables and number (%) for categorical variables. The baseline NLR and MLR values according to radiologic classification were compared using the Kruskal-Wallis test. For statistical analysis, an IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA) software was used.
Results
Study participants
The eligibility screening identified 549 patients with MAC-PD, including 95, 176, and 278 patients with FC, C-NB, and NC-NB types, respectively. Their median age was 64.0 (IQR, 56.0–72.0) years, and women were predominant (61.4%). The mean body mass index was 20.3 ± 2.9 kg/m2. Sputum acid-fast bacillus (AFB) smear positivity was noted in 49.0% of the patients. As shown in Table 1, a statistically significant difference was noted in terms of age, gender, body mass index, smoking history, etiologic organism, and sputum AFB smear positivity.
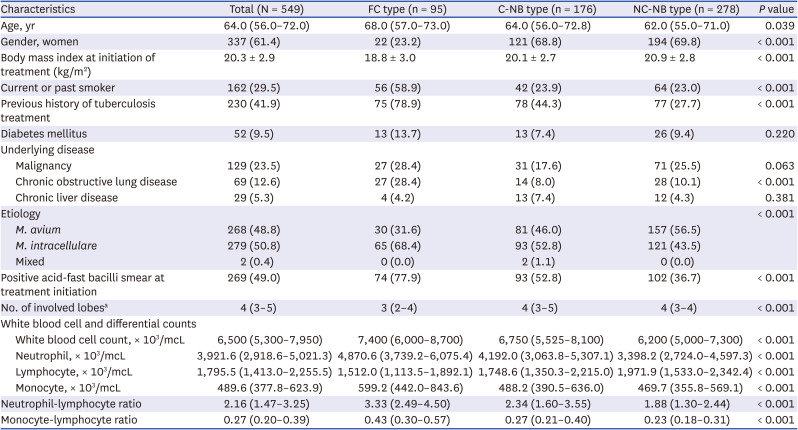
Table 1
Clinical characteristics of 549 patients with Mycobacterium avium complex pulmonary disease according to the radiologic classification
Data are presented as mean ± standard deviation, median (interquartile range), or frequencies (%).
FC = fibrocavitary, C-NB = cavitary nodular bronchiectatic, NC-NB = non-cavitary nodular bronchiectatic.
aThe extent of the involved lobe was assessed according to how many of the six lung lobes were involved, considering the lingular segment to be a separate lobe.
![]()
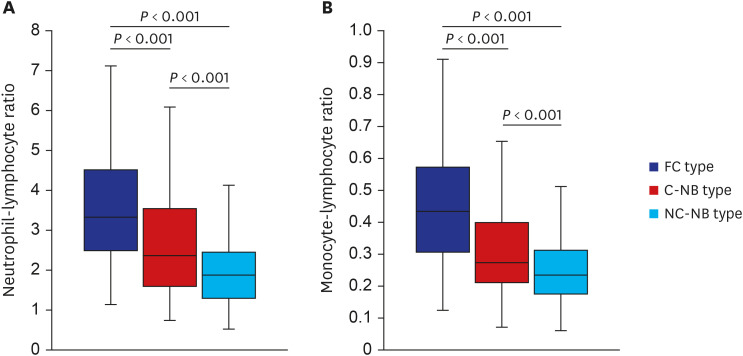
Baseline NLR and MLR according to radiologic classification
The baseline NLR of the 549 patients was 2.16 (IQR, 1.47–3.25). As shown in Fig. 1A, NLR was significantly higher in the FC type (3.33 [IQR, 2.49–4.50]), followed by that in the C-NB type (2.34 [IQR, 1.60–3.55]), and significantly lower in the NC-NB type (1.88 [IQR, 1.30–2.44]) (P < 0.001). In addition, the baseline MLR of the 549 patients was 0.27 (IQR, 0.20–0.39), and it was significantly higher in the FC type (0.43 [IQR, 0.30–0.57]), followed by that in the C-NB type (0.27 [IQR, 0.21–0.40]), and NC-NB type (0.23 [IQR, 0.18–0.31]) (P < 0.001), as shown in Fig. 1B.
Discussion
Although previous studies have shown that NLR and MLR are related to the treatment outcomes or severity of tuberculosis,1245 whether these two laboratory markers would also have a clinical value in MAC-PD has not been assessed, so far. This study investigated this aspect by retrospectively analyzing 549 patients with MAC-PD in a tertiary referral center in South Korea. We found a distinct difference in the baseline NLR and MLR according to the radiologic severity of MAC-PD; both NLR and MLR showed higher values when the radiologic findings of MAC-PD were more severe.
Radiologic classification has vital importance in MAC-PD regarding various aspects including the treatment regimen, outcome, and prognosis. In terms of drug regimen composition, an intermittent oral-drug therapy is recommended for patients with NC-NB type, whereas an aminoglycoside-containing daily regimen is recommended for those with cavitary type (i.e., FC and C-NB types).6 Notably, the treatment success rate for cavitary MAC-PD was reported to be significantly lower than that for NC-NB type despite receiving standard treatment.7 In addition, significant difference in the mortality rate was noted according to the radiologic type of MAC-PD. A recent study reported that the overall survival rates were higher in patients with NC-NB type than in those with a cavitary disease, and those patients with C-NB type showed mortality rates intermediate between those of NC-NB and FC forms.8
These clinical differences according to radiologic classification could be explained by cavitation, which indicates a higher mycobacterial burden in MAC-PD.9 Therefore, it can be predicted that the presence of cavity is accompanied by a severe overall inflammatory response. In general, the immune responses of circulating leukocytes to various inflammatory events are characterized by an increased number of neutrophils in the peripheral blood.10 In the case of tuberculosis, extensive neutrophilic response is a sign of severity and has been particularly related to tissue destruction.11 Neutrophilia is independently associated with a higher risk of cavity formation.12 Additionally, an increase in matrix metalloproteinase-8-expressing neutrophil was related to cavitation in tuberculosis.9 Moreover, monocytes are one of the essential components of the innate immune responses and act as a link to the adaptive immune system.4 Therefore, as the disease progresses, the number of monocytes derived from the hematopoietic stem cells could increase to phagocytize and restrict mycobacterium.13 An ongoing immune response against the cavitary lesion could result in further increase in the percentage of blood monocytes.141516 Moreover, lymphopenia could result from the accumulation of lymphocytes at the infection site, leading to their decreased number in the peripheral blood.17 These theoretical changes in neutrophils, lymphocytes, and monocytes can reasonably explain why NLR and MLR were increased in accordance with the radiologic severity in MAC-PD.
Only those patients who received treatment were included in this study. This is because patients with cavitary form MAC-PD without treatment are rarely encountered, as immediate treatment initiation is recommended for this type.18 When we performed the same analysis in patients with MAC-PD who did not receive treatment using the data of the patients enrolled in our previous study,19 we found a statistical difference in NLR and MLR between the cavitary vs. non-cavitary type (Supplementary Fig. 1). However, the number of patients with cavitary type was too small to analyze.
There may be other laboratory test results that can be related to the radiologic severity of MAC-PD including erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), or platelet count considering that previous studies have shown these inflammatory markers were associated with severity or the immune response of mycobacterial disease.202122 We compared the ESR, CRP, or platelet count according to the radiologic classification among a portion of patients in this study for whom these inflammatory markers were measured, the results of which are shown in Supplementary Fig. 2. As the Figure denotes, statistically significant differences in CRP and platelet count were noted among the three groups. Besides laboratory markers, the extent of radiologic involvement could also reflect the severity of MAC-PD. Additional analysis and results regarding whether the baseline NLR and MLR differ according to the number of involved lobes in each radiologic type, are summarized in Supplementary Fig. 3.
This study had some limitations; the most significant limitation being that it was conducted at a single referral center, and it had a retrospective design. Second, although NLR and MLR were measured in all the enrolled patients within 90 days of treatment initiation, the measured time points were slightly different for each patient. It was unclear whether the slightly different measurement time points for each patient affected the overall results of NLR and MLR. Finally, whether NLR and MLR could be used as a marker to predict treatment outcomes was not assessed. Further studies are needed to determine whether these values at baseline or during treatment are related to treatment outcomes in terms of treatment success or mortality.
In conclusion, this study showed that the baseline NLR and MLR had a distinct difference in accordance with the radiologic severity of MAC-PD.
 XML Download
XML Download