

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Calcium (Ca) makes up almost 40% of the total mineral mass in the human body. Over 99% of total body Ca is stored in the skeleton and teeth as hydroxyapatite, where it provides structural support [1]. The remaining 1% is freely available in the serum, extracellular fluid, and soft tissues [1]. Serum Ca is tightly regulated, and the body uses bone tissue as a reservoir to maintain constant concentrations of Ca in the serum, muscle, and intercellular fluids [1]. Adequate Ca intake is beneficial to bone health and possibly in the prevention of other chronic diseases, such as obesity, cancer, and cardiovascular disease [2].
The 2015 Dietary Reference Intakes for Koreans (KDRIs) for Ca was based on the effect of adequate intake on bone health owing to the limited number of studies on other health outcomes. In 2015, Ca equilibrium, bone mineral density (BMD), and fracture risk were used as major health indicators in the literature review to establish the Estimated Average Requirement (EAR) for Ca. The EAR and Recommended Nutrient Intake (RNI) for Ca were calculated using the average body size and mean Ca absorption rate of Koreans by the life-cycle stage. However, the reference body weight in some age groups was underestimated. In addition, until the revision of the 2015 KDRIs, the basis for recommendations, such as Ca accumulation during growth and Ca absorption, were mostly based on studies conducted among non-Asians. Therefore, in 2020, we focused on investigating various health outcomes associated with Ca intake and improving the 2020 KDRIs for Ca to better reflect Korean or at least Asian characteristics.
The main questions of the literature review regarding the revision of KDRIs for Ca in 2020 are as follows.
SEARCH METHODS FOR THE IDENTIFICATION OF STUDIES
Data source and literature search
Electronic databases were systematically searched according to Preferred Reporting Items for the Systematic Reviews and Meta-Analyses (PRISMA) guidelines [3]. Further search of the MEDLINE, EMBASE, and Web of Science, from January 2008 until June 2019 were performed. To search for literature reporting the data from Korean participants, additional searches of the Korean Studies Information Service System (KISS), National Digital Science Library (NDSL), DBpia, and Research Information Sharing Service (RISS) were performed. The search terms, which were based on the EAR and Tolerable Upper Intake Level (UL) for Ca, consisted of the Ca type and its synonyms (“calcium,” “calcium carbonate,” “dietary calcium,” “dairy product,” “calcium citrate,” “calcium phosphates,” “calcium malate”); health outcomes for setting the EAR (“cardiovascular disease,” “hypertension,” “pregnancy related non-skeletal disorders,” “bone health,” “growth,” “cancer,” “obesity,” “type 2 diabetes,” “metabolic syndrome,” “frailty,” “sarcopenia,” “mortality”); and health outcomes for setting the UL (“kidney stones,” “heterotopic and ossification,” “bone health,” “calcinosis,” “hypercalcemia,” “calculus”). The search terms related to the abovementioned outcomes were listed in Supplementary Tables 1 and 2. MESH terms and subject headings were used in coordination with each database’s rules. The same English search terms and additional Korean language terms, related to Ca balance and bone health, were applied to the Korean search engines: KISS; NDSL; DBpia; and RISS. Additionally, relevant Korean journals, including the Journal of Bone Metabolism, Journal of Korean Society of Food Science and Nutrition, and non-DB indexed issues of the Journal of Nutrition and Health, were hand-searched.
Study selection
The inclusion criteria were as follows: (1) studies performed only in healthy participants or participants with hypertension and diabetes mellitus, consisting of less than 20% of the study population (except for studies in adults aged 65 yrs and older); (2) interventions of dairy products, Ca supplements, or Ca and vitamin D supplements; (3) the study design was an intervention, prospective cohort, or nested case-control; and (4) cross-sectional studies and case-control studies in Asians were included due to the limited number of intervention studies in Asians. The following exclusion criteria were applied: (1) animal or cell studies; (2) conventional review paper; (3) meta-analyses; (4) studies in participants where over 20% had a disease; (5) interventions with nutrients other than Ca and vitamin D; (6) interventions where the Ca supplemented group served as control; (7) cross-sectional or case-control studies in non-Asians; (8) non-English or Korean language; and (9) unpublished data (e.g. scientific meeting abstract). Afterwards, duplicate and non-relevant studies were excluded. Abstract screening was performed with Rayyan by 3–4 research staff under the supervision of CYP and KK between 2014–2019, and independently by MJC and SYB between 2008–2013. Full-text evaluation was performed by 3–4 research staff under the supervision of CYP and KK between 2014–2019 and by MJC and SYB between 2008–2013 and disagreements were primarily resolved through discussions among the authors. We could not perform any quantitative data analysis because our search identified only a few studies by distinguished life-cycle stages and was thus inadequate to perform a meta-analysis.
Quality assessment and result summary
Quality assessment tools were applied in the systematic review for exploring scientific basis of the revision of KDRI for Ca depending on the study design, study population, risk of bias, and result consistency. The Strengthening and Reporting of Observational studies in Epidemiology (STROBE) statement [4] was used to assess the quality of cross-sectional studies. For cohort studies including nested case-control and case-control studies, the Newcastle-Ottawa scale [5] was applied. For assessment of intervention studies, the Jadad scale [6] was used. In conjunction with quality assessment, study findings were summarized in a specific table to identify feasible evidence for the revision of the 2020 KDRI for Ca.
RESULTS
Results of the systematic review for establishing the EAR for Ca
From literature published between January 2014 and June 2019, the initial database search identified 13,246 articles. After duplicates were removed, we screened 9,878 articles. The included articles were randomized controlled trials (RCTs), intervention studies, or cross-sectional studies (in Asians only) that provided information on the dose of Ca, dietary Ca intake, and Ca status of the study participants. Fifty-nine publications fulfilled the inclusion criteria for performing the quality assessment. In an additional literature search of the Korean databases and literature published between 2008 and 2013, a total of 63 articles were identified of which 6 articles were subjected to sequential review. A total of 65 studies were included in the review. The study selection process is illustrated in Fig. 1.
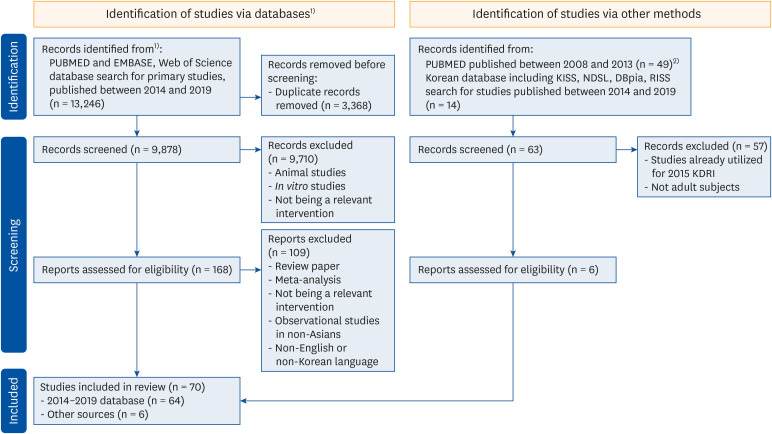
Fig. 1
Flow chart of study selection in the systematic review for the 2020 KDRIs for calcium.
KDRI, Dietary Reference Intakes for Korean; KISS, Information Service System; NDSL, National Digital Science Library; RISS, Research Information Sharing Service.
1)The format of the flow chart was adapted from the Preferred Reporting Items for the Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement.
2)Since search terms applied for the 2015 KDRIs (publications years 2008–2013) differ from that for the 2020 KDRIs (publications searched for years 2014–2019), an additional database search was performed for studies published between years 2008 and 2013 to apply the same search terms as 2014–2019 publications for bone health.
![]()
Characteristics and main findings of the included studies according to bone health indicators
Results of individual studies from the literature assessment have been outlined in Tables 1-3 according to the health indicators for setting the EAR and UL for Ca. For the bone health measurement indicators used in setting the EAR, the results of the literature were further categorized by the life-cycle stage of the participants: infants 0 to 12 mon of age; children and adolescents 1 through 18 yrs of age; and adults including postmenopausal women.
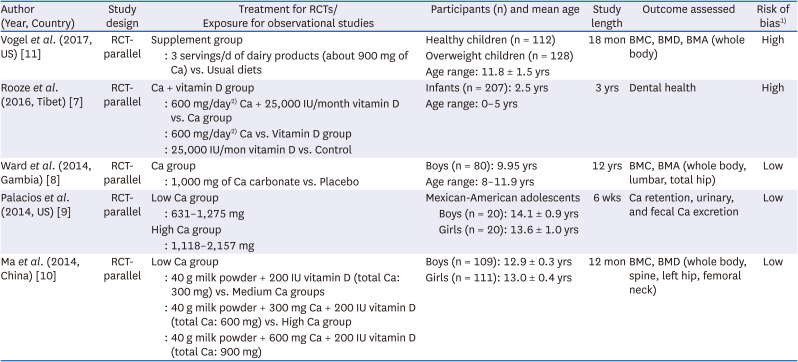
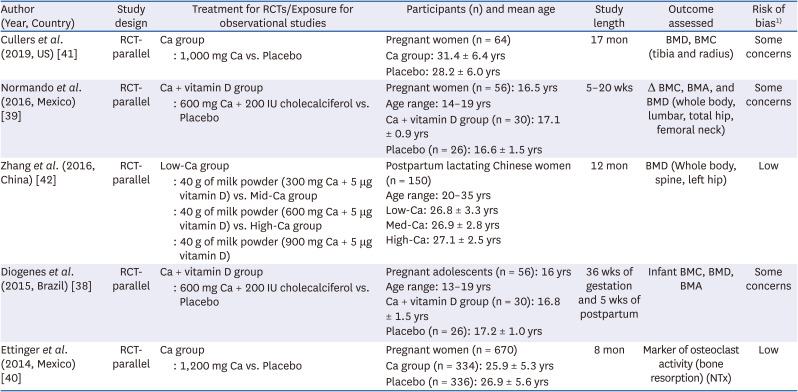
Table 1
Characteristics of the included studies examining the effect of Ca intake (EAR level) on bone health of infants, children, and adolescents aged 0 to 18 yrs (RCTs)
| Author (Year, Country) | Study design | Treatment for RCTs/Exposure for observational studies | Participants (n) and mean age | Study length | Outcome assessed | Risk of bias1) | ||
|---|---|---|---|---|---|---|---|---|
| Vogel et al. (2017, US) [11] | RCT-parallel | Supplement group | Healthy children (n = 112) | 18 mon | BMC, BMD, BMA (whole body) | High | ||
| : 3 servings/d of dairy products (about 900 mg of Ca) vs. Usual diets | Overweight children (n = 128) | |||||||
| Age range: 11.8 ± 1.5 yrs | ||||||||
| Rooze et al. (2016, Tibet) [7] | RCT-parallel | Ca + vitamin D group | Infants (n = 207): 2.5 yrs | 3 yrs | Dental health | High | ||
| : 600 mg/day2) Ca + 25,000 IU/month vitamin D vs. Ca group | Age range: 0–5 yrs | |||||||
| : 600 mg/day2) Ca vs. Vitamin D group | ||||||||
| : 25,000 IU/mon vitamin D vs. Control | ||||||||
| Ward et al. (2014, Gambia) [8] | RCT-parallel | Ca group | Boys (n = 80): 9.95 yrs | 12 yrs | BMC, BMA (whole body, lumbar, total hip) | Low | ||
| : 1,000 mg of Ca carbonate vs. Placebo | Age range: 8–11.9 yrs | |||||||
| Palacios et al. (2014, US) [9] | RCT-parallel | Low Ca group | Mexican-American adolescents | 6 wks | Ca retention, urinary, and fecal Ca excretion | Low | ||
| : 631–1,275 mg | Boys (n = 20): 14.1 ± 0.9 yrs | |||||||
| High Ca group | Girls (n = 20): 13.6 ± 1.0 yrs | |||||||
| : 1,118–2,157 mg | ||||||||
| Ma et al. (2014, China) [10] | RCT-parallel | Low Ca group | Boys (n = 109): 12.9 ± 0.3 yrs | 12 mon | BMC, BMD (whole body, spine, left hip, femoral neck) | Low | ||
| : 40 g milk powder + 200 IU vitamin D (total Ca: 300 mg) vs. Medium Ca groups | Girls (n = 111): 13.0 ± 0.4 yrs | |||||||
| : 40 g milk powder + 300 mg Ca + 200 IU vitamin D (total Ca: 600 mg) vs. High Ca group | ||||||||
| : 40 g milk powder + 600 mg Ca + 200 IU vitamin D (total Ca: 900 mg) | ||||||||
Ca, calcium; EAR, estimated average requirement; RCT, randomized controlled trial; BMC, bone mineral content; BMA, bone mineral area; BMD, bone mineral density.
1)The quality of each study is assessed on the basis of the study design, and risk of bias assessment is used for RCTs [6].
2)Ca of 15 mmol and vitamin D of 625 μg were given to the study participants. The mmol unit of Ca and μg of vitamin D are converted to mg and IU in the table, respectively.
![]()
Table 3
Characteristics of the included studies examining the effect of Ca intake (EAR level) on bone health of pregnant or lactating women (RCTs)
| Author (Year, Country) | Study design | Treatment for RCTs/Exposure for observational studies | Participants (n) and mean age | Study length | Outcome assessed | Risk of bias1) | |
|---|---|---|---|---|---|---|---|
| Cullers et al. (2019, US) [41] | RCT-parallel | Ca group | Pregnant women (n = 64) | 17 mon | BMD, BMC (tibia and radius) | Some concerns | |
| : 1,000 mg Ca vs. Placebo | Ca group: 31.4 ± 6.4 yrs | ||||||
| Placebo: 28.2 ± 6.0 yrs | |||||||
| Normando et al. (2016, Mexico) [39] | RCT-parallel | Ca + vitamin D group | Pregnant women (n = 56): 16.5 yrs | 5–20 wks | Δ BMC, BMA, and BMD (whole body, lumbar, total hip, femoral neck) | Some concerns | |
| : 600 mg Ca + 200 IU cholecalciferol vs. Placebo | Age range: 14–19 yrs | ||||||
| Ca + vitamin D group (n = 30): 17.1 ± 0.9 yrs | |||||||
| Placebo (n = 26): 16.6 ± 1.5 yrs | |||||||
| Zhang et al. (2016, China) [42] | RCT-parallel | Low-Ca group | Postpartum lactating Chinese women (n = 150) | 12 mon | BMD (Whole body, spine, left hip) | Low | |
| : 40 g of milk powder (300 mg Ca + 5 μg vitamin D) vs. Mid-Ca group | Age range: 20–35 yrs | ||||||
| : 40 g of milk powder (600 mg Ca + 5 μg vitamin D) vs. High-Ca group | Low-Ca: 26.8 ± 3.3 yrs | ||||||
| : 40 g of milk powder (900 mg Ca + 5 μg vitamin D) | Med-Ca: 26.9 ± 2.8 yrs | ||||||
| High-Ca: 27.1 ± 2.5 yrs | |||||||
| Diogenes et al. (2015, Brazil) [38] | RCT-parallel | Ca + vitamin D group | Pregnant adolescents (n = 56): 16 yrs | 36 wks of gestation and 5 wks of postpartum | Infant BMC, BMD, BMA | Some concerns | |
| : 600 mg Ca + 200 IU cholecalciferol vs. Placebo | Age range: 13–19 yrs | ||||||
| Ca + vitamin D group (n = 30): 16.8 ± 1.5 yrs | |||||||
| Placebo (n = 26): 17.2 ± 1.0 yrs | |||||||
| Ettinger et al. (2014, Mexico) [40] | RCT-parallel | Ca group | Pregnant women (n = 670) | 8 mon | Marker of osteoclast activity (bone resorption) (NTx) | Low | |
| : 1,200 mg Ca vs. Placebo | Ca group (n = 334): 25.9 ± 5.3 yrs | ||||||
| Placebo (n = 336): 26.9 ± 5.6 yrs | |||||||
Ca, calcium; EAR, Estimated Average Requirement; RCT, randomized controlled trial; BMC, bone mineral content; BMA, bone mineral area; BMD, bone mineral density; NTx, cross-linked N-telopeptides.
1)The quality of each study is assessed on the basis of the study design, and risk of bias assessment is used for RCTs [6].
![]()
Results of studies in infants aged 0 to 12 mon
In the study of infants, only one RCT study, which measured the tooth loss incidence and growth bone index was reviewed [7]. The study followed up on Tibetan children aged 0–5 yrs for 3 yrs, who received either Ca (15 mmol/day, equivalent to 600 mg/day), with or without vitamin D (625 μg/mon), or no supplement and found no significant improvement in growth and bone metabolism (Table 1). The evidence on the effect of Ca supplementation on bone health indicators in infants was limited.
Results of studies in children and adolescents aged 1 to 18 yrs
Four RCTs studies were reviewed for children and adolescents to examine the relationship between Ca intake and growth, and bone health indicators (Table 1). Gambian boys received 1 yr of Ca carbonate supplementation (1,000 mg/day), which advanced their growth spurt but had no lasting effect on bone mineral or bone size [8]. Ca retention in Mexican-American adolescents increased with Ca intake (P < 0.0001) ranging from 600 to 2,200 mg/day but did not differ by sex (P = 0.66) [9]. When Chinese adolescents aged 12–14 yrs were given 300, 600, and 900 mg of Ca supplements for 1 yr (total Ca intake including meals, 700 mg, 900 mg, and 1,300 mg), the femoral neck bone mineral content (BMC) increased regardless of sex. However, there was no significant difference between the 900 mg and 1,300 mg total Ca intake groups [10]. In the Unites States (US), white and black adolescents aged 8–16 yrs were classified based on body weight into healthy weight group (50–70 percentile), overweight group (85 percentile or more), and allocated to a supplement group (900 mg Ca/day per day through 3 servings of dairy products) or control group. Bone indicators were observed every 6 mon for 18 mon, and the bone content of the tibia increased by 4% in the supplement group; however, there was no significant difference regarding other bone indices [11].
The current recommended Ca intake in Korea is 1,000 mg and 900 mg for boys, and 900 mg and 800 mg for girls aged 12–14 yrs and 15–18 yrs, respectively [12]. The results of reviewed studies suggested that Ca supplementation in children and adolescents would be helpful in accumulating bone mass, but the amounts of Ca intake reported in these studies to increase bone accumulation were not different from the Ca requirement stated in the 2015 KDRIs calculated based on the physical growth standard. Therefore, there was no evidence to warrant reduction or increment of the currently applied Ca intake in children and adolescents.
Results of studies on men aged 19 yrs and older, and young women
Of the literature evaluated regarding bone health indicators including BMD, BMC, bone mineral area (BMA), and serum metabolites in adults, eleven studies were 2-armed RCTs [1314151617181920212223], and one was a cross-over study [24]; 5 of the studies were from the US, 2 from the United Kingdom (UK) [1620], 2 from Australia [1318], one from China [19], one from Japan [23], and one from Thailand [25]. Ten studies were cross-sectional [25262728293031323334], of which 7 were from Korea [25272829303233], one from Japan [26], one from Saudi Arabia [34], and one from India [31] (Table 2).
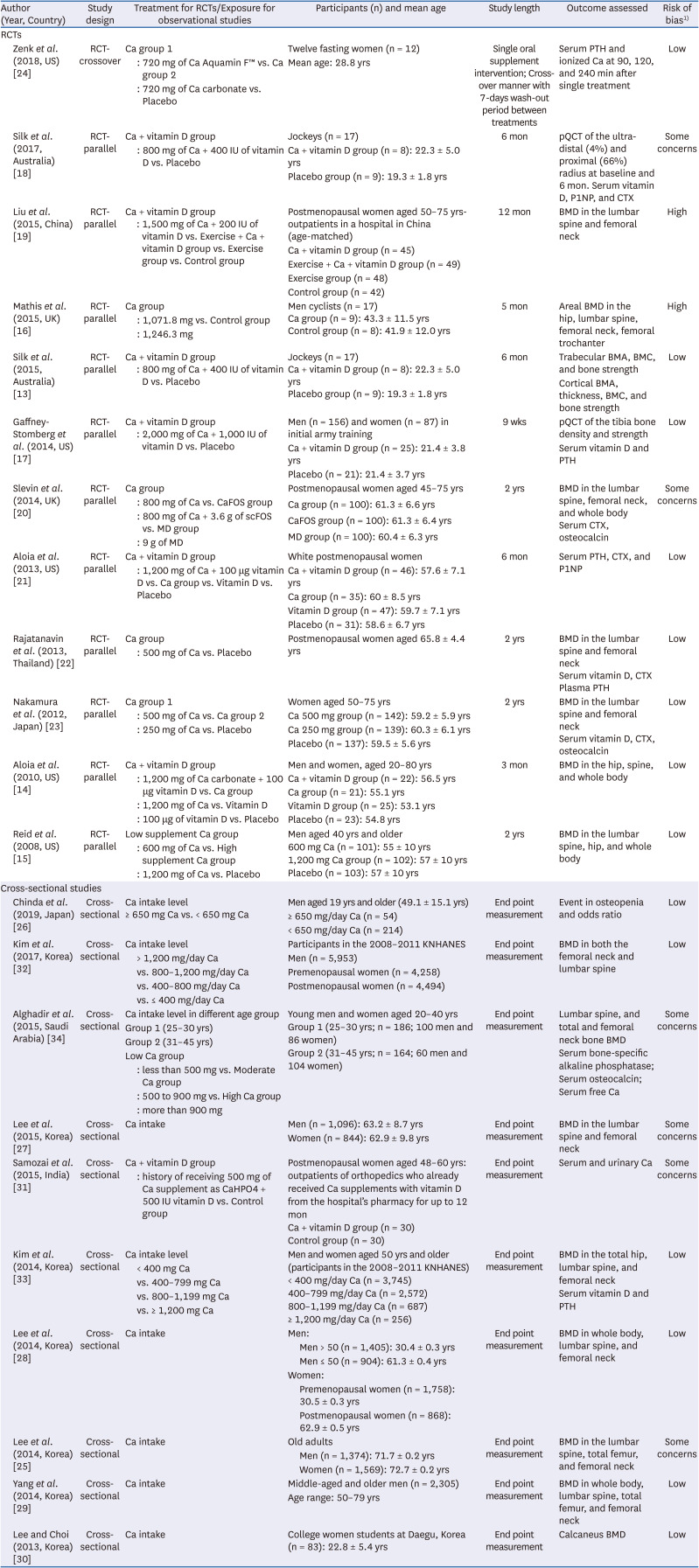
Table 2
Characteristics of the included studies examining the effect of Ca intake (EAR level) on bone health of adults aged 19 yrs and older
| Author (Year, Country) | Study design | Treatment for RCTs/Exposure for observational studies | Participants (n) and mean age | Study length | Outcome assessed | Risk of bias1) | |||
|---|---|---|---|---|---|---|---|---|---|
| RCTs | |||||||||
| Zenk et al. (2018, US) [24] | RCT-crossover | Ca group 1 | Twelve fasting women (n = 12) | Single oral supplement intervention; Cross-over manner with 7-days wash-out period between treatments | Serum PTH and ionized Ca at 90, 120, and 240 min after single treatment | Low | |||
| : 720 mg of Ca Aquamin F™ vs. Ca group 2 | Mean age: 28.8 yrs | ||||||||
| : 720 mg of Ca carbonate vs. Placebo | |||||||||
| Silk et al. (2017, Australia) [18] | RCT-parallel | Ca + vitamin D group | Jockeys (n = 17) | 6 mon | pQCT of the ultra-distal (4%) and proximal (66%) radius at baseline and 6 mon. Serum vitamin D, P1NP, and CTX | Some concerns | |||
| : 800 mg of Ca + 400 IU of vitamin D vs. Placebo | Ca + vitamin D group (n = 8): 22.3 ± 5.0 yrs | ||||||||
| Placebo group (n = 9): 19.3 ± 1.8 yrs | |||||||||
| Liu et al. (2015, China) [19] | RCT-parallel | Ca + vitamin D group | Postmenopausal women aged 50–75 yrs-outpatients in a hospital in China (age-matched) | 12 mon | BMD in the lumbar spine and femoral neck | High | |||
| : 1,500 mg of Ca + 200 IU of vitamin D vs. Exercise + Ca + vitamin D group vs. Exercise group vs. Control group | Ca + vitamin D group (n = 45) | ||||||||
| Exercise + Ca + vitamin D group (n = 49) | |||||||||
| Exercise group (n = 48) | |||||||||
| Control group (n = 42) | |||||||||
| Mathis et al. (2015, UK) [16] | RCT-parallel | Ca group | Men cyclists (n = 17) | 5 mon | Areal BMD in the hip, lumbar spine, femoral neck, femoral trochanter | High | |||
| : 1,071.8 mg vs. Control group | Ca group (n = 9): 43.3 ± 11.5 yrs | ||||||||
| : 1,246.3 mg | Control group (n = 8): 41.9 ± 12.0 yrs | ||||||||
| Silk et al. (2015, Australia) [13] | RCT-parallel | Ca + vitamin D group | Jockeys (n = 17) | 6 mon | Trabecular BMA, BMC, and bone strength | Low | |||
| : 800 mg of Ca + 400 IU of vitamin D vs. Placebo | Ca + vitamin D group (n = 8): 22.3 ± 5.0 yrs | Cortical BMA, thickness, BMC, and bone strength | |||||||
| Placebo group (n = 9): 19.3 ± 1.8 yrs | |||||||||
| Gaffney-Stomberg et al. (2014, US) [17] | RCT-parallel | Ca + vitamin D group | Men (n = 156) and women (n = 87) in initial army training | 9 wks | pQCT of the tibia bone density and strength | Low | |||
| : 2,000 mg of Ca + 1,000 IU of vitamin D vs. Placebo | Ca + vitamin D group (n = 25): 21.4 ± 3.8 yrs | Serum vitamin D and PTH | |||||||
| Placebo (n = 21): 21.4 ± 3.7 yrs | |||||||||
| Slevin et al. (2014, UK) [20] | RCT-parallel | Ca group | Postmenopausal women aged 45–75 yrs | 2 yrs | BMD in the lumbar spine, femoral neck, and whole body | Some concerns | |||
| : 800 mg of Ca vs. CaFOS group | Ca group (n = 100): 61.3 ± 6.6 yrs | Serum CTX, osteocalcin | |||||||
| : 800 mg of Ca + 3.6 g of scFOS vs. MD group | CaFOS group (n = 100): 61.3 ± 6.4 yrs | ||||||||
| : 9 g of MD | MD group (n = 100): 60.4 ± 6.3 yrs | ||||||||
| Aloia et al. (2013, US) [21] | RCT-parallel | Ca + vitamin D group | White postmenopausal women | 6 mon | Serum PTH, CTX, and P1NP | Low | |||
| : 1,200 mg of Ca + 100 μg vitamin D vs. Ca group vs. Vitamin D vs. Placebo | Ca + vitamin D group (n = 46): 57.6 ± 7.1 yrs | ||||||||
| Ca group (n = 35): 60 ± 8.5 yrs | |||||||||
| Vitamin D group (n = 47): 59.7 ± 7.1 yrs | |||||||||
| Placebo (n = 31): 58.6 ± 6.7 yrs | |||||||||
| Rajatanavin et al. (2013, Thailand) [22] | RCT-parallel | Ca group | Postmenopausal women aged 65.8 ± 4.4 yrs | 2 yrs | BMD in the lumbar spine and femoral neck | Low | |||
| : 500 mg of Ca vs. Placebo | Serum vitamin D, CTX | ||||||||
| Plasma PTH | |||||||||
| Nakamura et al. (2012, Japan) [23] | RCT-parallel | Ca group 1 | Women aged 50–75 yrs | 2 yrs | BMD in the lumbar spine and femoral neck | Low | |||
| : 500 mg of Ca vs. Ca group 2 | Ca 500 mg group (n = 142): 59.2 ± 5.9 yrs | Serum vitamin D, CTX, osteocalcin | |||||||
| : 250 mg of Ca vs. Placebo | Ca 250 mg group (n = 139): 60.3 ± 6.1 yrs | ||||||||
| Placebo (n = 137): 59.5 ± 5.6 yrs | |||||||||
| Aloia et al. (2010, US) [14] | RCT-parallel | Ca + vitamin D group | Men and women, aged 20–80 yrs | 3 mon | BMD in the hip, spine, and whole body | Low | |||
| : 1,200 mg of Ca carbonate + 100 μg vitamin D vs. Ca group | Ca + vitamin D group (n = 22): 56.5 yrs | ||||||||
| : 1,200 mg of Ca vs. Vitamin D | Ca group (n = 21): 55.1 yrs | ||||||||
| : 100 μg of vitamin D vs. Placebo | Vitamin D group (n = 25): 53.1 yrs | ||||||||
| Placebo (n = 23): 54.8 yrs | |||||||||
| Reid et al. (2008, US) [15] | RCT-parallel | Low supplement Ca group | Men aged 40 yrs and older | 2 yrs | BMD in the lumbar spine, hip, and whole body | Low | |||
| : 600 mg of Ca vs. High supplement Ca group | 600 mg Ca (n = 101): 55 ± 10 yrs | ||||||||
| : 1,200 mg of Ca vs. Placebo | 1,200 mg Ca group (n = 102): 57 ± 10 yrs | ||||||||
| Placebo (n = 103): 57 ± 10 yrs | |||||||||
| Cross-sectional studies | |||||||||
| Chinda et al. (2019, Japan) [26] | Cross-sectional | Ca intake level | Men aged 19 yrs and older (49.1 ± 15.1 yrs) | End point measurement | Event in osteopenia and odds ratio | Low | |||
| ≥ 650 mg Ca vs. < 650 mg Ca | ≥ 650 mg/day Ca (n = 54) | ||||||||
| < 650 mg/day Ca (n = 214) | |||||||||
| Kim et al. (2017, Korea) [32] | Cross-sectional | Ca intake level | Participants in the 2008–2011 KNHANES | End point measurement | BMD in both the femoral neck and lumbar spine | Low | |||
| > 1,200 mg/day Ca | Men (n = 5,953) | ||||||||
| vs. 800–1,200 mg/day Ca | Premenopausal women (n = 4,258) | ||||||||
| vs. 400–800 mg/day Ca | Postmenopausal women (n = 4,494) | ||||||||
| vs. ≤ 400 mg/day Ca | |||||||||
| Alghadir et al. (2015, Saudi Arabia) [34] | Cross-sectional | Ca intake level in different age group | Young men and women aged 20–40 yrs | End point measurement | Lumbar spine, and total and femoral neck bone BMD | Some concerns | |||
| Group 1 (25–30 yrs) | Group 1 (25–30 yrs; n = 186; 100 men and 86 women) | Serum bone-specific alkaline phosphatase; Serum osteocalcin; Serum free Ca | |||||||
| Group 2 (31–45 yrs) | Group 2 (31–45 yrs; n = 164; 60 men and 104 women) | ||||||||
| Low Ca group | |||||||||
| : less than 500 mg vs. Moderate Ca group | |||||||||
| : 500 to 900 mg vs. High Ca group | |||||||||
| : more than 900 mg | |||||||||
| Lee et al. (2015, Korea) [27] | Cross-sectional | Ca intake | Men (n = 1,096): 63.2 ± 8.7 yrs | End point measurement | BMD in the lumbar spine and femoral neck | Some concerns | |||
| Women (n = 844): 62.9 ± 9.8 yrs | |||||||||
| Samozai et al. (2015, India) [31] | Cross-sectional | Ca + vitamin D group | Postmenopausal women aged 48–60 yrs: outpatients of orthopedics who already received Ca supplements with vitamin D from the hospital’s pharmacy for up to 12 mon | End point measurement | Serum and urinary Ca | Some concerns | |||
| : history of receiving 500 mg of Ca supplement as CaHPO4 + 500 IU vitamin D vs. Control group | Ca + vitamin D group (n = 30) | ||||||||
| Control group (n = 30) | |||||||||
| Kim et al. (2014, Korea) [33] | Cross-sectional | Ca intake level | Men and women aged 50 yrs and older (participants in the 2008–2011 KNHANES) | End point measurement | BMD in the total hip, lumbar spine, and femoral neck | Low | |||
| < 400 mg Ca | < 400 mg/day Ca (n = 3,745) | Serum vitamin D and PTH | |||||||
| vs. 400–799 mg Ca | 400–799 mg/day Ca (n = 2,572) | ||||||||
| vs. 800–1,199 mg Ca | 800–1,199 mg/day Ca (n = 687) | ||||||||
| vs. ≥ 1,200 mg Ca | ≥ 1,200 mg/day Ca (n = 256) | ||||||||
| Lee et al. (2014, Korea) [28] | Cross-sectional | Ca intake | Men: | End point measurement | BMD in whole body, lumbar spine, and femoral neck | Low | |||
| Men > 50 (n = 1,405): 30.4 ± 0.3 yrs | |||||||||
| Men ≤ 50 (n = 904): 61.3 ± 0.4 yrs | |||||||||
| Women: | |||||||||
| Premenopausal women (n = 1,758): 30.5 ± 0.3 yrs | |||||||||
| Postmenopausal women (n = 868): 62.9 ± 0.5 yrs | |||||||||
| Lee et al. (2014, Korea) [25] | Cross-sectional | Ca intake | Old adults | End point measurement | BMD in the lumbar spine, total femur, and femoral neck | Some concerns | |||
| Men (n = 1,374): 71.7 ± 0.2 yrs | |||||||||
| Women (n = 1,569): 72.7 ± 0.2 yrs | |||||||||
| Yang et al. (2014, Korea) [29] | Cross-sectional | Ca intake | Middle-aged and older men (n = 2,305) | End point measurement | BMD in whole body, lumbar spine, total femur, and femoral neck | Low | |||
| Age range: 50–79 yrs | |||||||||
| Lee and Choi (2013, Korea) [30] | Cross-sectional | Ca intake | College women students at Daegu, Korea (n = 83): 22.8 ± 5.4 yrs | End point measurement | Calcaneus BMD | Low | |||
Ca, calcium; EAR, Estimated Average Requirement; Aquamin F™, botanical Ca derived from the marine algal Lithothamnion sp.; BMA, bone mineral area; BMC, bone mineral content; BMD, bone mineral density; P1NP, procollagen type 1 N propeptide; CTX, C-terminal cross-linked telopeptide of type 1 collagen; KNHANES, Korea National Health and Nutrition Examination Survey; PTH, parathyroid hormone; pQCT, peripheral Quantitative Computed Tomography; scFOS, short-chain fructo-oligosaccharide; RCT, randomized controlled trial; CaFOS, 800 mg of calcium with 3 g of short-chain fructo-oligosaccharide; MD, maltodextrin.
![]()
A total of 7 RCT studies reported findings for adult men and young women. In a study conducted with healthy young Australian jockeys in their twenties, Ca supplementation of 800 mg and 400 IU vitamin D for 6 mon significantly increased BMC (6.6%), BMA (5.9%), and BMD (1.3%) in the proximal cortical bone of the tibia; however, these changes were not significantly different from the placebo-control group [1213]. The group supplemented with the same amount of Ca and vitamin D had shown higher vitamin D levels (18.1%, P = 0.014, partial η2 = 0.38) and lower C-terminal cross-linked telopeptide of type I collagen (CTX) (−24.8%, P = 0.011), but there was no difference in either trabecular or cortical bone properties between groups [18]. In a study with male and female military personnel (mean age, 21.4 yrs) Ca supplementation with 2,000 mg and 1,000 IU vitamin D increased serum Ca levels, BMD, BMC, and thickness of the cortical bone by 14% in both groups [17]. Ca consumption of 1,600 mg and 1,000 IU of vitamin D prior to cycling for 5 mon did not ameliorate the negative effects of competitive cycling on the hip BMD in male road cyclists [16]. Overall, the findings regarding the change in bone health indicators in response to Ca supplementation are inconsistent. In addition, participants in the aforementioned studies, such as athletes and soldiers, are under repetitive physical loading [131718]; therefore, the results may not apply to general adults whose physical activity strength is weak or moderate. In 2 additional reviewed RCTs reported during 2008–2013, healthy men in the US (mean age, 57 yrs) who consumed 600 mg or 1,200 mg of Ca have shown an increased level of serum alkaline phosphatase, a bone formation indicator, and a decreased level of CTX, a bone resorption marker, in a dose-dependent manner compared to those in the placebo group. However, BMD was found to increase by 1.0–1.5% only in a group of participants who consumed 1,200 mg of Ca [15]. Ca supplementation with 1,200 mg for 3 mon decreased the serum bone resorption marker in healthy adult men and women in the US population (age range, 20–80 yrs old) [14]. An RCT conducted with healthy women (mean age, 28.8 yrs) reported increased parathyroid hormone (PTH) level after commercially manufactured Ca supplementation. However, this study only performed a single time point of Ca supplementation in participants with obesity (body mass index [BMI] > 25.5), and their sodium intake was limited to < 100 mEq [24] indicating that this evidence would be ineligible for extrapolation regarding the level of Ca consumption from the daily diet.
A total of 9 cross-sectional studies were reviewed to explore evidence in setting the EAR for Ca in adult men and young women. Of the study results reported, Japanese men who consumed Ca < 650 mg/day have shown a 2.92-fold higher risk of osteopenia than men who took Ca ≥ 650 mg/day (95% confidence interval, 1.09–7.81) [26]. A study on Korean men (aged < 50 yrs) reported a positive association between Ca intake and BMD in the femoral neck and lumbar spine [25272829], while no significant association was observed in men aged ≥ 50 yrs [28]. A study conducted in Daegu, a metropolitan city in Korea, reported that Ca intake in young Korean female college students (mean age, 22.8 yrs old; mean BMI, 21.8) was only 77% of the RNI [30]. This study also reported that the mean Ca intake was 568.9 mg in students of the normal BMD group and 446.2 mg in students of the osteopenia group without significant difference in energy consumption between the groups [30], indicating a positive relationship between Ca intake and Ca accretion in young women. The levels of Ca used in these studies are mostly in the range of the EAR for Ca in the 2015 KDRI [12].
Results of studies on postmenopausal women aged 50–75 yrs
In finding evidence in postmenopausal women, 5 RCTs and 4 cross-sectional studies were reviewed. Postmenopausal women aged 50–75 yrs who participated in the program of exercise (“the modified eighth section of the Eight-Section Brocade”) with 500 mg of daily Ca intake for 12 mon have shown increased lumbar spine BMD compared to women in a group only receiving Ca supplement without physical activity [19]. However, the study did not assess the amount of Ca obtained from the participants’ daily diet; hence, the exact amount of total Ca intake could not be inferred. Additionally, the effect of Ca on bone indicators could not be distinguished from the effect of physical activity. In women aged 45–75 yrs who were residing in the Ulster area in the UK, Ca intake of 900 mg/day for 1 yr did not induce any change in bone parameters in the lumbar spine and femoral neck during the 1-yr follow-up period [20]. Ca supplementation with 1,200 mg/day for 3 mon decreased the serum CTX, bone resorption marker, and PTH level in response to instant Ca load in healthy postmenopausal white American women [21]. However, the level of Ca effective in bone metabolism indicators reported in Asian countries are uncertain because the study participants’ basal Ca intake is different per study or not reported. A study conducted in Thailand reported that approximately 800 mg/day of Ca intake including the dietary Ca for 2 yrs increased the lumbar BMD by 2.7% compared to baseline measurement in healthy Thai postmenopausal women whose average daily Ca intake is 376 mg [22]. In a study conducted with Japanese postmenopausal women aged 50–75 yrs, Ca supplements of 500 mg/day slowed bone loss in the lumbar spine and femoral neck during a 2-yr follow-up period in perimenopause and postmenopausal women with a habitually low Ca intake (< 500 mg/day) [23]. Indian postmenopausal women, outpatients of orthopedics, who had a history of receiving tablets containing 500 mg Ca and 500 IU vitamin D for at least a month up to 12 mon have shown an increased urinary Ca excretion without the change in the serum Ca level, indicating enhanced Ca retention [31]. In the Korea National Health and Nutrition Examination Survey (KNHANES) conducted on the Korean population, Ca intake was positively correlated with the whole-body BMD in premenopausal women, while no significant association was detected in postmenopausal women aged ≥ 50 yrs [252728]. Another study, which analyzed the data from the 2008–2011 KNHANES, reported the association between Ca intake and the risk of metabolic syndrome and BMD [32]. In this study, participants were categorized by their daily Ca intake amount: < 400 mg; 400–800 mg; 800–1,200 mg; and ≥ 1,200 mg. Increased lumbar and femoral BMD and decreased odds ratio for the risk of osteoporosis were reported in groups with a Ca intake of 400–800 mg. Position statements of the 2015 Korean Society for Bone and Mineral Metabolism (KSBMM) recommended a daily Ca intake of 800–1,000 mg/day for preventing and treating osteoporosis in Korean postmenopausal women and men aged ≥ 50 yrs [35]. In the 2015 KDRIs, an extra 100 mg/day of Ca was added to the calculated RNIs for postmenopausal women as a reasonable margin of safety for lessening bone loss due to the typically low Ca intake of Korean women and need for public health protection at this life stage [12]. Postmenopausal women have a particularly higher risk of fracture, which may be exacerbated with inadequate Ca intake. Observational studies in Koreans indicate that adults with dietary Ca intakes over 668 mg/day have lower PTH and higher BMD at the femoral neck and spine [36], whereas others show that dietary intake of 800 mg/day and above is associated with better bone health despite adequate D status [33]. However, Ca intake through supplements was not accounted for in these studies. Nevertheless, these intakes are similar to the requirements calculated from a balance study in Japanese older adults [37].
In the literature reviewed in assessing the EAR for Ca in adults, findings from the RCTs were inconsistent due to different study conditions. Study participants under atypical physical activity were included, such as cyclists, soldiers, and jockeys, and the use of a broad range of Ca doses. Furthermore, inferring the proper Ca level, which may be advantageous to bone health outcomes on the data from Asian countries appears unreliable in Korean adults because the basal Ca intake of study participants varies per studies, and the Ca absorption data specific in the Korean population is almost scarce. Hence, the results achieved before June 2019 are not applicable to the general Korean adult population, including postmenopausal women in the 2020 KDRI.
Results of studies in pregnant or lactating women
In terms of the evidence in pregnant or lactating women, a total of 5 RCT studies were reviewed (Table 3). In Brazilian adolescent mothers who received Ca (600 mg/day) plus cholecalciferol (200 IU/day) supplementation or placebo from 26 wks of gestation to parturition, the BMC, BMD, and bone area BA changes in infants born were not different between supplementation and placebo group. However, infant body weight and its increment were higher in the supplemented group [38]. Another study of pregnant adolescents in Brazil aged 13–19 yrs reported that changes in bone mass by Ca supplementation were dependent on the genotype of the vitamin D receptor (VDR) [39]. In a study of short-term interventions in adult pregnant women, participants in their first trimester of pregnancy who received either 1,200 mg/day Ca or placebo were followed through 1-mon postpartum. Ca excretion in the Ca supplement group decreased by 15.8% on average, as compared to the placebo group, but there was no significant effect of Ca on bone formation. However, in participants who consumed 50% or more of the prescribed Ca, the bone speed of sound of the arm bone, which is an index of increase in bone thickness, increased by 59.0 m/s (P = 0.009) at 1 mon after childbirth [40]. In White and Black American pregnant women aged 19–50 yrs who received 1,000 mg of Ca and 2,000 IU of vitamin D for 36 mon, the supplement group had significantly greater increases in radial total BMD (P = 0.02) and tibial cortical BMD (P = 0.03) at 12 mon postpartum than the placebo group [41]. In Chinese postpartum lactating women, change in BMD from baseline to 12 mon among the 3 groups of 300 mg Ca (40 g milk powder), 600 mg Ca (40 g milk powder and 300 mg Ca supplement), and 900 mg Ca (40 g milk powder and 600 mg Ca supplement) was not significantly different [42].
Overall, the evidence on the effect of Ca supplementation on bone health indicators in pregnant or lactating women was limited or inconsistent. The results showed that the positive changes in bone health indicators after Ca supplementation during pregnancy and lactation were not significant.
Characteristics and main findings of studies according to health outcomes other than bone
The main findings of the studies extracted through the search of keywords related to health outcomes other than bone health in setting the EAR for Ca were summarized in Tables 4-7. Other health outcomes included growth (5 RCTs, 2 cohort, and one nested case-control), cardiovascular disease (7 RCTs and 2 cross-sectional), hypertension (3 RCTs and 3 cohort), obesity, diabetes, and metabolic syndrome (4 RCTs, 6 cohort, and one cross-sectional) cancer (one RCTs and one cohort), frailty & sarcopenia (2 RCTs). Overall, reviews of cancer, frailty and sarcopenia among non-bone health outcomes were excluded because of a small number of studies reviewed in this study.
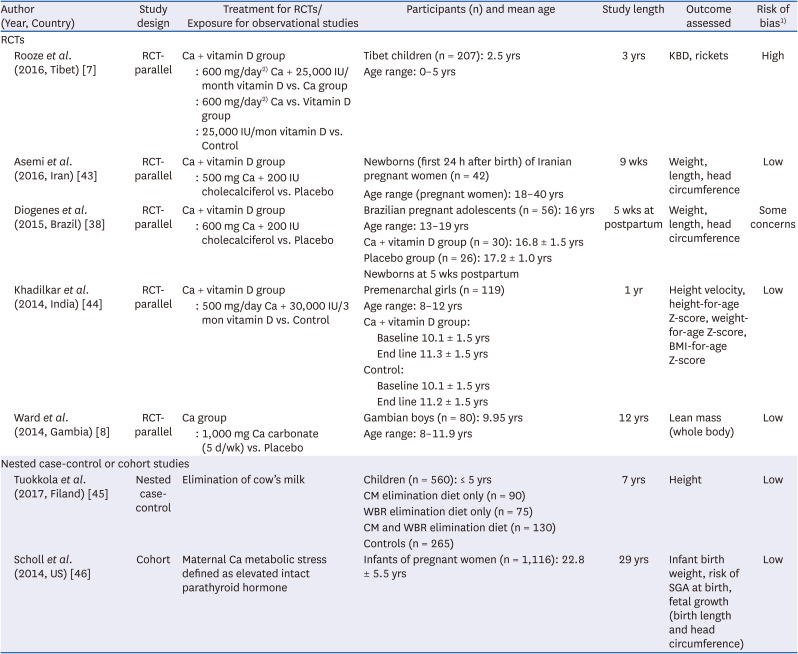
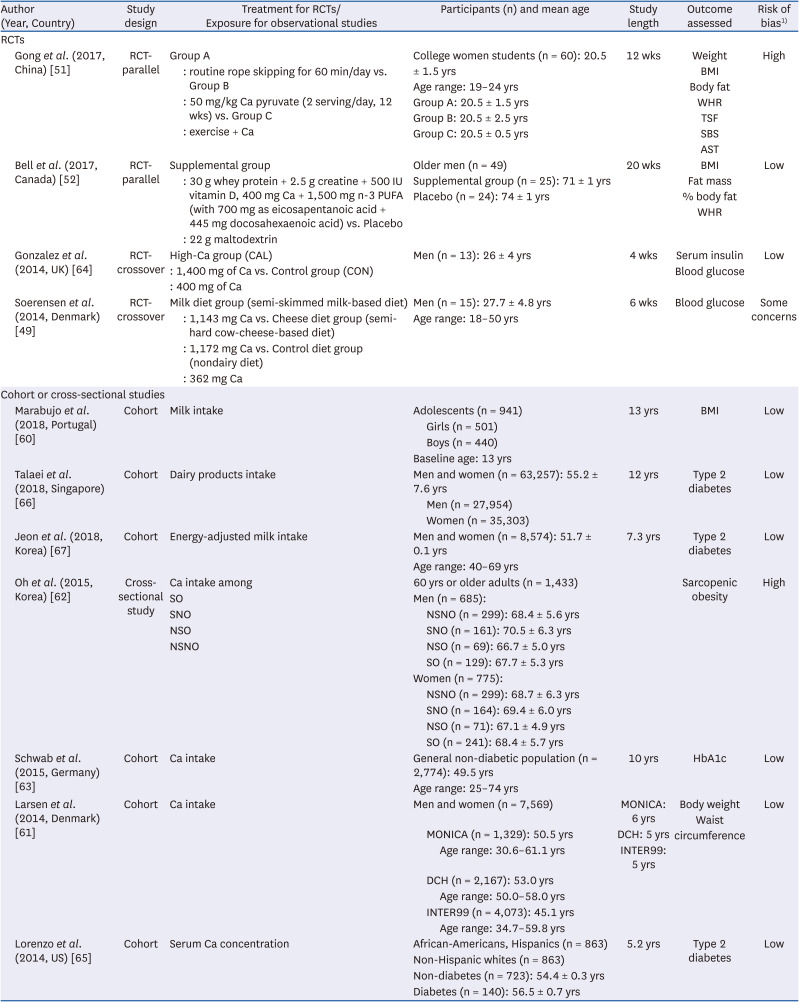
Table 4
Characteristics of the included studies examining the effect of Ca intake (EAR level) on growth
| Author (Year, Country) | Study design | Treatment for RCTs/Exposure for observational studies | Participants (n) and mean age | Study length | Outcome assessed | Risk of bias1) | |||
|---|---|---|---|---|---|---|---|---|---|
| RCTs | |||||||||
| Rooze et al. (2016, Tibet) [7] | RCT-parallel | Ca + vitamin D group | Tibet children (n = 207): 2.5 yrs | 3 yrs | KBD, rickets | High | |||
| : 600 mg/day2) Ca + 25,000 IU/month vitamin D vs. Ca group | Age range: 0–5 yrs | ||||||||
| : 600 mg/day2) Ca vs. Vitamin D group | |||||||||
| : 25,000 IU/mon vitamin D vs. Control | |||||||||
| Asemi et al. (2016, Iran) [43] | RCT-parallel | Ca + vitamin D group | Newborns (first 24 h after birth) of Iranian pregnant women (n = 42) | 9 wks | Weight, length, head circumference | Low | |||
| : 500 mg Ca + 200 IU cholecalciferol vs. Placebo | Age range (pregnant women): 18–40 yrs | ||||||||
| Diogenes et al. (2015, Brazil) [38] | RCT-parallel | Ca + vitamin D group | Brazilian pregnant adolescents (n = 56): 16 yrs | 5 wks at postpartum | Weight, length, head circumference | Some concerns | |||
| : 600 mg Ca + 200 IU cholecalciferol vs. Placebo | Age range: 13–19 yrs | ||||||||
| Ca + vitamin D group (n = 30): 16.8 ± 1.5 yrs | |||||||||
| Placebo group (n = 26): 17.2 ± 1.0 yrs | |||||||||
| Newborns at 5 wks postpartum | |||||||||
| Khadilkar et al. (2014, India) [44] | RCT-parallel | Ca + vitamin D group | Premenarchal girls (n = 119) | 1 yr | Height velocity, height-for-age Z-score, weight-for-age Z-score, BMI-for-age Z-score | Low | |||
| : 500 mg/day Ca + 30,000 IU/3 mon vitamin D vs. Control | Age range: 8–12 yrs | ||||||||
| Ca + vitamin D group: | |||||||||
| Baseline 10.1 ± 1.5 yrs | |||||||||
| End line 11.3 ± 1.5 yrs | |||||||||
| Control: | |||||||||
| Baseline 10.1 ± 1.5 yrs | |||||||||
| End line 11.2 ± 1.5 yrs | |||||||||
| Ward et al. (2014, Gambia) [8] | RCT-parallel | Ca group | Gambian boys (n = 80): 9.95 yrs | 12 yrs | Lean mass (whole body) | Low | |||
| : 1,000 mg Ca carbonate (5 d/wk) vs. Placebo | Age range: 8–11.9 yrs | ||||||||
| Nested case-control or cohort studies | |||||||||
| Tuokkola et al. (2017, Filand) [45] | Nested case-control | Elimination of cow’s milk | Children (n = 560): ≤ 5 yrs | 7 yrs | Height | Low | |||
| CM elimination diet only (n = 90) | |||||||||
| WBR elimination diet only (n = 75) | |||||||||
| CM and WBR elimination diet (n = 130) | |||||||||
| Controls (n = 265) | |||||||||
| Scholl et al. (2014, US) [46] | Cohort | Maternal Ca metabolic stress defined as elevated intact parathyroid hormone | Infants of pregnant women (n = 1,116): 22.8 ± 5.5 yrs | 29 yrs | Infant birth weight, risk of SGA at birth, fetal growth (birth length and head circumference) | Low | |||
Ca, calcium; EAR, Estimated Average Requirement; KBD, Kashin–Beck disease; SGA, small-for-gestational-age; CM, cow's milk; WBR, wheat, barley or rye; RCT, randomized controlled trial; BMI, body mass index.
1)The quality of each study is assessed on the basis of the study design, and risk of bias assessment is used for RCTs [6] cohort or cross-sectional studies [4].
2)Ca of 15 mmol and vitamin D of 625 μg were given to the study participants. The mmol unit of Ca and μg of vitamin D are converted to mg and IU in the table, respectively.
![]()
Table 7
Characteristics of the included studies examining the effect of Ca intake (EAR level) on obesity, diabetes, and metabolic syndrome
| Author (Year, Country) | Study design | Treatment for RCTs/Exposure for observational studies | Participants (n) and mean age | Study length | Outcome assessed | Risk of bias1) | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| RCTs | ||||||||||
| Gong et al. (2017, China) [51] | RCT-parallel | Group A | College women students (n = 60): 20.5 ± 1.5 yrs | 12 wks | Weight | High | ||||
| : routine rope skipping for 60 min/day vs. Group B | Age range: 19–24 yrs | BMI | ||||||||
| : 50 mg/kg Ca pyruvate (2 serving/day, 12 wks) vs. Group C | Group A: 20.5 ± 1.5 yrs | Body fat | ||||||||
| : exercise + Ca | Group B: 20.5 ± 2.5 yrs | WHR | ||||||||
| Group C: 20.5 ± 0.5 yrs | TSF | |||||||||
| SBS | ||||||||||
| AST | ||||||||||
| Bell et al. (2017, Canada) [52] | RCT-parallel | Supplemental group | Older men (n = 49) | 20 wks | BMI | Low | ||||
| : 30 g whey protein + 2.5 g creatine + 500 IU vitamin D, 400 mg Ca + 1,500 mg n-3 PUFA (with 700 mg as eicosapentanoic acid + 445 mg docosahexaenoic acid) vs. Placebo | Supplemental group (n = 25): 71 ± 1 yrs | Fat mass | ||||||||
| : 22 g maltodextrin | Placebo (n = 24): 74 ± 1 yrs | % body fat | ||||||||
| WHR | ||||||||||
| Gonzalez et al. (2014, UK) [64] | RCT-crossover | High-Ca group (CAL) | Men (n = 13): 26 ± 4 yrs | 4 wks | Serum insulin | Low | ||||
| : 1,400 mg of Ca vs. Control group (CON) | Blood glucose | |||||||||
| : 400 mg of Ca | ||||||||||
| Soerensen et al. (2014, Denmark) [49] | RCT-crossover | Milk diet group (semi-skimmed milk-based diet) | Men (n = 15): 27.7 ± 4.8 yrs | 6 wks | Blood glucose | Some concerns | ||||
| : 1,143 mg Ca vs. Cheese diet group (semi-hard cow-cheese-based diet) | Age range: 18–50 yrs | |||||||||
| : 1,172 mg Ca vs. Control diet group (nondairy diet) | ||||||||||
| : 362 mg Ca | ||||||||||
| Cohort or cross-sectional studies | ||||||||||
| Marabujo et al. (2018, Portugal) [60] | Cohort | Milk intake | Adolescents (n = 941) | 13 yrs | BMI | Low | ||||
| Girls (n = 501) | ||||||||||
| Boys (n = 440) | ||||||||||
| Baseline age: 13 yrs | ||||||||||
| Talaei et al. (2018, Singapore) [66] | Cohort | Dairy products intake | Men and women (n = 63,257): 55.2 ± 7.6 yrs | 12 yrs | Type 2 diabetes | Low | ||||
| Men (n = 27,954) | ||||||||||
| Women (n = 35,303) | ||||||||||
| Jeon et al. (2018, Korea) [67] | Cohort | Energy-adjusted milk intake | Men and women (n = 8,574): 51.7 ± 0.1 yrs | 7.3 yrs | Type 2 diabetes | Low | ||||
| Age range: 40–69 yrs | ||||||||||
| Oh et al. (2015, Korea) [62] | Cross-sectional study | Ca intake among | 60 yrs or older adults (n = 1,433) | Sarcopenic obesity | High | |||||
| SO | Men (n = 685): | |||||||||
| SNO | NSNO (n = 299): 68.4 ± 5.6 yrs | |||||||||
| NSO | SNO (n = 161): 70.5 ± 6.3 yrs | |||||||||
| NSNO | NSO (n = 69): 66.7 ± 5.0 yrs | |||||||||
| SO (n = 129): 67.7 ± 5.3 yrs | ||||||||||
| Women (n = 775): | ||||||||||
| NSNO (n = 299): 68.7 ± 6.3 yrs | ||||||||||
| SNO (n = 164): 69.4 ± 6.0 yrs | ||||||||||
| NSO (n = 71): 67.1 ± 4.9 yrs | ||||||||||
| SO (n = 241): 68.4 ± 5.7 yrs | ||||||||||
| Schwab et al. (2015, Germany) [63] | Cohort | Ca intake | General non-diabetic population (n = 2,774): 49.5 yrs | 10 yrs | HbA1c | Low | ||||
| Age range: 25–74 yrs | ||||||||||
| Larsen et al. (2014, Denmark) [61] | Cohort | Ca intake | Men and women (n = 7,569) | MONICA: 6 yrs | Body weight | Low | ||||
| MONICA (n = 1,329): 50.5 yrs | DCH: 5 yrs | Waist circumference | ||||||||
| Age range: 30.6–61.1 yrs | INTER99: 5 yrs | |||||||||
| DCH (n = 2,167): 53.0 yrs | ||||||||||
| Age range: 50.0–58.0 yrs | ||||||||||
| INTER99 (n = 4,073): 45.1 yrs | ||||||||||
| Age range: 34.7–59.8 yrs | ||||||||||
| Lorenzo et al. (2014, US) [65] | Cohort | Serum Ca concentration | African-Americans, Hispanics (n = 863) | 5.2 yrs | Type 2 diabetes | Low | ||||
| Non-Hispanic whites (n = 863) | ||||||||||
| Non-diabetes (n = 723): 54.4 ± 0.3 yrs | ||||||||||
| Diabetes (n = 140): 56.5 ± 0.7 yrs | ||||||||||
Ca, calcium; EAR, Estimated Average Requirement; RCT, randomized controlled trial; BMI, body mass index; WHR, waist-hip ratio; TSF, triceps skinfold thickness; SBS, subscapular skinfold thickness; AST, abdominal skinfold thickness; PUFA, polyunsaturated fatty acid; MONICA, MONItoring trends and determinants of Cardiovascular disease; DCH, Diet, Cancer and Health Study; SO, sarcopenic obese; SNO, sarcopenic nonobese; NSO, nonsarcopenic obese; NSNO, nonsarcopenic nonobese.
![]()
The relationship between Ca intake and growth in infants, toddlers, and adolescents were not consistent across studies (Table 4). There was no effect of Ca on growth in Tibetan children [7] and newborn [43]. However, Ca supplement was associated with an increase in adolescent growth [8], in which Ca and vitamin D supplementation had a positive effect on growth [44] and bone loss [38]. Milk consumption [45] and maternal Ca [46] were related to the growth of the fetus and children, respectively. These studies had several limitations to be considered as the evidence of EAR for Ca. Two RCTs studies were not double blinded and lacked detailed information on statistical analysis or Ca intake amount [744]. Three RCTs studies had a short supplementation period, and the number of the study participants was small [73843]. In one study, information on key factors related to growth such as physical activity, ultraviolet rays, vitamin D, and lean body mass was unclear or did not take account in the statistical model [8]. Two studies included specific participants, such as toddlers with food allergies [45] or infants of low-income mothers in their twenties [46].
In terms of cardiovascular disease, most studies showed that Ca supplements or dairy product intakes were negatively related to blood lipids [4748495051525354] (Table 5). However, Ca supplements used in some studies contained other nutrients, making it difficult to evaluate the effect of Ca itself on blood lipids or cardiovascular disease [47515253]. Several studies examined the effect of Ca on blood lipids by supplementation with Ca-rich supplements, not the dietary intake [4147525354]. In some RCT studies, there was no detailed information on the randomization process [5155]. Several cross-sectional studies could not examine the causal relationship between Ca intake and outcomes [4850]. One cross-sectional study had no information on drugs affecting Ca homeostasis, while one RCT study had a very short-term change (120 min) in blood lipid concentrations [54], and another RCT study examined participants with a more atherogenic lipid profile which would be more susceptible to saturated fatty acids, inducing increases in blood lipids and resulting in more-pronounced differences between diets [49].
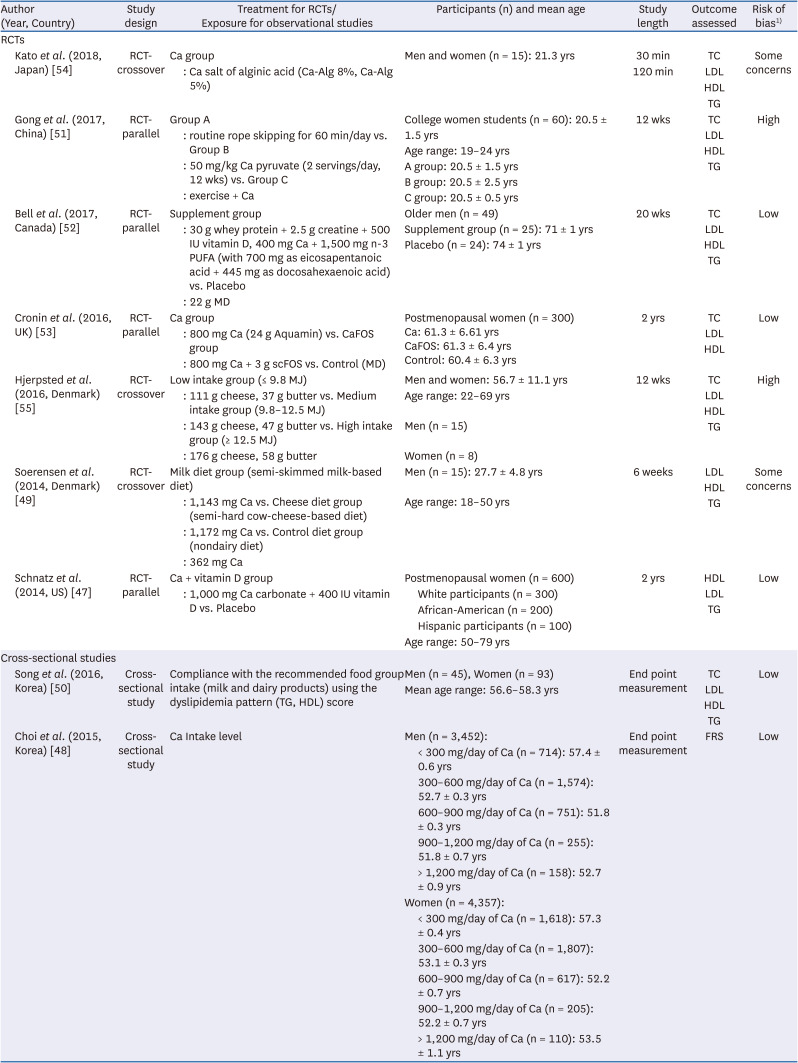
Table 5
Characteristics of the included studies examining the effect of Ca intake (EAR level) on cardiovascular diseases
| Author (Year, Country) | Study design | Treatment for RCTs/Exposure for observational studies | Participants (n) and mean age | Study length | Outcome assessed | Risk of bias1) | |||
|---|---|---|---|---|---|---|---|---|---|
| RCTs | |||||||||
| Kato et al. (2018, Japan) [54] | RCT-crossover | Ca group | Men and women (n = 15): 21.3 yrs | 30 min | TC | Some concerns | |||
| : Ca salt of alginic acid (Ca-Alg 8%, Ca-Alg 5%) | 120 min | LDL | |||||||
| HDL | |||||||||
| TG | |||||||||
| Gong et al. (2017, China) [51] | RCT-parallel | Group A | College women students (n = 60): 20.5 ± 1.5 yrs | 12 wks | TC | High | |||
| : routine rope skipping for 60 min/day vs. Group B | Age range: 19–24 yrs | LDL | |||||||
| : 50 mg/kg Ca pyruvate (2 servings/day, 12 wks) vs. Group C | A group: 20.5 ± 1.5 yrs | HDL | |||||||
| : exercise + Ca | B group: 20.5 ± 2.5 yrs | TG | |||||||
| C group: 20.5 ± 0.5 yrs | |||||||||
| Bell et al. (2017, Canada) [52] | RCT-parallel | Supplement group | Older men (n = 49) | 20 wks | TC | Low | |||
| : 30 g whey protein + 2.5 g creatine + 500 IU vitamin D, 400 mg Ca + 1,500 mg n-3 PUFA (with 700 mg as eicosapentanoic acid + 445 mg as docosahexaenoic acid) vs. Placebo | Supplement group (n = 25): 71 ± 1 yrs | LDL | |||||||
| : 22 g MD | Placebo (n = 24): 74 ± 1 yrs | HDL | |||||||
| TG | |||||||||
| Cronin et al. (2016, UK) [53] | RCT-parallel | Ca group | Postmenopausal women (n = 300) | 2 yrs | TC | Low | |||
| : 800 mg Ca (24 g Aquamin) vs. CaFOS group | Ca: 61.3 ± 6.61 yrs | LDL | |||||||
| : 800 mg Ca + 3 g scFOS vs. Control (MD) | CaFOS: 61.3 ± 6.4 yrs | HDL | |||||||
| Control: 60.4 ± 6.3 yrs | |||||||||
| Hjerpsted et al. (2016, Denmark) [55] | RCT-crossover | Low intake group (≤ 9.8 MJ) | Men and women: 56.7 ± 11.1 yrs | 12 wks | TC | High | |||
| : 111 g cheese, 37 g butter vs. Medium intake group (9.8–12.5 MJ) | Age range: 22–69 yrs | LDL | |||||||
| : 143 g cheese, 47 g butter vs. High intake group (≥ 12.5 MJ) | Men (n = 15) | HDL | |||||||
| : 176 g cheese, 58 g butter | Women (n = 8) | TG | |||||||
| Soerensen et al. (2014, Denmark) [49] | RCT-crossover | Milk diet group (semi-skimmed milk-based diet) | Men (n = 15): 27.7 ± 4.8 yrs | 6 weeks | LDL | Some concerns | |||
| : 1,143 mg Ca vs. Cheese diet group (semi-hard cow-cheese-based diet) | Age range: 18–50 yrs | HDL | |||||||
| : 1,172 mg Ca vs. Control diet group (nondairy diet) | TG | ||||||||
| : 362 mg Ca | |||||||||
| Schnatz et al. (2014, US) [47] | RCT-parallel | Ca + vitamin D group | Postmenopausal women (n = 600) | 2 yrs | HDL | Low | |||
| : 1,000 mg Ca carbonate + 400 IU vitamin D vs. Placebo | White participants (n = 300) | LDL | |||||||
| African-American (n = 200) | TG | ||||||||
| Hispanic participants (n = 100) | |||||||||
| Age range: 50–79 yrs | |||||||||
| Cross-sectional studies | |||||||||
| Song et al. (2016, Korea) [50] | Cross-sectional study | Compliance with the recommended food group intake (milk and dairy products) using the dyslipidemia pattern (TG, HDL) score | Men (n = 45), Women (n = 93) | End point measurement | TC | Low | |||
| Mean age range: 56.6–58.3 yrs | LDL | ||||||||
| HDL | |||||||||
| TG | |||||||||
| Choi et al. (2015, Korea) [48] | Cross-sectional study | Ca Intake level | Men (n = 3,452): | End point measurement | FRS | Low | |||
| < 300 mg/day of Ca (n = 714): 57.4 ± 0.6 yrs | |||||||||
| 300–600 mg/day of Ca (n = 1,574): 52.7 ± 0.3 yrs | |||||||||
| 600–900 mg/day of Ca (n = 751): 51.8 ± 0.3 yrs | |||||||||
| 900–1,200 mg/day of Ca (n = 255): 51.8 ± 0.7 yrs | |||||||||
| > 1,200 mg/day of Ca (n = 158): 52.7 ± 0.9 yrs | |||||||||
| Women (n = 4,357): | |||||||||
| < 300 mg/day of Ca (n = 1,618): 57.3 ± 0.4 yrs | |||||||||
| 300–600 mg/day of Ca (n = 1,807): 53.1 ± 0.3 yrs | |||||||||
| 600–900 mg/day of Ca (n = 617): 52.2 ± 0.7 yrs | |||||||||
| 900–1,200 mg/day of Ca (n = 205): 52.2 ± 0.7 yrs | |||||||||
| > 1,200 mg/day of Ca (n = 110): 53.5 ± 1.1 yrs | |||||||||
Ca, calcium; EAR, Estimated Average Requirement; RCT, randomized controlled trial; CaFOS, 800 mg of calcium with 3 g of short-chain fructo-oligosaccharides; scFOS, short-chain fructo-oligosaccharides; MD, maltodextrin; TC, total cholesterol; LDL, low density lipoprotein cholesterol; HDL, high density lipoprotein cholesterol; TG, triglyceride; MJ, megajoule; PUFA, polyunsaturated fatty acid; FRS, Framingham risk score.
![]()
Among studies reviewed for the relationship between Ca intake and blood pressure (Table 6), the effect of Ca intake on the decrease in blood pressure was more significant in women compared to men [49565758]; however, there were also results that did not show significant positive effects in both women and men [434953]. A cohort study found that the conjoint effects of serum Ca and insulin resistance at baseline on hypertension at follow-up [59].
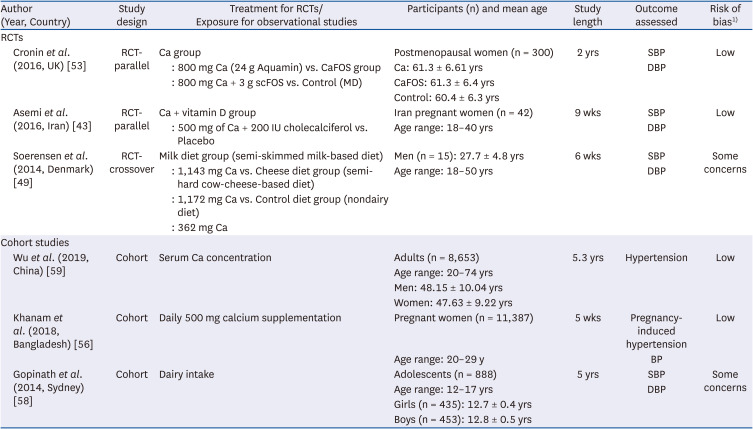
Table 6
Characteristics of the included studies examining the effect of Ca intake (EAR level) on hypertension
| Author (Year, Country) | Study design | Treatment for RCTs/Exposure for observational studies | Participants (n) and mean age | Study length | Outcome assessed | Risk of bias1) | ||
|---|---|---|---|---|---|---|---|---|
| RCTs | ||||||||
| Cronin et al. (2016, UK) [53] | RCT-parallel | Ca group | Postmenopausal women (n = 300) | 2 yrs | SBP | Low | ||
| : 800 mg Ca (24 g Aquamin) vs. CaFOS group | Ca: 61.3 ± 6.61 yrs | DBP | ||||||
| : 800 mg Ca + 3 g scFOS vs. Control (MD) | CaFOS: 61.3 ± 6.4 yrs | |||||||
| Control: 60.4 ± 6.3 yrs | ||||||||
| Asemi et al. (2016, Iran) [43] | RCT-parallel | Ca + vitamin D group | Iran pregnant women (n = 42) | 9 wks | SBP | Low | ||
| : 500 mg of Ca + 200 IU cholecalciferol vs. Placebo | Age range: 18–40 yrs | DBP | ||||||
| Soerensen et al. (2014, Denmark) [49] | RCT-crossover | Milk diet group (semi-skimmed milk-based diet) | Men (n = 15): 27.7 ± 4.8 yrs | 6 wks | SBP | Some concerns | ||
| : 1,143 mg Ca vs. Cheese diet group (semi-hard cow-cheese-based diet) | Age range: 18–50 yrs | DBP | ||||||
| : 1,172 mg Ca vs. Control diet group (nondairy diet) | ||||||||
| : 362 mg Ca | ||||||||
| Cohort studies | ||||||||
| Wu et al. (2019, China) [59] | Cohort | Serum Ca concentration | Adults (n = 8,653) | 5.3 yrs | Hypertension | Low | ||
| Age range: 20–74 yrs | ||||||||
| Men: 48.15 ± 10.04 yrs | ||||||||
| Women: 47.63 ± 9.22 yrs | ||||||||
| Khanam et al. (2018, Bangladesh) [56] | Cohort | Daily 500 mg calcium supplementation | Pregnant women (n = 11,387) | 5 wks | Pregnancy-induced hypertension | Low | ||
| Age range: 20–29 y | BP | |||||||
| Gopinath et al. (2014, Sydney) [58] | Cohort | Dairy intake | Adolescents (n = 888) | 5 yrs | SBP | Some concerns | ||
| Age range: 12–17 yrs | DBP | |||||||
| Girls (n = 435): 12.7 ± 0.4 yrs | ||||||||
| Boys (n = 453): 12.8 ± 0.5 yrs | ||||||||
Ca, calcium; EAR, Estimated Average Requirement; RCT, randomized controlled trial; CaFOS, 800 mg of calcium with 3 g of short-chain fructo-oligosaccharides; scFOS, short-chain fructo-oligosaccharides; MD, maltodextrin; SBP, systolic blood pressure; DBP, diastolic blood pressure; BP, blood pressure.
![]()
The effects of Ca intake on obesity, diabetes, and metabolic syndrome were not consistent (Table 7). Dietary Ca intake was not related to BMI [60] or waist circumference [61]. In elderly men, dietary Ca intake was related to sarcopenic obesity [62]. Ca supplement has a positive effect on body weight [51], lean body mass [52], and glycated hemoglobin (HbA1c) [63]. However, there was no effect [64] or a negative effect [65] of Ca supplement on blood glucose and diabetes. Ca intake from some dairy products had no effect on BMI [60], but had a positive effect on diabetes [6667]. Among these studies, one RCT study was not double-blinded and did not have detailed information on the randomization process or Ca intake amount [51]. Another RCTs study could not evaluate the effect of Ca itself [52]. There were studies that did not consider confounding factors related to Ca intakes, such as vitamin D intakes, PTH concentrations, fat contents of dairy products, growth status, or had dietary measurement errors [6063656667]. For several studies, the generalizability of results was limited [4961636466]. One cross-sectional study was limited to a causal effect of Ca intake [62].
Results of the systematic review for establishing the Ca UL
Results of individual studies from the literature assessment have been outlined in Table 8 according to health indicators in setting the Ca UL. The major health indicators reviewed in this study include kidney stones, ossification, bone health, calcinosis, hypercalcemia, and calculus.
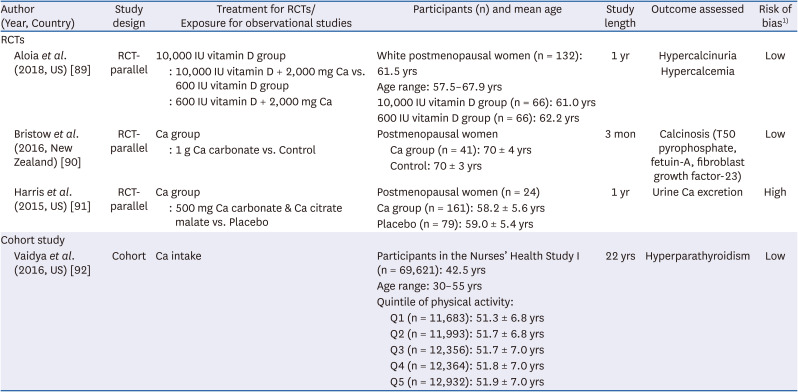
Table 8
Characteristics of the included studies examining the UL level of Ca intake
| Author (Year, Country) | Study design | Treatment for RCTs/Exposure for observational studies | Participants (n) and mean age | Study length | Outcome assessed | Risk of bias1) | |||
|---|---|---|---|---|---|---|---|---|---|
| RCTs | |||||||||
| Aloia et al. (2018, US) [89] | RCT-parallel | 10,000 IU vitamin D group | White postmenopausal women (n = 132): 61.5 yrs | 1 yr | Hypercalcinuria | Low | |||
| : 10,000 IU vitamin D + 2,000 mg Ca vs. 600 IU vitamin D group | Age range: 57.5–67.9 yrs | Hypercalcemia | |||||||
| : 600 IU vitamin D + 2,000 mg Ca | 10,000 IU vitamin D group (n = 66): 61.0 yrs | ||||||||
| 600 IU vitamin D group (n = 66): 62.2 yrs | |||||||||
| Bristow et al. (2016, New Zealand) [90] | RCT-parallel | Ca group | Postmenopausal women | 3 mon | Calcinosis (T50 pyrophosphate, fetuin-A, fibroblast growth factor-23) | Low | |||
| : 1 g Ca carbonate vs. Control | Ca group (n = 41): 70 ± 4 yrs | ||||||||
| Control: 70 ± 3 yrs | |||||||||
| Harris et al. (2015, US) [91] | RCT-parallel | Ca group | Postmenopausal women (n = 24) | 1 yr | Urine Ca excretion | High | |||
| : 500 mg Ca carbonate & Ca citrate malate vs. Placebo | Ca group (n = 161): 58.2 ± 5.6 yrs | ||||||||
| Placebo (n = 79): 59.0 ± 5.4 yrs | |||||||||
| Cohort study | |||||||||
| Vaidya et al. (2016, US) [92] | Cohort | Ca intake | Participants in the Nurses’ Health Study I (n = 69,621): 42.5 yrs | 22 yrs | Hyperparathyroidism | Low | |||
| Age range: 30–55 yrs | |||||||||
| Quintile of physical activity: | |||||||||
| Q1 (n = 11,683): 51.3 ± 6.8 yrs | |||||||||
| Q2 (n = 11,993): 51.7 ± 6.8 yrs | |||||||||
| Q3 (n = 12,356): 51.7 ± 7.0 yrs | |||||||||
| Q4 (n = 12,364): 51.8 ± 7.0 yrs | |||||||||
| Q5 (n = 12,932): 51.9 ± 7.0 yrs | |||||||||
![]()
There was no evidence on kidney stones, ossification, bone health, and calculus to consider the intake amount of Ca UL. Health indicators showing the detrimental effects of excessive Ca intake were calcinosis, hypercalcemia, hypercalcinuria, hyperparathyroidism, and urine Ca excretion. Only one RCT study in each health indicator was reviewed. Generally, studies could not separately evaluate the effect of Ca intake alone, and the generalization of the results was limited due to small sample size. Therefore, the evidence was not enough to apply the UL criteria.
DISCUSSION
We systematically reviewed literature published between 2008–2013 and 2014–2019 to assess the evidence in revising the KDRIs for Ca. Few studies of good quality were available for review. Most scientific evidence on bone health was reliable, but studies on other outcomes were weak or lacking. No balance studies or Ca absorption studies in Koreans were available in the years between 2014–2019. The changes in EAR and RNI in certain age groups were due to changes in the physical growth standards or rounding.
Habitual Ca intake of Koreans was considered in the 2020 KDRIs. The traditional Korean diet is low in Ca and change in dietary habits may be difficult. According to some revised calculations and rounding (as explained below), the EAR and RNI were subjected to increase in children and adolescents. However, the mean Ca intakes of Korean children and adolescents are far below those in the 2015 KDRIs, and an increase in the values for the 2020 KDRIs seemed unrealistic for public nutrition programs. Therefore, we rounded down the values resulting in similar values as those in the 2015 KDRIs. We recommend increasing the KDRIs for Ca in the future when mean Ca intake increases and approaching higher recommendations becomes realistically possible. However, due to the change in reference body size of older adults in the 2020 KDRIs, the calculated EARs and RNIs slightly decreased. The values were rounded up due to the increased risk of osteoporosis and fracture in this population and the higher rate of consumption of Ca supplements. The percentages of adults that consume Ca containing supplements and of those that reach the recommended intakes increases with age in adults, possibly due to the medical prescription of Ca supplements to prevent osteoporosis. The use of supplements may be the most practical method to adhere to the KDRIs in Koreans as habitual dietary Ca intake is low [6869]. Accordingly, the 2020 KDRI values for Ca did not change from those of 2015.
The KDRIs are established based on the assumption that other nutrients are appropriately consumed. However, in reality, the proper intake of some nutrients may be difficult to achieve. For instance, consumption of processed foods is increasing in Korea. Processed foods are generally high in sodium and phosphorus—2 nutrients that increase Ca excretion [70] when consumed in excess. Low Ca intake and high phosphorus and sodium intake can be detrimental to bone health in Koreans [12]. In particular, Korean adolescents have the highest EAR and RNI but the lowest intakes for Ca while consuming high amounts of sodium, possibly due to high intakes of processed foods [71]. This may negatively affect peak bone mass and increase the risk of osteoporosis and fracture in the later years of life. In addition, due to the decrease of outdoor social activities, increase of indoor activities, use of face masks during coronavirus disease 2019, and limited food sources of vitamin D, vitamin D deficiency may increase despite the already low vitamin D status of Koreans [72]. Low vitamin D status affects Ca metabolism and is associated with low BMD when Ca intake is also low. Therefore, appropriate intake of nutrients in addition to Ca is necessary, especially for Koreans, a population with low mean Ca intake.
As the literature search resulted in few reliable studies to revise the 2015 KDRI values, we thoroughly re-examined the basis of the previous KDRIs. The evidence of the recommendations in children and adolescents (ages 6–18 yrs) in the 2020 KDRIs were tailored to Asians as much as possible. When evidence in the Asian population was lacking but abundant in Whites within a specific age group, we used the mean of Whites and then averaged that with values in Asians in order to give more weight to Asians. In addition, for adolescents ages 12–14 and 15–18 yrs, balance studies were utilized to calculate the EAR and RNI [7374]. Regarding post-menopausal women, a 100 mg/day Ca increment to the calculated RNIs in women aged 50 yrs and older ensure public health protections and err on the side of caution in 2015 and was thus continued in 2020. As a result, the recommendations of the 2020 KDRIs for Ca did not change, but the scientific basis of the 2015 KDRIs was revisited and improved when determined necessarily.
Future research on the effect of Ca intake on non-skeletal outcomes, such as obesity, diabetes, hypertension, and cancer, is required. Small studies suggest a potential benefit of Ca on these outcomes [4951], but well-designed clinical trials are lacking. In pregnant and lactating women, recent evidence [38394041] in addition to those reviewed in 2015 [757677787980818283] indicates a possible need for additional Ca intake compared to that for non-pregnant or non-lactating women. Although the development of technical devices shows that BMD may recover after pregnancy or weaning, micro structures may remain deteriorated [84]. However, results are inconclusive, and more research must be conducted. Due to genetics, ability, and personal preferences, nutrition is not “one size fits all.” Studies have shown that the effect of Ca supplementation on bone may differ on the genotype of the VDR [39]. Our current knowledge on personalized nutrition is still developing. The US has launched Nutrition for Precision Health, powered by the All of Us research program [85].
Some research gaps specific to Koreans were additionally identified during the literature review. Despite decades of demand for clinical trials in Koreans, few have been performed. Studies on Ca balance, Ca absorption, Ca kinetics, and RCTs in diverse age groups are lacking among Koreans. To date, we were able to identify only one small balance study conducted decades ago in Korean children [86]. However, dietary pattern, nutrient intake, body weight, and height of children has drastically changed during the past decades, limiting its applicability. One balance and isotopic study were executed in the US, with a majority of participants being Korean American adolescents (specific ethnicity is not referred to in the manuscript, but the details are familiar as one author participated in the study) [87]. To our knowledge, apart from these 2 studies, most studies of the Korean population are observational, with a majority being cross-sectional. Furthermore, Ca supplement intake information is frequently omitted in observational studies. Another research gap is in pregnant adolescents, an increasing population in Korea [88]. Unlike the DRIs in North Americans, this dynamic life stage has not yet been accounted for in the KDRIs. In addition, nutrient requirements may differ between adult pregnancy and adolescent pregnancy as competition for essential nutrients between the growing adolescent and fetus may occur. A few Ca RCTs in pregnant adolescents are available in Whites but not in Koreans [3875]. Further clinical research in Korean pregnant females, including adolescents, is needed to be incorporated in future recommendations. Furthermore, the demand for personalized nutritional information is increasing in Korea as well. The KDRIs are utilized as public health guidelines; however, personalized approaches to nutrition may affect the shaping of the future KDRIs.
To conclude, despite a comprehensive review of the recent literature, we were unable to find high quality RCTs applicable in the 2020 KDRIs for Ca. Solid scientific evidence remains inadequate to set Ca requirements for outcomes other than bone health. Clinical trials in Koreans in diverse age groups and life stages may improve the quality of future recommendations.
 XML Download
XML Download