

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
As the coronavirus disease 2019 (COVID-19) infection spreads around the world, each country was reporting many excess deaths. Excess deaths were defined as any death that exceeds the expected number of deaths based on the number of deaths over the past several years.12 During the COVID-19 pandemic, there are several reports regarding excess death that does not directly associate with COVID-19 infection because of lock-down and stay-at-home campaign. It has been known that the fear of contagion during the COVID-19 pandemic creates time delays with subsequent impact on mortality in patients with acute myocardial infarction (AMI).3 However, difference of time delay and clinical outcome in patients with ST-segment elevation myocardial infarction (STEMI) or non-STEMI between pre-pandemic and pandemic era has not been fully investigated yet in Korea. Therefore, the aim of this study was to investigate the impact of COVID-19 pandemic on time delay and clinical outcome in patients with STEMI or non-STEMI.
METHODS
Study design and patient population
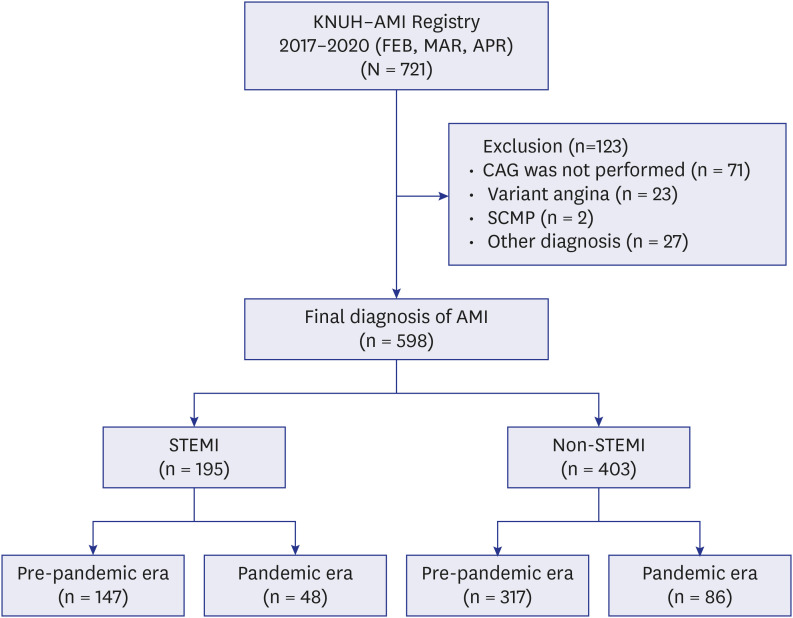
This observational study included 721 consecutive patients who were diagnosed with AMI at admission during pre-pandemic era (February, March, April 2017, 2018, and 2019) and COVID-19 pandemic era (February, March, April 2020). Patients who were registered in the Kyungpook National University Hospital—AMI registry within the study period were enrolled in this study. AMI was diagnosed based on the presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia. STEMI and non-STEMI were defined according to fourth universal definition of myocardial infarction.4 Study flow diagram was shown in Fig. 1. Of these, patients who did not receive coronary angiography (n = 71) or were diagnosed with variant angina (n = 23), stress induced cardiomyopathy (n = 2), or other diagnoses (n = 27) were excluded. Baseline characteristics of the patients who did not receive coronary angiography are shown in Supplementary Table 1. Finally, 598 patients who underwent coronary angiography in the pre-pandemic and pandemic era with same diagnosis during the same period were analyzed in this study. Among them, 195 patients were diagnosed as STEMI at pre-pandemic (n = 147) and pandemic era (n = 48), whereas 403 patients were diagnosed as non-STEMI at pre-pandemic (n = 317) and pandemic era (n = 86), respectively.
Clinical assessment
Baseline demographic and clinical characteristics including age, sex, cardiovascular risk factors such as hypertension, diabetes mellitus, hyperlipidemia, and current smoking, and presenting characteristics were collected at the time of admission. Electrocardiogram was recorded and analyzed by attending cardiologists. Left ventricular ejection fraction was assessed by two-D echocardiography prior to hospital discharge. Venous blood samples were obtained at the time of admission. All patients’ data and procedural details were collected at the time of admission. All patients’ medications were collected during hospitalization.
Definition of time variables
Transfer time in hospital was defined as transfer time from emergency room (ER) to catheterization laboratory. Symptom-to-door time was defined as the time from symptom onset to ER arrival in our hospital. Door-to-balloon time was defined as the time of ER arrival to the first passage of an intracoronary device.567
Clinical outcomes
The primary outcomes were the incidence of time delay, cardiac arrest, and in-hospital mortality. During the follow-up period, clinical outcome data were obtained by reviewing medical records and interviewing patients by telephone.
Statistical analyses
Data were expressed as mean ± standard deviation for continuous variables and as percentages for categorical variables. Comparisons between baseline variables were assessed using Student’s t-test for continuous variables and Pearson’s χ2 test for categorical variables. Normality test was performed for all continuous variables. Analyses were conducted to compare eras (pre-pandemic versus pandemic) and were stratified based on presentation (non-STEMI or STEMI). The cumulative incidence rates of cardiac arrest and in-hospital death between pre-pandemic and pandemic eras were estimated by Kaplan-Meier curve using the log-rank test. For all analyses, a 2-sided P value < 0.05 was considered statistically significant. Statistical analysis was performed using the Statistical Package for the Social Sciences, version 20.0 (IBM Corp., Armonk, NY, USA).
RESULTS
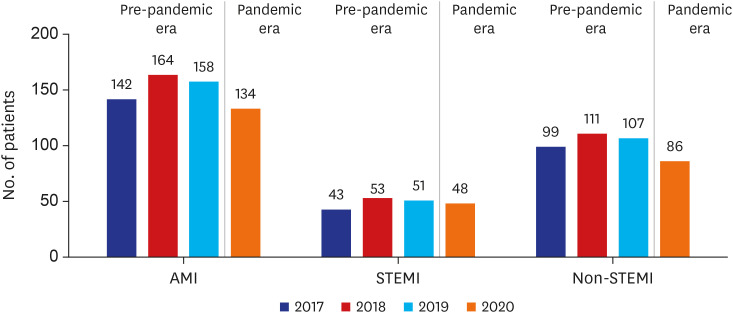
During the pandemic era, there was 13.5% reduction in the number of patients hospitalized with AMI compared with pre-pandemic era, which was mainly driven by 18.8% reduction in non-STEMI (Fig. 2).
Baseline characteristics are presented in Table 1. There were no significant differences in demographic characteristic including age, sex, body mass index between pre-pandemic and pandemic era both STEMI and non-STEMI. In initial presentation, systolic (P = 0.002) and diastolic blood pressure (P = 0.003) was significantly lower in the pre-pandemic era compared with those of pandemic era in STEMI, but not in non-STEMI. Among cardiovascular risk factors, dyslipidemia (P = 0.008) was significantly higher during pandemic era compared with pre-pandemic era in non-STEMI. There were no significant differences of prevalence of other cardiovascular risk factors hypertension, diabetes mellitus, previous ischemic heart disease, chronic kidney disease, and current smoking between pre-pandemic and pandemic era both STEMI and non-STEMI.8 Left ventricular ejection fraction (P = 0.069) was lower during pandemic era in non-STEMI, but not in STEMI. Among laboratory findings, low-density lipoprotein cholesterol level was significantly lower during pandemic era compared with pre-pandemic era in STEMI. There were no significant differences in the serum levels of hemoglobin, glucose, hemoglobin A1c, lipid profiles, and creatinine between two eras in both STEMI and non-STEMI. Among medications, the use of P2Y12 inhibitors were lower in the pre-pandemic era, whereas the use of angiotensin converting enzyme inhibitors/angiotensin type 2 receptor blockers (ACE-I/ARBs) were lower during pandemic era in both STEMI and non-STEMI.
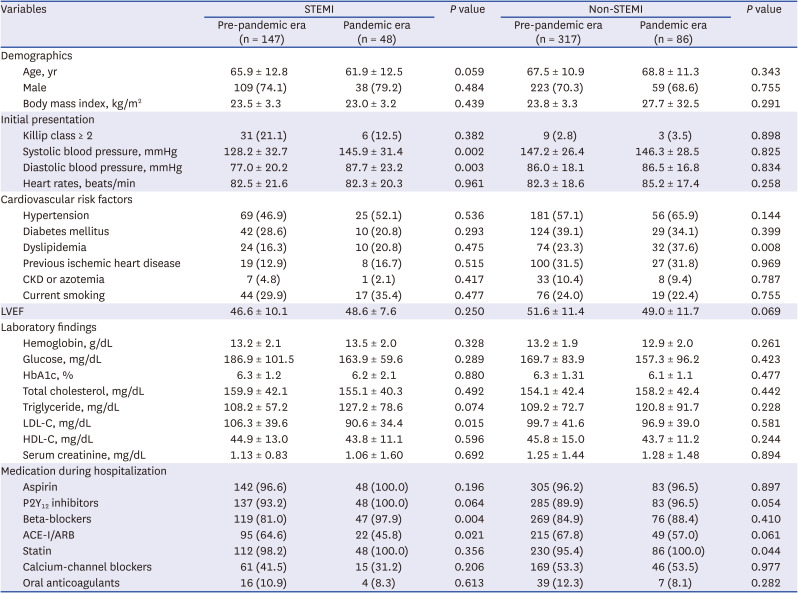
Table 1
Baseline characteristics of study subjects
Data are expressed as mean ± standard deviation or number (percent).
STEMI = ST-segment elevation myocardial infarction, CKD = chronic kidney disease, LVEF = left ventricular ejection fraction, HbA1c = hemoglobin A1c, LDL-C = low-density lipoprotein cholesterol, HDL-C = high-density lipoprotein cholesterol, ACE-I = angiotensin converting enzyme inhibitor, ARB = angiotensinogen type 2 receptor blocker.
![]()
Angiographic and procedural characteristics are presented in Table 2. In patients with STEMI, there were no significant differences in diseases vessel, multivessel disease, treated vessel, pre thrombolysis in myocardial infarction flow, fluoroscopy time procedure time, frequency of angioplasty, and the number of stents between pre-pandemic and pandemic era. The amount of contrast was significantly higher during pandemic era compared to that of pre-pandemic era (P = 0.002). In patients with non-STEMI, left main coronary artery diseases was significantly higher during the pandemic era compared with pre-pandemic era (P = 0.037). Accordingly, percutaneous coronary intervention of left main coronary artery disease was performed more frequently during pandemic era compared with pre-pandemic era (P = 0.032).
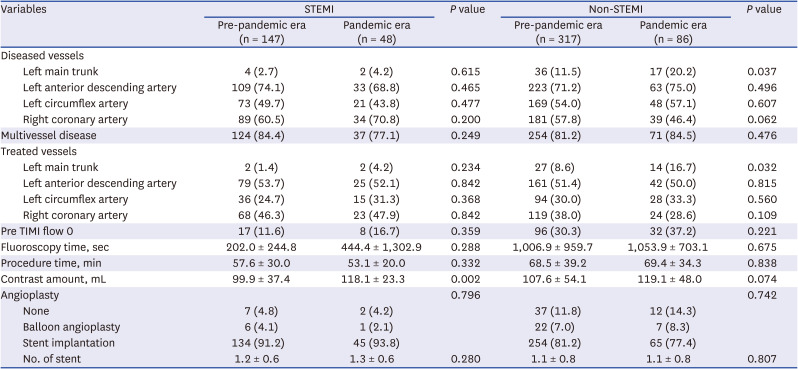
Table 2
Angiographic and procedural characteristics in study subjects
Data are expressed as mean ± standard deviation or number (percent).
STEMI = ST-segment elevation myocardial infarction, TIMI = thrombolysis in myocardial infarction.
![]()
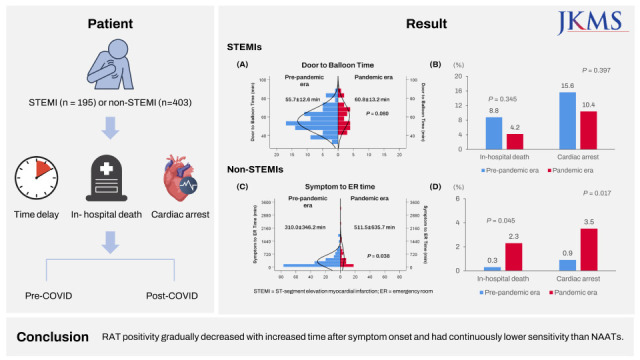
Time variables related to logistics of care of AMI are presented in Table 3. Time distribution of symptom to ER time, ER to catheterization lab arrival time, and door to balloon time between pre-pandemic and pandemic era in both STEMI and non-STEMI are shown in Supplementary Fig. 1. In patients with STEMI, there was no significant difference in symptom to ER time, symptom to catheterization lab arrival time, symptom to balloon time, and ER to catheterization lab time between pre-pandemic and pandemic era. Door to balloon time was shorter in the pre-pandemic era compared with pandemic era (P = 0.080). In patients with non-STEMI, symptom to ER time was significantly longer during the pandemic compared with pre-pandemic era (P = 0.038). Patients who arrived ER within 360 minutes (72.7% vs. 57.1%, P = 0.040) and within 720 minutes (87.6% vs. 75.5%, P = 0.040) were significantly higher in the pre-pandemic era compared with pandemic era in non-STEMI, but not in STEMI (Fig. 3).
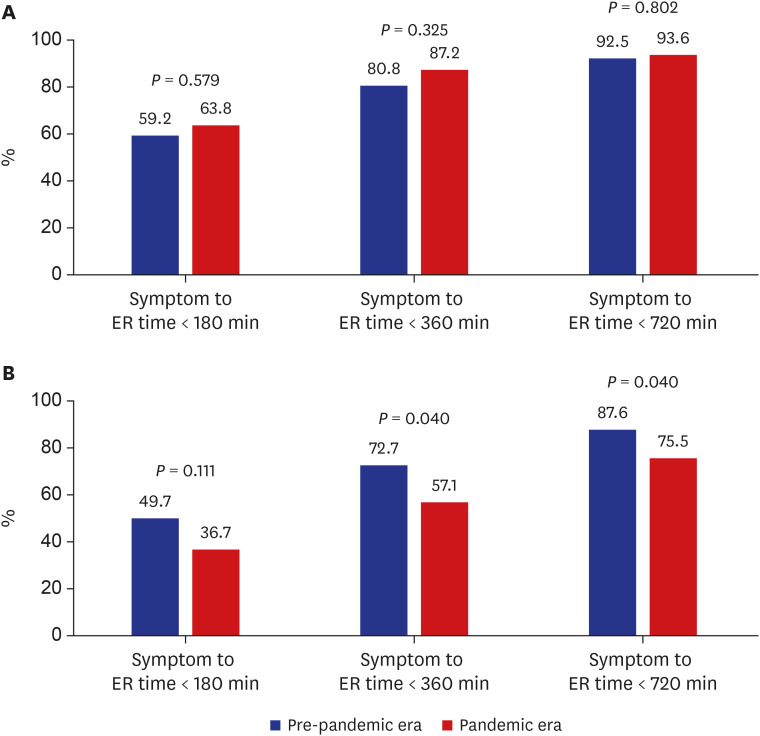

Fig. 3
Comparison of patient delay in (A) ST-segment elevation myocardial infarction and (B) non-ST-segment elevation myocardial infarction between pre-pandemic and pandemic era.
ER = emergency room.
![]()
Table 3
Time variables in study subjects
Data are expressed as mean ± standard deviation or number (percent).
STEMI = ST-segment elevation myocardial infarction, ER = emergency room, cath = catheterization, lab = laboratory.
aNon-parametric test.
![]()
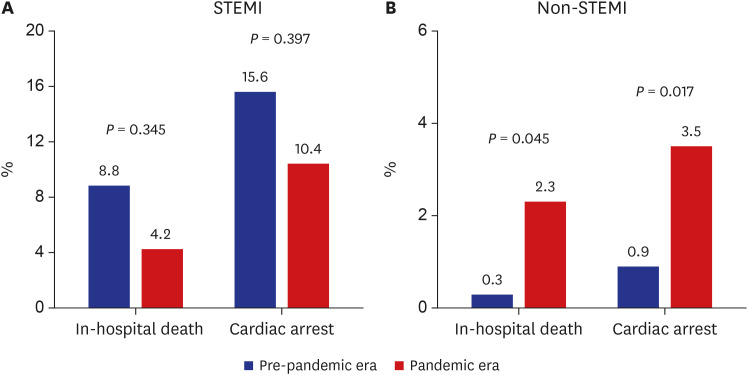
In patients with STEMI, there were no significant differences in in-hospital death (8.8% vs. 4.2%, P = 0.345) and cardiac arrest (15.6% vs. 10.4%, P = 0.397) between pre-pandemic and pandemic era (Fig. 4). In patients with non-STEMI, in-hospital death (2.3% vs. 0.3%, P = 0.045) and cardiac arrest (3.5% vs. 0.9%, P = 0.017) were significantly higher during pandemic era compared with pre-pandemic era.
DISCUSSION
The main findings of this observational study are as follows. First, the number of patients who were admitted with a suspicion of AMI were decreased during the pandemic. Second, there were considerable time delays including system delay in STEMI and patient delay in non-STEMI during the pandemic. Third, the incidence of in-hospital death and cardiac arrest was significantly higher during the pandemic in non-STEMI, but not in STEMI.
There are three intriguing findings in our study. First, there has been a reduction in hospital admissions for AMI,9 and this might be closely related to the excess death in Korea during the COVID-19 pandemic. Little is known about the associations between patient delay and clinical outcomes during the COVID-19 pandemic in Korea. The COVID-19 pandemic is spreading rapidly around the world, causing hundreds of thousands of excess deaths in many countries.1 However, some of excess death might not be directly related to COVID-19 infection. In the United States, mortality increased by 20% during the COVID-19 pandemic from March to July 2020.10 However, COVID-19 was a documented cause of only 67% of these excess deaths. In Daegu city, Korea, crude death rate increased during the COVID-19 pandemic from February to April 2020 (Supplementary Fig. 2). However, COVID-19 was a documented cause of about 40% of these excess deaths. Interestingly, Western countries reported a decrease in hospitalization for acute cardiovascular disease (CVD) such as AMI and stroke during the COVID-19 pandemic.1112 It might be explained by true population-level reduction of acute CVD because of shifts in dietary pattern (i.e., decreased consumption of high-sodium, fast food intake),131415 reduced exposure to ambient air pollution,16171819 telemedicine,2021 decline in ambulatory CVD clinic visits, outpatient testing, deferral of elective procedures, stay-at-home messaging from government and media,222324 and seasonal variation. However, one of the possible explanations is that many patients were reluctant to visit the hospital due to the fear of contacting COVID-19.2526 Recently, Google Trends meta-data showed that search volume for chest pain is strongly correlated with COVID-19 case numbers in the Unites States. This indicates that the fear of contacting COVID-19 may be leading patients to self-triage using internet searches instead of hospital admission.27 In our study, there has been a considerable decrease in hospital admission for AMI. In addition, AMI patients visited the hospital later than usual. Although our study excluded suspected AMI patients with cardiac enzyme elevation, cardiac arrest, cardiogenic shock, or ventricular tachycardia/fibrillation who did not receive coronary angiography, the number of these patients were numerically lower in the pandemic era (Supplementary Fig. 3). Therefore, it seems to be evident that acute care of CVD may be delayed, deferred, or abbreviated during the COVID-19 pandemic. Considering the high mortality of CVD, this late presentation may increase ‘collateral COVID-19 mortality’28 and contribute to these excess deaths during the COVID-19 pandemic.29 Therefore, patients suffering from non-COVID-19 related acute CVD continue to receive timely, evidence based and high-quality care.
Second, logistics of AMI care were delayed during the COVID-19 pandemic. However, the pattern of time delay and the effect on in-hospital death and cardiac arrest were different between STEMI and non-STEMI. In the present study, patients with STEMI have a trend for longer door to balloon time during the pandemic. This system delay might be because it took time to put on personal protective equipment and to transfer patients due to uncertainty about COVID-19 infection.303132 Interestingly, the incidence of in-hospital death and cardiac arrest was lower during the pandemic. Patients with STEMI may have died while staying at home without coming to the hospital despite symptoms.3334 In addition, symptom to ER time was significantly longer and the incidence of in-hospital death and cardiac arrest was significantly higher in non-STEMI during the pandemic. Patients delay in non-STEMI due to the fear of possibility contacting patients with COVID-19 at ER is thought to have led to greater in-hospital death and cardiac arrest during the pandemic.2526 Therefore, it seems that the system delay of STEMI and the patient delay of non-STEMI differently contributed to worsening the prognosis of patients with AMI during the pandemic.
Third, ACE-I/ARBs were significantly underused for the management of AMI during the COVID-19 pandemic. In Korea, this information is interesting and valuable because there have been few real-world data regarding usage of ACE-I/ARBs for AMI in the early period of COVID-19 pandemic. Previous studies showed that COVID-19 patients with diabetes mellitus and hypertension appear to have worse prognosis due to overexpression of ACE2 receptor in airway alveolar epithelial cells because SARS-CoV-2 uses the ACE2 receptor to enter the lungs in a mechanism.353637383940 Therefore, there has been some concerns regarding the negative effect of ACE-I/ARBs by upregulation of ACE2 receptors that patients receiving ACE-I/ARBs may be more susceptible to COVID-19 infection and have poorer outcomes. Major cardiology scientific associations have rejected these correlation hypotheses for now.414243 However, in the present study, it has been documented that ACE-Is/ARBs were significantly underused for the management of AMI in the early period of the pandemic although there is no significant evidence to support an association between COVID-19 and ACE-I/ARBs. The suboptimal use of ACE-I/ARBs during the pandemic may affect the clinical outcome in this study.
This study has certain limitations that should be noted. First, because this study was a single center and observational study, we could not completely exclude the possibility of residual confounding factors that were not available in our registry. Second, we collected symptom onset time based on the patient’s memory. Therefore, we could not completely exclude the possibility of recall bias. Third, the reason for late presentation was not collected in our registry. Therefore, our results should only be regarded as hypothesis generating. However, the limitations of the study should not undermine the strength of this study, namely that it includes patients encountered in day-to-day clinical practice before and during the pandemic. Despite these limitations, we believe that our data could provide the clinical insight necessary to understand contemporary management and prognosis for AMI during the pandemic.
In conclusion, during the COVID-19 pandemic, there has been a considerable reduction in hospital admissions for AMI, time delay, and underuse of ACE-I/ARBs for the management of AMI, and this might be closely associated with the excess death in Korea.
 XML Download
XML Download