

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since 1983, when the cause of death statistics started to be published, cancer has been reported as the leading cause of death in Korea, making it the country’s major public health concern.1 In 2018, over 240,000 patients were newly diagnosed with cancer in Korea, and more than one-fourth of all-cause mortality cases resulted from cancer.2 Supported by a national policy on cancer prevention and screening in Korea, the incidence rate of cancer peaked in 2011 and gradually declined subsequently. The overall cancer mortality rate has also steadily decreased since 2002 owing to diagnostic and treatment modality advances. In 2018, liver, pancreatic, and biliary tract cancers were the 6th (6.5% of all new cancers), 8th (3.1%), and 9th (2.9%) most common cancers in Korea, respectively. However, when the incidence rates of all hepatobiliary and pancreatic (HBP) cancers were added, they comprise 12.5%, which is higher than that of stomach cancer (12.0%), the most common cancer in Korea. With the availability of vaccination and effective treatment for viral hepatitis, especially hepatitis B, the incidence of hepatocellular carcinoma (HCC) is decreasing; in contrast, the incidence rates of pancreatic and biliary tract cancers are rapidly increasing, and liver and pancreatic cancers ranked 2nd and 5th in the most common causes of cancer-related death in 2018.234567 Unfortunately, considering the relatively small number of patients with each type of HBP cancers, liver, pancreatic, and biliary tract cancers have not been prioritized in the national health policy, despite being fatal. Although studies from our institution have reported short-term future predictions of cancer incidence and mortality in Korea annually, no studies have focused on future cancer burdens regarding long-term changes in the incidence and mortality rates of HBP cancers.89 Moreover, although the cancer registration system in Korea is highly efficient in providing nationwide cancer statistics, a lag time of at least two years is required for data collection and analysis in a specific year.1011 In planning and implementing comprehensive cancer control programs, the number of new cases and deaths that are expected to occur in the future should be estimated. Therefore, this study aimed to analyze the current trends and predict the epidemiologic features of liver, pancreatic, and biliary tract cancers according to the Korea Central Cancer Registry data. The findings of this study could provide useful insights into health policy planning and budget allocation, including cancer prevention, diagnostic and treatment strategies.
METHODS
Data collection
The Korean Ministry of Health and Welfare initiated the Korea Central Cancer Registry (KCCR), a nationwide, hospital-based cancer registry, in 1980. Since 1999, the KCCR has collected cancer incidence data countrywide by integrating a nationwide hospital-based KCCR database with data from regional cancer registries. The KCCR built the Korea National Cancer Incidence Database (KNCI DB), which collects data from hospitals, 11 population-based registries, and additional medical record reviews since 2005. They have been providing the nationwide cancer incidence, survival, and prevalence statistics annually.12 This database contains information on age; sex; region; diagnosis; date; primary cancer site; histological type; most valid diagnostic method; summary stage of surveillance, epidemiology, and end results program (since 2005); and first treatment course within 4 months after diagnosis.
In this study, we obtained cancer incidence data from 1999–2017 from the KNCI DB. Cancer cases were classified according to the International Classification of Diseases for Oncology (ICD-O), third edition, and converted according to the International Classification of Diseases, 10th edition (ICD-10).1314 We also collected cancer mortality data from 2002–2018 from Statistics Korea.1 The cause of death was coded and classified according to ICD-10.14 We obtained the estimated population from 1999–2040 from Statistics Korea as well.
Cancer sites were categorized as follows: liver (C22.0, C22.9), gallbladder (GB) (C23), Intra- and extrahepatic bile duct (bile duct [BD]; IBD and EBD, respectively) (C22.1, C24.0, C24.8, C24.9), ampulla of Vater (AoV) (C24.1), and pancreas (C25).
Ethical statement
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki, as reflected in a prior approval obtained from the institutional ethical committee (Institutional Review Board, National Cancer Center, Korea [NCC2020-0093]), Written informed consent from the participants was waived because of the retrospective design of the study.
Statistical analysis
Rates were expressed as crude rate (CR) and age-standardized rates (ASR) per 100,000 individuals. The CR was calculated as the total number of incidence (crude incidence rate [CIR]) or mortality (crude mortality rate [CMR]) cases divided by the midyear population of the specified years. ASRs were standardized using the registered population of year 2000 and expressed per 100,000 persons; the incidence rate ratio using ASRs was also calculated.15 Based on the CIR and the age-standardized incidence rate (ASIR), which were calculated until 2017, the prediction was made for 2018–2040. Conversely, the CMR and age-standardized mortality rate (ASMR) were calculated until 2018, and a forecast was made for 2019–2040.
Incidence and mortality were modeled using an age-period-cohort model and extrapolated to 2040. The age-period-cohort model was as follows:
where λ represents the incidence (mortality) rate according to age and calendar period; g is the “link” function; and fA, fP, and fC represent the functions of age, period (year of incidence or mortality), and cohort (year of birth, i.e., cohort = period–age), respectively.16 We used the exponential function as the link function, and fA, fP, and fC as natural cubic splines.
We used the “apcspline” Stata ado-program to conduct annual percentage change (APC) modeling, with a default setting for internal knots for the spline (6 for age variable, 5 for period variable, and 3 for cohort variable).
When modeling using the spline, we absorbed the linear trends in period and cohort over the timespan with observed data into a drift component and attenuated the drift into the future. A function was developed in Stata to fit the model to the incidence/mortality of cancer in the individual (from 1999 to 2017 in incidence, 2002 to 2018 in mortality) and 5-year age groups (0–4, 5–9, …, 74–79, 80+) by sex. To estimate age-specific cancer rates in future years, an APC model was fitted to age-specific rates for the 5-year age groups against their respective years, and the projected age-specific rates were multiplied by the age-specific population to obtain the projected number of cancer cases and deaths for the upcoming years. To adjust the future demographic structure, we employed an estimated population by Statistics Korea to calculate the ASIR and ASMR. Linear regression models were used on logarithmic scaled ASRs and calendar years to identify time points with significant trend changes and to calculate the APC for each segment between these time points.17 The joinpoint regression analysis describes changes in data trends by connecting several different line segments on a log scale at “joinpoints,” which was performed to detect when significant changes occurred in cancer trends according to sex and cancer site. The linear regression model was applied to ASRs by 5-year age groups against their respective years, based on the observed cancer incidence data of the latest trends to predict ASRs.
Moreover, APC, which is the average percentage change of ASRs, is calculated as follows:

where log(Ry) = b0 + b1y × year
Log(Ry) is the natural log-transformed ASR.17
The weighted average of APCs was the average APC (AAPC) with 95% confidence intervals for the whole period of interest.18 We also performed a pairwise comparison, and tested the differences between sexes. All statistical tests were two-tailed, and P values < 0.05 were considered statistically significant. Incidence and trends were analyzed using SAS 9.4 (SAS Institute, Inc., Cary, NC, USA), Joinpoint 4.7.0.0 (National Cancer Institute, Bethesda, MD, USA), and Stata version 16.1 (StataCorp LP, College Station, TX, USA).
RESULTS
Incidence and mortality rates of liver, pancreatic, and biliary tract cancers in Korea from 1999 to 2017, and from 2002 to 2018
From 1999 to 2017, HBP cancer cases had been increasing in number continuously. Compared with HCC, which showed a relatively slow increase of new cases GB, BD, AoV, and pancreatic cancers had increased for approximately 2–3 times within the same period. In ASIR analysis, the ASIRs of liver and GB cancers decreased, whereas those of BD and pancreatic cancer increased (Table 1). Supplementary Table 1 shows the trend of annual cancer incidence cases among HBP cancers.

Table 1
Annual cases and age-standardized rates of hepatobiliary and pancreatic cancer
![]()
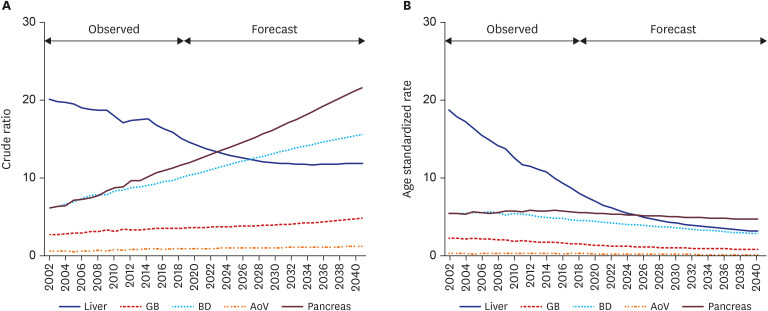
During the same period, trends in the ASIR of each cancer were as follows: 25.8 to 13.5 in liver cancer (AAPC −3.6%; P < 0.001), 2.9 to 2.6 in GB cancer (AAPC −0.5%; P = 0.171), 5.1 to 5.9 in BD cancer (AAPC 1.1%; P = 0.084), 0.9 to 0.9 in AoV cancer (AAPC −0.6%; P = 0.217), and 5.6 to 7.3 in pancreatic cancer (AAPC 1.5%; P < 0.001). The APC of ASIR in liver and pancreatic cancers was statistically significant (Table 2). In the subgroup analysis, the trends of change of ASIRs were similar between both sexes; APC of the liver was significantly low and that of the BD and pancreas was significantly high (Supplementary Table 2). In particular, the APC of ASIR in pancreatic cancer was significantly higher in females than in males (2.4% vs. 0.8%, P < 0.001).
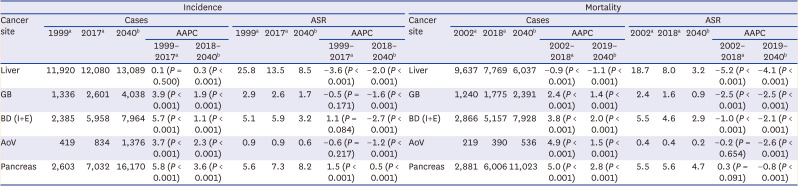
Table 2
Incidence and mortality cases and age-standardized rates of hepatobiliary and pancreatic cancers up to 2040
ASR = age-standardized rates, AAPC = average annual percent change, GB = gallbladder, BD (I+E) = bile duct (intrahepatic+extrahepatic), AoV = ampulla of vater.
aObserved values; bEstimated values.
![]()
From 2002 to 2018, the ASMR of each cancer decreased, except for pancreatic cancer (18.7 to 8.0 in liver [AAPC −5.2%; P < 0.001], 2.4 to 1.6 in GB [AAPC −2.5%; P < 0.001], 5.5 to 4.6 in IBD and EBD [AAPC −1.0%; P < 0.001], 0.4 to 0.4 in AoV [AAPC −0.2%; P = 0.654], and 5.5 to 5.6 in pancreatic [AAPC 0.3%; P = 0.091]) cancers per 100,000 persons. Thus, except for pancreatic cancer, the APC of all ASMRs in other HBP cancers was negative (Table 2). In the subgroup analysis, the trends of change of ASMRs in liver, GB, and BD cancers were decreasing, similar to those in males and females. The ASMR in pancreatic cancer had been decreased in males but increased in females. Meanwhile, the ASMR in AoV cancer showed no significant difference in the past in both sexes (Supplementary Table 2).
Predicting future epidemiology of liver, pancreatic, and biliary tract cancer in Korea by 2040
Predicted annual cases of newly diagnosed cancer from 2018 to 2040 increased in all cancer types as follows: 12,157 to 13,089 (liver), 2,681 to 4,038 (GB), 6,304 to 7,964 (IBD and EBD), 844 to 1,376 (AoV), and 7,459 to 16,170 (pancreas) (Fig. 1). The CIR of pancreatic cancer is predicted to increase more rapidly than those of other cancers (Fig. 2A). Meanwhile, the predicted ASIR increased in pancreatic cancer (7.5 to 8.2 [AAPC 0.5%; P < 0.001]) but decreased in all other cancers (13.2 to 8.5 in liver [AAPC −2.0%; P < 0.001], 2.5 to 1.7 in GB [AAPC −1.6%; P < 0.001], 5.9 to 3.2 in IBD and EBD [AAPC −2.7%; P < 0.001], and 0.8 to 0.6 in AoV [AAPC −1.2%; P < 0.001]) (Table 2, Fig. 2B). Both sexes were predicted to have similar increasing trends of CIR (Supplementary Fig. 1A and B). In subgroup analysis in both sexes, the predicted ASIR of pancreatic cancer increased only in females (6.2 to 7.9 [AAPC 1.1%; P < 0.001] vs.8.6 to 8.5 [AAPC −0.1%; P < 0.001]). Meanwhile, the predicted ASIR in GB, IBD/EBD, and AoV cancers decreased slightly in both males and females. Moreover, the ASIR of liver cancer decreased more rapidly in males (21.8 to 12.5 [AAPC −2,5%; P < 0.001] than in females (5.3 to 4.5 [AAPC −0.8%; P < 0.001]) (Supplementary Table 3, Supplementary Fig. 1C and D).
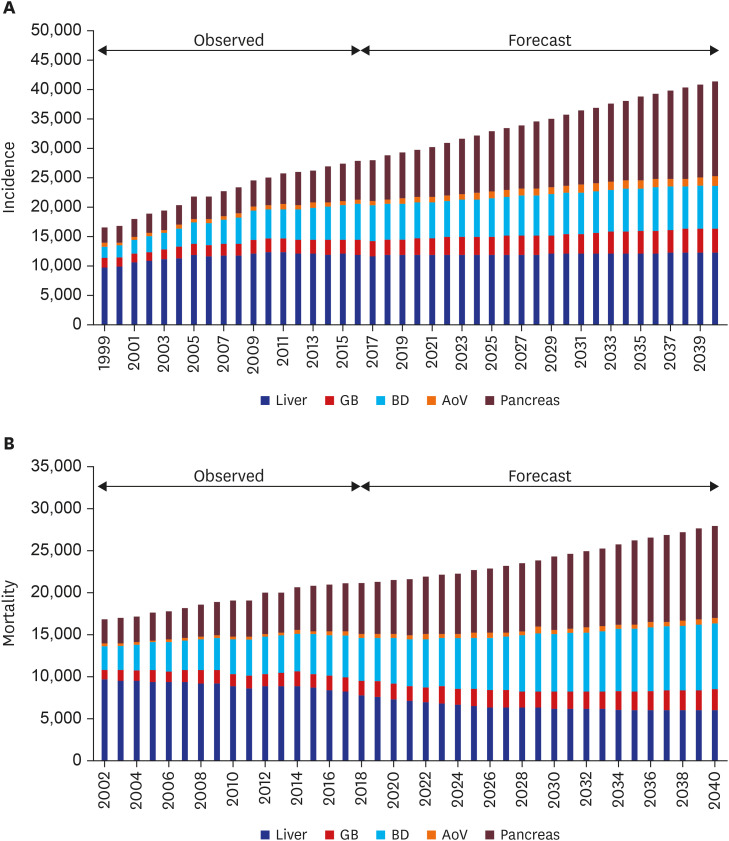
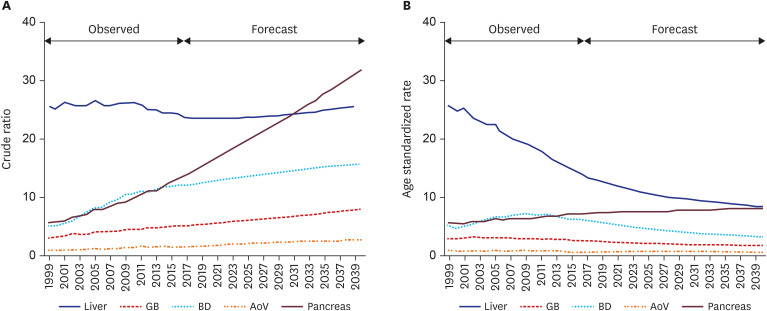
Fig. 1
Trends in the number of cases of hepatobiliary and pancreatic cancers in the Korean population. (A) Incidence. (B) Mortality.
GB = gallbladder, BD = bile duct, AoV = ampulla of Vater.
![]()
Fig. 2
Trends and future prediction of incidence rates of hepatobiliary and pancreatic cancers in the Korean population. (A) Trends and projected mortality crude rates for incidence. (B) Trends and projected age-standardized rates for incidence.
GB = gallbladder, BD = bile duct, AoV = ampulla of Vater.
![]()
Furthermore, the predicted annual deaths from 2019 to 2040 decreased in liver cancer (7,551 to 6,037) but increased in other cancers (GB, 1,795 to 2,391; IBD and EBD, 5,313 to 7,928; AoV, 397 to 536; pancreas, 6,202 to 11,023). CMRs are predicted to increase markedly in pancreatic and BD cancers but decrease in liver cancer (Fig. 3A). However, the predicted ASMR decreased in all cancer types (7.5 to 3.2 in liver [AAPC −4.0%; P < 0.001], 1.5 to 0.9 in GB [AAPC −2.4%; P < 0.001], 4.5 to 2.9 in IBD and EBD [AAPC −2.1%; P < 0.001], 0.3 to 0.2 in AoV [AAPC −2.6%; P < 0.001], and 5.6 to 4.7 in pancreatic cancer [AAPC −0.8%; P < 0.001]) (Fig. 3B). Pancreatic cancer was predicted to be the leading cause of cancer-related death among HBP cancers. Similar CMR trends are expected in both sexes. Although CMR in liver cancer was predicted to be still higher in males than in females, it was predicted to decrease more markedly in males (22.8 to 18.7) than in females (6.4 to 5.1). Meanwhile, CMR in pancreatic cancer was predicted to increase more markedly (P < 0.001, data not shown) in females (12.1 to 25.1) than in males (11.8 to 18.2) (Supplementary Fig. 2A and B). The ASMR of pancreatic cancer was also predicted to increase in females (4.8 to 4.9) (P < 0.001) but decrease in males (6.3 to 4.5) (P < 0.001) (Supplementary Table 3). Furthermore, the ASMR (4.9) of pancreatic cancer in females in 2040 were predicted to be the highest among all HBP cancers (liver, 1.1; GB, 0.9; BD,1.7; AoV, 0.1). Moreover, the ASMR of the liver (12.9 to 5.4 [AAPC −4.1%; P < 0.001]) was still expected to be the highest in males in 2040 (GB, 0.9; BD, 4.2; AoV, 0.3; pancreas, 4.5). However, the predicted ASMR of other HBP cancers was decreased (P < 0.001) (Supplementary Table 3, Supplementary Fig. 2C and D).
DISCUSSION
Changes in cancer incidence and mortality may vary depending on the geography, race, sex, and age; hence establishing a nationwide healthcare policy is required to identify the epidemiologic features of cancer and predict its future according to the gathered data.21920 In Korea, a national policy on cancer prevention and screening revealed that the incidence of all types of cancers peaked in 2011 and then declined. The overall mortality rate of cancers has also started to decline since 2002, owing to advances in diagnostic and treatment modalities. However, these trends of cancer do not represent the trend of each cancer. In this study, we specifically assessed the epidemiological changes of HBP cancers (GB, IBD/EBD, liver, AoV, and pancreatic cancers). Results showed that the number of new HBP cancer cases had increased from 1999 to 2017 and predicted to continuously increase by 2040. In liver cancer, the incidence and mortality rates had decreased from 2011 and 2002, and the projected CIR, CMR, ASIR, and ASMR were predicted to dramatically decrease by 2040. In other HBP cancers, especially pancreatic cancer, the incidence had increased, and the CIR and ASIR were predicted to increase. The CMR and ASMR in pancreatic cancer were also predicted to decrease but slightly, and eventually, this type would become the leading cancer in HBP cancer mortality by 2040.
Rahib et al.21 predicted that pancreatic and liver cancers would surpass breast, prostate, and colorectal cancers, becoming the second and third leading causes of cancer-related death by 2030 in the United States. In a recently published report in Korea, pancreas is predicted to become one of the five leading cancer sites causing mortality in both sexes in 2021.22 Our study showed that pancreatic cancer incidence has been increasing gradually since 1999. Although the ASMR of pancreatic cancer is expected to slightly decrease in the future, it is expected to increase in females and pancreas will be the leading site of HBP cancer mortality by 2030–2040. The increase in predicted mortality of pancreatic cancer may result from the lack of effective treatment and difficulty in making early diagnosis despite the increased incidence. Surgery is the only potentially curative option for pancreatic cancer, but less than 20% of patients are eligible for this treatment. In addition, treatments for metastatic pancreatic cancer are minimally effective.232425 Therefore, strategies for early detection and therapeutic targets that can be translated and tested in clinical trials should be identified as early as possible in preparation for the expected increase of pancreatic cancer cases in the next 10–20 years. Of note, an extensive process is required to validate an early detection biomarker for clinical use, and approximately 7.9 years is needed for clinical testing and approval of a new cancer therapy.2627
Especially, the increasing trend of incidence and mortality in pancreatic cancer were observed and predicted more clearly in females than in males. Although the increase in females’ social activities and smoking and drinking rates may be the cause, the smoking and drinking rates only increased slightly, and these rates remain considerably higher in males than females.28 Therefore, these results are difficult to interpret, and additional research is needed to explain these different trends between sexes.
In contrast, the incidence and mortality rates of liver cancer were predicted to decrease more dominantly in males than females. This dramatic decrease may be derived from vaccination for chronic hepatitis B virus (HBV) as a national policy. Approximately 80% of all primary liver cancers are diagnosed as HCC, and the most important cause of HCC in Korea is HBV infection.29 According to the results of a random selection registry study of the Korean Liver Cancer Association and the KCCR, 62.2% and 10.4% of patients diagnosed with HCC between 2008 and 2010 had HBV and hepatitis C virus, respectively; the remaining 27.4% was considered unknown but was presumed to be liver cirrhosis caused by alcoholic and/or nonalcoholic fatty liver disease.3031 Since 1983, HBV vaccination has been recommended for all neonates in Korea. The percentage of vaccinated infants has surpassed 98.9% since 1990, and the HBsAg carrier rate in the general population decreased to 3.7% in 2007. In particular, HBsAg prevalence decreased to 0.44% in teenagers and 0.2% in children below 10 years old.32 Aside from vaccination, advances in medical, interventional, and surgical treatment for liver disease can contribute to reduced HCC mortality.33343536
As shown in our study results, the incidence and mortality rates of HBP cancers continue to change. Future predictions analyzed at a particular point of time must be interpreted. As cancer incidence and mortality increase, medical costs also increase; thus, researchers, including clinicians, need to regularly conduct epidemiologic analysis and prediction for efficient budgeting.3738 Based on the accumulated results, improved national cancer policies will be established and implemented in the future.
The annual rates of HBP cancer incidence and mortality are expected to increase in the future. However, those of liver cancer are decreasing and will further decrease, especially in males. In contrast, those of pancreatic cancer have been increasing and will continue to increase, becoming the most frequent and leading cause of cancer-related death among HBP cancers. Therefore, more HBP specialists and improvement in health policy are needed in preparation for such situation.
 XML Download
XML Download