

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pneumonia is one of the most significant causes of mortality and morbidity worldwide.1 In South Korea, pneumonia ranked as the third most common cause of death in 2020.2 With an aging population, pneumonia continues to be a significant burden for the public healthcare system.3 In addition, since pneumonia can be fatal in the elderly, interest in its prevention and management has been continuous.4
Previous studies have reported the incidence of pneumonia in relation to drug use.5 Some have shown that certain frequently prescribed drugs, such as proton pump inhibitors and antipsychotics, increase pneumonia risk.567 However, some previous studies identifying the relationship between antihypertensive drug use and pneumonia prevention have shown inconsistent results.891011
A previous study using a nationwide database in South Korea reported that angiotensin receptor blocker (ARB) use is associated with reduced hospitalization for pneumonia in patients with stroke.12 Our study attempted to investigate the relationship between antihypertensive drug use and the incidence of pneumonia in the general population. As a secondary analysis, we attempted to validate the drug–disease relationship identified in the previous study through the subgroup analysis of a more diverse population.
METHODS
Study design, data source, and participants
This study used a case-crossover study design to assess the association of the usage and types of antihypertensive drugs with the incidence of pneumonia while minimizing the confounding factors derived from demographic characteristics. This study was performed using data from the Korea National Health Insurance Service–National Sample Cohort (NHIS-NSC) database, which includes 2.2% of the total eligible Korean population from 2002 to 2015.13 The database contains individual medical information, such as diagnosis, prescribed medications, and hospitalization history, without personal identification. The diagnoses recorded in this cohort database were based on the International Classification of Diseases, 10th Revision (ICD-10). We extracted the data of those diagnosed with and hospitalized for pneumonia. All the enrolled participants in this study had a pneumonia event (cases), and each case served as its own control.
Variables included in this study
The primary endpoint of this study was hospitalization for pneumonia, which was defined as ICD-10 codes J12–18. We included the index date of the first-onset pneumonia from 2002 to 2015 to account for recurrent pneumonia.
The antihypertensive drug types were divided into 3 subgroups: angiotensin-converting-enzyme (ACE) inhibitors, ARBs, and other antihypertensive drugs. Patients with combination drugs including ACE inhibitors were categorized into the ACE inhibitor subgroup. Similarly, patients with combination drugs including ARBs were categorized into the ARB subgroup.
Statistical analysis
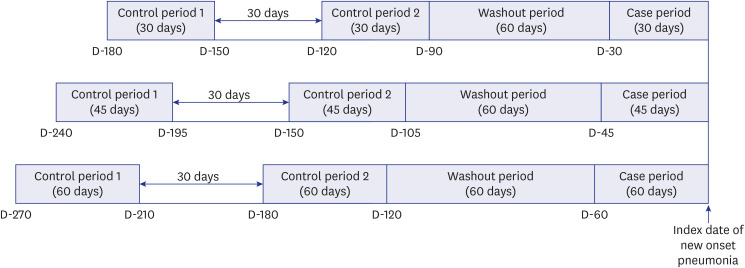
Categorical variables were expressed as frequencies and proportions. Our primary analysis was the comparison of each individual’s drug exposure period (30 days before the incidence of pneumonia, which was defined as the case period) to two control periods, each lasting 30 days (90–120 and 150–180 days before pneumonia onset) (Fig. 1). For the subgroup analyses, comparison were made according to exposure to other medications, such as statins, antipsychotics, and benzodiazepine, as well as by the number of outpatient clinic visits. We performed further subgroup analyses according to the presence of diabetes mellitus, documented disability, and whether the participants were aged ≥ 70 years. Finally, to verify the robustness of the primary results, we performed sensitivity analyses by modifying the case and control periods (Fig. 2). To adjust for confounding factors, the participants’ characteristics were included in the analyses. The entire medication list utilized in this study is available in Supplementary Data 1. Conditional logistic regression analysis was performed to determine the association between drug usage and pneumonia risk. For each model, we adjusted determinants such as ACE inhibitors, ARBs, other antihypertensives, statins, antipsychotics, benzodiazepine, and the number of outpatient visits. All statistical analyses were performed using the SAS system for Windows (SAS Institute Inc., Cary, NC, USA).
Fig. 1
The case-crossover study design. Case period was defined as a 30-day window before the index date of new-onset pneumonia. Two control periods were each defined as a 30-day window in a 30-day interval. A 60-day washout period was set between the end of the last control period and the start of the case period.

RESULTS
Baseline characteristics
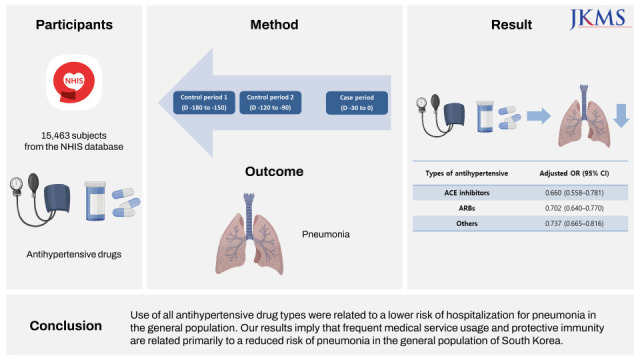
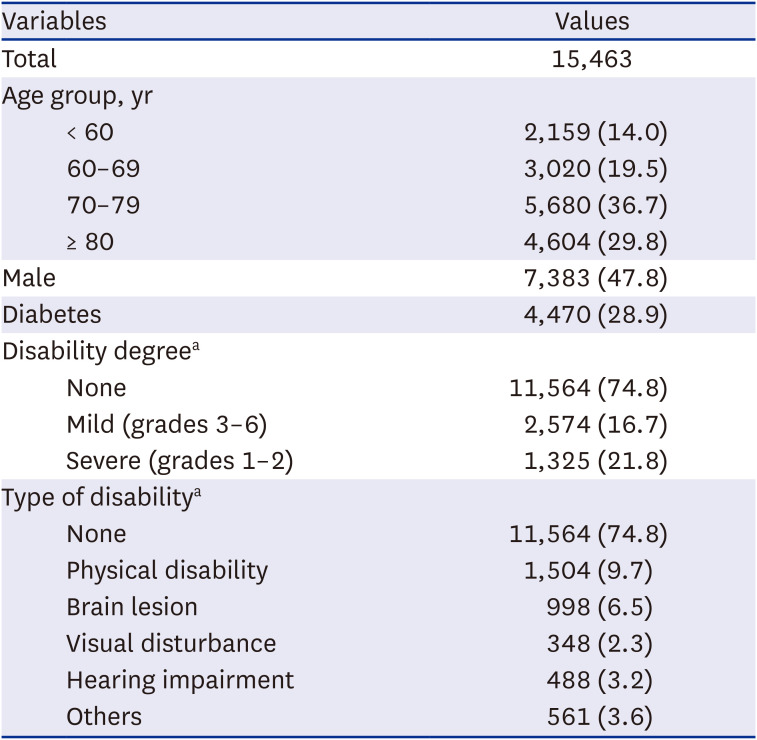
Of 15,463 patients included in the final cohort, 7,383 (47.8%) were male, 10,284 (66.5%) were aged ≥ 70 years, 4,470 (28.9%) had diabetes mellitus, and 3,899 (38.4%) had a disability (Table 1). According to medicine usage, 1,183 (7.7%), 5,030 (32.53%), and 3,647 (23.6%) received ACE inhibitors, ARBs, and other antihypertensive drugs, respectively (Supplementary Table 1).
Table 1
Baseline characteristics
Risk of hospitalization for pneumonia
The use of ACE inhibitors (adjusted odds ratio [aOR], 0.660; 95% confidence interval [CI], 0.558–0.781), ARBs (aOR, 0.702; 95% CI, 0.640–0.770), and other antihypertensive drugs (aOR, 0.737; 95% CI, 0.665–0.816) were significantly associated with a reduced risk of pneumonia (Table 2). The sensitivity analyses revealed similar results (Supplementary Table 2).
Table 2
Association between antihypertensive use and pneumonia risk

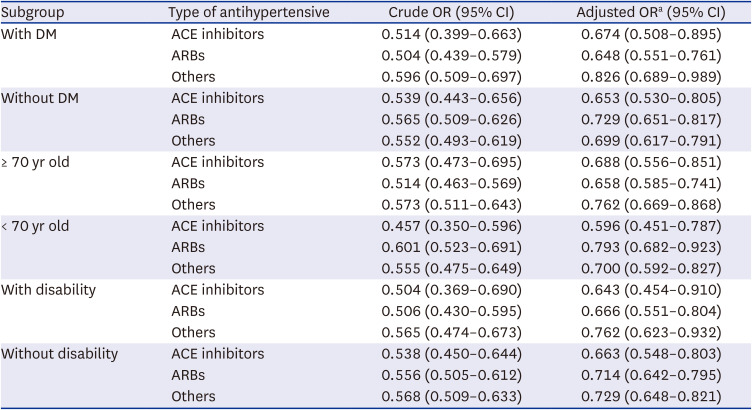
In the subgroup analyses, the use of antihypertensive drugs significantly reduced the incidence of pneumonia regardless of the presence of diabetes mellitus or disability and whether the participants were aged ≥ 70 years (Table 3).
Table 3
Association between antihypertensive use and pneumonia risk by subgroup
Among other determinants in the logistic regression models, antipsychotics significantly increased the risk of pneumonia (aOR, 1.346; 95% CI, 1.160–1.562). On the other hand, more frequent outpatient visits significantly decreased the risk of hospitalization for pneumonia (aOR, 0.884; 95% CI, 0.878–0.891) and consistently decreased this risk in all subgroups. Odds ratios for other determinants and their sensitivity analyses results are shown in Supplementary Tables 3 and 4, respectively.
DISCUSSION
This was the first study to identify the association between antihypertensive drug usage and pneumonia prevention in the general population, using data from the Korean NHIS-NSC database. This study demonstrated that antihypertensive drug usage was related to a lower risk of hospitalization for pneumonia in the general population of South Korea. The results were consistent regardless of the type of antihypertensive drug used, the presence of diabetes mellitus or disability, or old age.
The preventive effects of ACE inhibitors or ARBs on the incidence of pneumonia are not consistent in previous studies.1415 Our results confirmed that these drugs lowered the risk of pneumonia. Several mechanisms may explain these results. The findings of previous studies, including clinical trials, suggest that renin-angiotensin system (RAS) blockers—ACE inhibitors and ARBs— may reduce the risk of pneumonia or show a protective effect on the pulmonary function of specific populations, including older adults; or patients with stroke, neurodegenerative diseases, or chronic obstructive pulmonary diseases; and Asians.161718 ACE inhibitors work by downregulating intrarenal RAS activation.1920 Its main mechanism is to disturb the conversion of angiotensin I to angiotensin II. Dry cough, its major side effect, is attributed to the inhibitory mechanism of bradykinin and substance P degradation.2122 The swallowing reflex, which may be regulated by substance p, is an important defensive mechanism preventing aspiration of oropharyngeal contents into the respiratory system.2324 Further, as a complementary action, increased bradykinin and substance P levels can prevent asymptomatic aspiration and improve the coughing reflex.2526 Thus, ACE inhibitors may be implicated in the stimulation of the swallowing reflex. Lastly, angiotensin II promotes cellular immune response by activating lymphocytes in animals and humans.2728 Thus, ACE inhibitors are tasked to reduce the risk of pneumonia and other extrapulmonary inflammations.29
In contrast, several studies show no association between either ACE inhibitors or ARBs and the risk of pneumonia.830 A case-crossover study using data from the Taiwan Longitudinal Health Insurance database found that neither the use nor cumulative dose of ACE inhibitors or ARBs are associated with the risk of pneumonia among the general population of Taiwan.31
This discrepancy may be due to various outcome definitions, racial differences, geographic and climate factors, or specific healthcare systems in each country studied. Our outcome definition, particularly that of pneumonia hospitalization, did not include all types of pneumonia. In a study on patients with stroke, ARB use is associated with reduced pneumonia hospitalization.12 Therefore, the difference in the target group may have contributed to the difference in the results.
We confirmed that other antihypertensives—other than ACE inhibitors and ARBs—also reduced the risk of pneumonia in the general population. The relationship between the use of other antihypertensives and the risk of pneumonia was rarely studied, and the mechanism of reduced pneumonia incidence due to these medications has also not been elucidated. We inferred that these results eventually determined the risk of pneumonia according to medical use and accessibility. That is, the higher the number of outpatient clinic visits, the more likely the receipt of medical care, and thus the lower the risk of pneumonia. Our logistic regression models consistently showed that frequent outpatient clinic visits lowered the risk of pneumonia regardless of the subgroup. As such, after being diagnosed with hypertension, patients must visit medical facilities more regularly to potentially lower their risk of pneumonia, allowing for the early detection and management of respiratory symptoms or administration of influenza and pneumococcal vaccines.
Furthermore, we can infer that the different results between patients with stroke and the general population are attributed to the various mechanisms of pneumonia development. In the general population, community-acquired pneumonia is common. In stroke patients, the estimated proportion of aspiration or hospital-acquired pneumonia cases is relatively high. Community- and hospital-acquired pneumonia have different main pathogens.3233 Pathogens of community-acquired pneumonia, such as Streptococcus pneumoniae or Haemophilus influenza, are highly affected by vaccination and herd immunity.34 Therefore, a lowered risk of pneumonia in the general population may result from an immunity preventive effect on a main pathogen rather than the impact of a specific antihypertensive drug.35
In addition, we included the subgroup analyses to illuminate the effect of the variables on various groups. Older adults with medical comorbidities had an increased incidence of community- and hospital-acquired pneumonia.3637 In older adults and people with disabilities, swallowing dysfunction is a risk factors for pneumonia.3839 Previous studies have suggested that the swallowing function significantly changes with age due to decreased oropharyngeal skeletal muscle strength and reduced peristalsis, which requires multiple swallowing.4041 Diabetes mellitus is a risk factor for pneumonia hospitalization and is associated with other infectious diseases.4243 Our results confirmed that antihypertensive drugs were universally effective in preventing pneumonia regardless of the subgroup.
Finally, we simultaneously investigated other medications as covariates to determine their effects on pneumonia hospitalization. Antipsychotics showed an increased risk of pneumonia hospitalization in the total patient group. Previous studies have also suggested an association between antipsychotics and pneumonia risk.4445 These findings are primarily explained by dysphagia and secretion; antipsychotics can promote oropharyngeal dysphagia, which may be associated with an extrapyramidal adverse effect or a related anticholinergic reaction.46
This study had several limitations. First, we included pneumonia cases that required hospitalization. Therefore, this study excluded some atypical or community-acquired pneumonia cases that can be treated in an outpatient clinic. Second, given the observational feature of this study design, we cannot suggest a precise mechanism to explain the association between antihypertensive use and pneumonia prevention. Third, this study design cannot eliminate confounding factors that change over time, such as increasing medication compliance, changes in the frequency of outpatient visit, or changes in personal interest in health. Finally, due to the limitation of our database, we cannot consider seasonal variation, which is one of the vital factors in pneumonia risk.
In conclusion, the use of all antihypertensives were associated with a reduced risk of pneumonia hospitalization in the general population of South Korea. Our results were consistent with that of the previous reports and further suggested that frequent medical service usage and protective immunity were primarily related to a reduced risk of pneumonia in the general population of South Korea.
 XML Download
XML Download