

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) first emerged in China in late 2019.1 Since the World Health Organization (WHO) has declared a pandemic for coronavirus disease 2019 (COVID-19) in March 2020, there have been 509 million confirmed cases and 6.2 million cases of death caused by COVID-19 as of April 2022.2 Vaccination is a key strategy for controlling the COVID-19 pandemic, and several vaccines have been developed and approved for emergency use. However, as the COVID-19 pandemic continues for a long time, antibody levels might decline over time.3 Furthermore, as SARS-CoV-2 variants have emerged, there have been concerns regarding the decreased effectiveness of these vaccines against wild-type (WT) SARS-CoV-2.45
Protection against SARS-CoV-2 infection is associated with humoral and cellular immune responses. The presence of abundant neutralizing antibodies (nAbs) is crucial for protection against SARS-CoV-2 infection; however, cellular immunity is also important, particularly for the severe disease prevention. There is accumulating evidence that T cell immunity against SARS-CoV-2 is long-lasting and cross-reactive to SARS-CoV-2 variants, despite the rapid decrease of neutralizing antibody levels within 6 months.678
Ad26.COV2.S is a Janssen-manufactured COVID-19 vaccine, which comprises a recombinant, replication-incompetent human adenovirus type 26 (Ad26) vector encoding a SARS-CoV-2 spike (S) protein.9 In the recently published final analysis of the phase III ENSEMBLE trial, a single dose of Ad26.COV2.S provided 56.3% and 52.9% protection against moderate-to-severe critical COVID-19 for at least 14 and 28 days after administration, respectively. In addition, the overall vaccine efficacy against SARS-CoV-2 variants (except for the Omicron variant) was 43.8% and 44.4% at least 14 and 28 days after administration, respectively. There was no significant difference in serious adverse events (AEs) between the vaccine and placebo groups in the final analysis, although one case of vaccine-induced immune thrombotic thrombocytopenia was documented in a 25-year-old man in the vaccine group.10 In South Korea, Ad26.COV2.S has been used for priming or booster vaccination in adults aged ≥ 18 years, and as of April 2022, 1.5 million people have been vaccinated with Ad26.COV2.S in South Korea.11
However, data on the immunogenicity of Ad26.COV2.S is insufficient, and only 10 of the 805 participants were Asians in the phase I/IIa trial of this vaccine.9 Immunogenicity and reactogenicity data from diverse populations are important to establish effective vaccination strategies. Therefore, we conducted a prospective cohort study to evaluate the immunogenicity of Ad26.COV2.S in the Korean population. This study aimed to evaluate antibody kinetics (anti-S immunoglobulin [Ig] G and neutralizing antibody [NAb]) and T-cell response (up to 12 weeks after vaccination) with Ad26.COV2.S. Cross-reactive immune responses against the B.1.617.2 lineage (Delta variant) and lineage B.1.1.529 (Omicron variant) SARS-CoV-2 were also evaluated.
METHODS
Study design and procedures
This prospective cohort study was conducted from June 2021 to January 2022 at the Korea University Guro Hospital and Ajou University Hospital in South Korea. Healthy adults aged ≥ 19 years without medical comorbidities, without a history of COVID-19, without a history of vaccination against COVID-19, and scheduled to be vaccinated with Ad26.COV2.S (Janssen, 5 × 1010 viral particles) were included. Those who had a history of autoimmune diseases or immunocompromising conditions were excluded in this study. Demographic data (age, sex, height, weight, medical comorbidities, history of COVID-19 vaccination, and history of COVID-19) were collected at baseline. Blood samples were collected before vaccination (baseline), at 3–4 weeks, 5–8 weeks, and 10–12 weeks after vaccination to evaluate the longitudinal immunogenicity of Ad26.COV2.S (Fig. 1). Data on solicited local and systemic AEs were collected using a questionnaire on the seventh day after vaccination. The incidence, severity, and duration of AEs were also investigated. Serious and unsolicited AEs were recorded during the study period.

Immuogenicity analysis
Elecsys SARS-CoV-2 spike immunoassay (Roche) was performed to measure anti-S IgG antibodies using a Cobas 8000 (Roche Diagnostics, Switzerland) according to the manufacturer’s protocol. Anti-N antibodies were measured in each participant using the SARS-CoV-2 IgG assay (Abbott Laboratories, Chicago, IL, USA) to exclude preceding SARS-CoV-2 infection.
For the NAbs analysis, a plaque reduction neutralization test (PRNT) was performed using WT SARS-CoV-2 (hCoV/Korea/KCDC03/2020), B.1.617.2 lineage (hCoV-19/Korea/KDCA229079/2021), and lineage B.1.1.529 (hCoV-19/Korea/KDCA447321/2021). The mixture of serum dilution/virus (40 PFU/well) was incubated at 37°C for 2 hours, and added to the plate seeded with Vero E6 cells and incubated at 37°C for 1 hour, followed by the addition of 0.5% agarose (Lonza, Basel, Switzerland). After 2–3 days of incubation, the cells were fixed with 4% paraformaldehyde and stained to visualize the plaques. A reduction in plaque count of 50% (PRNT50) was then calculated for the median neutralizing titer (ND50) using the Spearman–Karber formula and ND50 ≥ 1:20 was considered positive.
IFN-γ enzyme-linked immunosorbent spot (ELISpot) assay was performed to quantify SARS-CoV-2 specific T-cell immune responses in peripheral blood mononuclear cells (PBMCs) from vaccinated individuals. ELISpot plates (Human IFN-γ ELISpotPRO kit, MABTECH, Sweden) were blocked by RPMI medium 1640 (Gibco, NY, USA) containing 10% fetal bovine serum (FBS, Gibco) and 1% penicillin/streptomycin (p/s, Gibco). After washing, the plates were added with 2 μg/well of SARS-CoV-2 Spike (ID: P0DTC2) peptide pools (GenScript, Piscataway, NJ, USA) and 3 × 105 cells/well of PBMCs. Stimulation with DMSO or PMA/Ionomycin was as negative and positive controls, respectively. The plates were then processed following the manufacturer’s protocol and median spot forming units (SFUs) were counted on the ELISpot reader. The results are presented as SFU per million input PBMC (SFU/106 PBMC).
Statistical analysis
Data are expressed as the mean with a 95% confidence interval (CI) or median with an interquartile range. The Wilcoxon signed-rank test was performed to compare paired data. Statistical analysis was performed using the Statistical Package for the Social Sciences version 20 (SPSS Inc., Chicago, IL, USA) or GraphPad Prism software (version 5.0; GraphPad Software, Inc., San Diego, CA, USA). Statistical significance was set at P < 0.05.
Ethics statement
The study was approved by the ethics committees of Korea University Guro Hospital (2021GR0099) and Ajou University Hospital (AJIRB-BMR-SMP-21-267), and was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Written informed consent was obtained from all participants.
RESULTS
Study participants
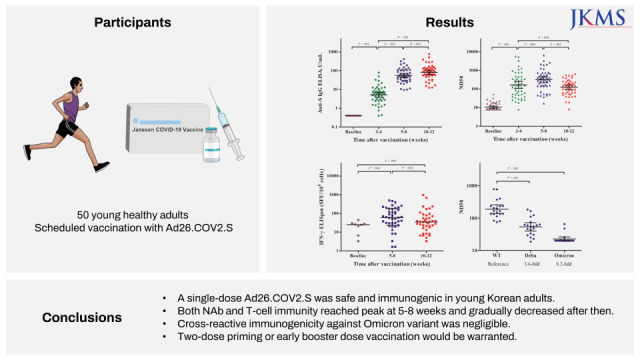
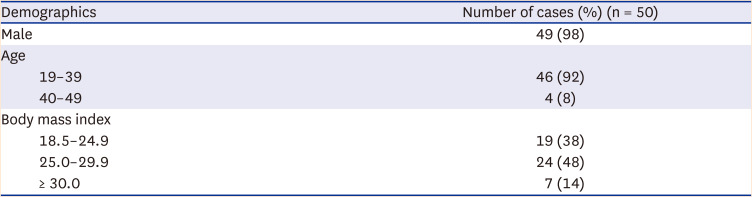
A total of 52 participants were included in the cohort, but two participants withdrew consent during follow-up. Among the 50 participants eligible for the analysis, 92% (n = 46) were aged 19–39 years and 8% (n = 4) were 40–49 years old. Most of the participants (98%, n = 49) were men with mean body mass index of 26.8 kg/m2 (Table 1). We measured IgG anti-N antibodies to assess the natural SARS-CoV-2 infection history; all participants showed negative anti-N antibodies using enzyme-linked immunosorbent assay. All participants completed a follow-up visit until 5–8 weeks after vaccination, but two of them did not at 10–12 weeks.
Humoral immune response
The baseline geometric mean titer (GMT) of anti-S IgG of all participants was 0.4 U/mL and was considered non-reactive. The GMT of anti-S IgG was 5.2 ± 3.0 U/mL at 3–4 weeks, 55.7 ± 2.4 U/mL at 5–8 weeks, and 81.3 ± 2.5 U/mL at 10–12 weeks after vaccination (Supplementary Table 1). The GMT of anti-S IgG significantly increased over the study periods (3–4, 5–8, and 10–12 weeks after vaccination; P < 0.001) (Fig. 2). Anti-S IgG was positive in 94% (47/50) of participants at 3–4 weeks, and increased to 100% at 5–8 and 10–12 weeks after vaccination.
Fig. 2
Immunogenicity after Ad26.COV2.S vaccination. (A) Titer of anti-Spike (S) anti-SARS-CoV-2 spike protein IgG, (B) 50% neutralization dose (ND50), (C) median of S-specific T-cell responses measured by IFN-γ ELISpot assay. The black bar represents geometric mean titer with 95% confidence intervals.
ELISA = enzyme-linked immunosorbent assay, IgG = immunoglobulin G, SFU = spot forming unit, IFN-γ = interferon-γ, ELISpot = enzyme-linked immuneSpot.
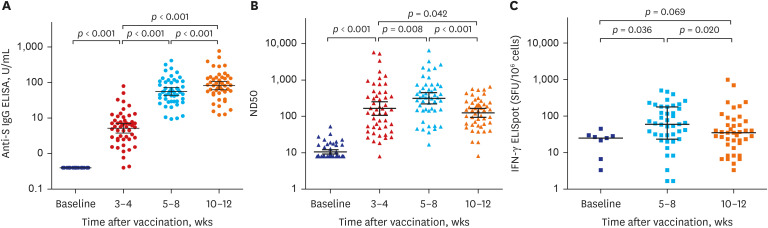
Regarding NAbs, the GMT of ND50 against WT SARS-CoV-2 was 10.6 ± 1.6, 164.6 ± 4.6, 313.9 ± 3.6, and 124.4 ± 2.6 at baseline, at 3–4 weeks, at 5–8 weeks and at 10–12 weeks after vaccination, respectively (Supplementary Table 1). The GMT of ND50 was highest at 5–8 weeks and was significantly attenuated by 2.5-fold at 10–12 weeks (P < 0.002) (Fig. 2). NAb against WT SARS-CoV-2 was detected in 96% (48/50) of the participants at 3–4 weeks, 98% (49/50) at 5–8 weeks, and 93.8% (45/48) at 10–12 weeks after vaccination.
SARS-CoV-2-specific T cell response
The IFN-γ ELISpot assay was performed to evaluate T-cell responses to SARS-CoV-2 S protein at baseline (nine participants), 5–8 weeks (43 participants), and 10–12 weeks (44 participants) after vaccination. The proportions of positive responders were 88.9%, 97.7%, and 97.7%, with a median number of spot-forming units (SFU) per 100,000 cells of 25.0 (95% CI, 5.0–29.2), 60.0 (95% CI, 23.3–178.3), and 35.0 (95% CI, 13.3–71.7) at pre-vaccination, at 5–8 weeks and at 10–12 weeks after vaccination, respectively (Supplementary Table 1). The S protein-specific T cell response peaked at 5–8 weeks and decreased at 10–12 weeks (P = 0.020) (Fig. 2).
Cross-reactive immunogenicity against variants of concern
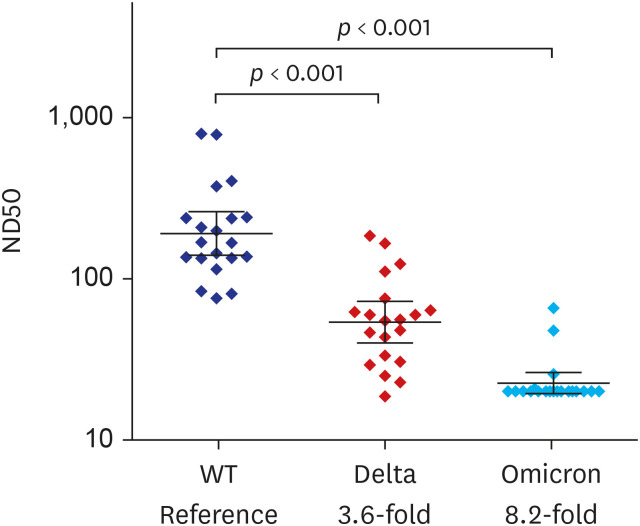
Neutralization assays were conducted against SARS-CoV-2 WT and variants of concern (VOCs, B.1.617.2 lineage [Delta] and lineage B.1.1.529 [Omicron]) in randomly selected participants (n = 20) 8 weeks after vaccination with Ad26.COV2.S. The GMTs of ND50 against SARS-CoV-2 WT and VOC are shown in Fig. 3. The reactivity rate of neutralizing antibody assays was 100% (20/20) for WT, 95% (19/20) for Delta, and 15% (3/20) for Omicron. The GMTs of ND50 against VOCs were significantly lower than that against WT [(WT vs. Delta vs. Omicron; 181.0 ± 1.9 vs. 50.9 ± 1.9 vs. 22.2 ± 1.4, respectively (P < 0.001)]. Compared to the WT, cross-neutralizing activity was significantly attenuated by 3.6-fold against Delta and 8.2-fold against Omicron.
Adverse events
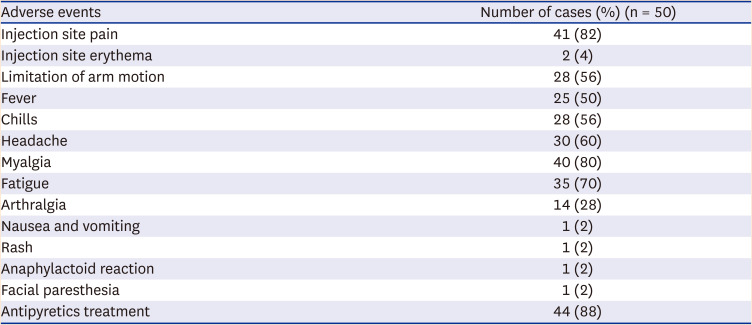
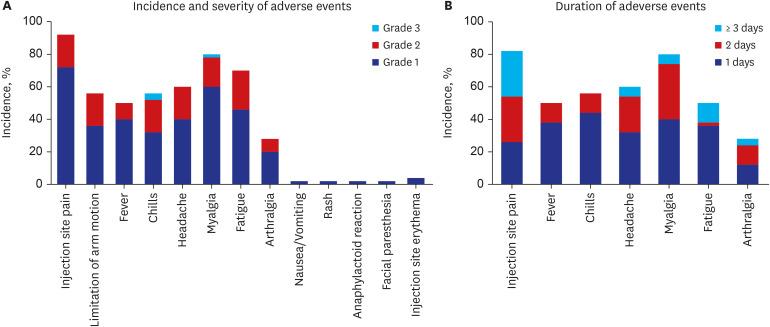
The reactogenicity of Ad26.COV2.S is shown in Table 2 and Fig. 4. The most common AEs were injection site pain (82%), myalgia (80%), fatigue (70%), headache (60%), chills (56%), limitation of arm motion (56%), and fever (50%). The frequency, severity, and duration of solicited AEs after Ad26.COV2.S are described in Supplementary Table 2. Most AEs were grade 1–2 with resolution within 2 days, but three cases of grade 3 AE were observed (two cases of chills and one of myalgia). There were no unsolicited AEs and grade 4 AEs during the study period.
Table 2
Reactogenicities at seventh day after vaccination with Ad26.COV2.S
DISCUSSION
In this prospective cohort study including Ad26.COV2.S recipients, we found that the seropositive rate of IgG anti-S antibody was 94% at 3–4 weeks after single-dose Ad26.COV2.S immunization and the antibody titer further increased by 12 weeks; NAb titer against WT SARS-CoV-2 was highest at 5-8 weeks after vaccination but decreased by 2.5-fold at 10–12 weeks; NAb titers against Delta and Omicron variants were attenuated by 3.6- and 8.2-fold compared to the WT SARS-CoV-2, respectively; S-specific T-cell immune response peaked at 5–8 weeks and decreased at 10–12 weeks; although injection site pain and myalgia were quite common, Ad26.COV2.S was well tolerated.
In phase I/IIa trial, a single shot of Ad26.COV2.S demonstrated acceptable immunogenicity and safety profiles.912 Consistent with our results, the GMT of IgG anti-S antibody peaked at 8 weeks after vaccination with Ad26.COV2.S (5 × 1010 viral particles), and approximately 100% seroconversion was observed at 4 weeks post-vaccination in young adults aged 18–55 years.912 The GMTs of NAb increased by 10 weeks, forming a plateau over the next-coming 2–4 weeks in a clinical trial.912 In comparison, the GMTs of NAb reached a peak at 5–8 weeks after vaccination with Ad26.COV2.S and gradually decreased thereafter in this study.9 Moreover, as reported for another adenovirus-vectored COVID-19 vaccine, ChAdOx1, single-dose adenovirus-vectored COVID-19 might induce insufficient memory B-cell response.13 Therefore, further studies are required to evaluate longevity in diverse populations despite previous studies reporting that humoral and cellular immunity is induced by Ad26.COV2.S persisted for up to 8 months.14 This study on the immunogenicity and reactogenicity of Ad26.COV2.S may be helpful in this context.
When analyzing cross-reactive immunogenicity for VOCs, NAb titers against Delta and Omicron variants were decreased by 3.6-fold and 8.2-fold, respectively, compared to the WT SARS-CoV-2. In particular, neutralizing activity against the Omicron variant was negligible. Cross-reactive neutralization activity is crucial for the prevention of SARS-CoV-2 infection, and to enhance cross-reactive neutralizing activity, sufficient memory B-cells must be produced by vaccination, and affinity maturation of memory B-cells is essential.68 These issues may be overcome to some extent using optimal booster vaccination strategies. In Ad26.COV2.S-primed recipients, heterologous mRNA vaccine boosting showed markedly enhanced neutralizing activity and a durable T-cell immune response comparable to homologous 2-dose mRNA vaccine immunization.1516
The strength of this study is that we provide unique and important data on the immunogenicity and safety of Ad26.COV2.S in the Korean population. Given that a low proportion of Asian participants were included in the previous clinical trials, our data could provide useful information on the immunogenicity and safety of Ad26.COV2.S in Asian populations. In addition, we evaluated cross-reactive immunogenicity against important VOCs using a neutralization assay.
This study had some limitations. First, the majority of participants were young men under 50 years of age. In accordance with the policy of the Korean government, Ad26.COV2.S was primarily assigned to military reservists aged 30–60 years. Immune responses can vary according to age, sex, race, and ethnicity. In the phase I/IIa trial of Ad26.COV2.S, cohort 1 (18–55 years old) showed robust immune responses compared to cohort 3 (≥ 65 years old).9 Second, the difference between Ad26.COV2.S and other platform vaccines was not directly compared in terms of immunogenicity and reactogenicity.
In conclusion, a single-dose Ad26.COV2.S vaccine is safe and immunogenic in young Korean adults. Both NAb and T cell immunity peak at 5–8 weeks and gradually decrease thereafter. The cross-reactive immunogenicity against the Omicron variant was negligible. The single-dose Ad26.COV2.S vaccination may not induce long-lasting protective immunity. Thus, two-dose priming or early booster dose vaccination would be warranted.
 XML Download
XML Download